
Abstract
Background:
In Sweden, 4700 women seek bariatric surgery annually, many of those being nulliparous. Anovulation is common among obese women, but bariatric surgery is not considered a treatment for infertility. The aim of this study was to explore the motives of women in fertile age for seeking bariatric surgery and their expectations on future fertility.
Materials and methods:
A qualitative study with semi-structured interviews with childless women (n = 12) aged 20 to 35 years. Interviews were conducted 1 to 3 weeks prior to surgery, transcribed verbatim, and analyzed with thematic analysis.
Results:
“To get back on track” was identified as a master theme with 3 underlying subthemes, with the following headings: “A better me,” “A fertile me,” and “A pregnant me.” The participants were hoping that weight-loss would make them feel more content with themselves, break isolation, and make it easier to find a partner. The participants considered fertility to improve after bariatric surgery, mainly based on stories from other patients of bariatric surgery. Having a child was expressed to be of great importance to them.
Conclusions:
Even though obese young women do not seek bariatric surgery for fertility reasons alone, there is a general perception of enhanced fertility after surgery, which is regarded as positive and important.
Introduction
Obesity is an increasing health burden, with 40% of Swedish women aged 30 to 44 years reporting overweight or obesity, and 14% being obese. 1 After failed conservative weight-loss, annually, around 570 women aged 20 to 35 years seek bariatric surgery in our area in the south of Sweden of 1.2 million inhabitants.
Laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy are 2 surgical treatments used for morbid obesity, and both give a loss of around 80% of excess body weight, ie, weight exceeding a body mass index (BMI) of 25 kg/m2 in 12 to 18 months. 2
Menstrual irregularities and anovulation are common in obese women, 3 leading to a 2-fold time to pregnancy. 4 Obese women going through nonsurgical weight-loss have shown improved fertility outcomes, 5 and bariatric surgery improves underlying conditions such as menstrual dysfunction and factors that underlie fertility and pregnancy outcomes. 6 Positive effects of bariatric surgery on postoperative pregnancies are reduced risks of gestational diabetes and excessive fetal growth. Negative effects are shorter gestation, an increased risk of small for gestational age infants, and possibly increased infant mortality. 7 Female sexual dysfunction, common in women before bariatric surgery, resolves after surgery,8,9 which also is associated with changes in relationship status. 10
Previous qualitative studies indicate participants’ expectations of “normality,” 11 with the “tipping point” for the decision to proceed with bariatric surgery being own worsening health issues and low energy levels limiting activities 12 —still a decision not easy to be made. 13
Many women lack knowledge about fertility and generally overestimate the success rate of assisted reproductive technologies.14,15
Little is known about the presurgery experiences and expectations of young women in the context of reproduction.
The aim of the current study was to explore the motives behind young women’s wish to go through a major surgical procedure and their expectations on future fertility.
Materials and Methods
Participants
From a single center in Malmö, Sweden, women without previous children, aged 20 to 35 years, with Swedish language and accepted for bariatric surgery (both public- and private-funded) were identified by the research nurse (I.S.) and consecutively invited to the study from April 2016 through March 2017 (see Figure 1).
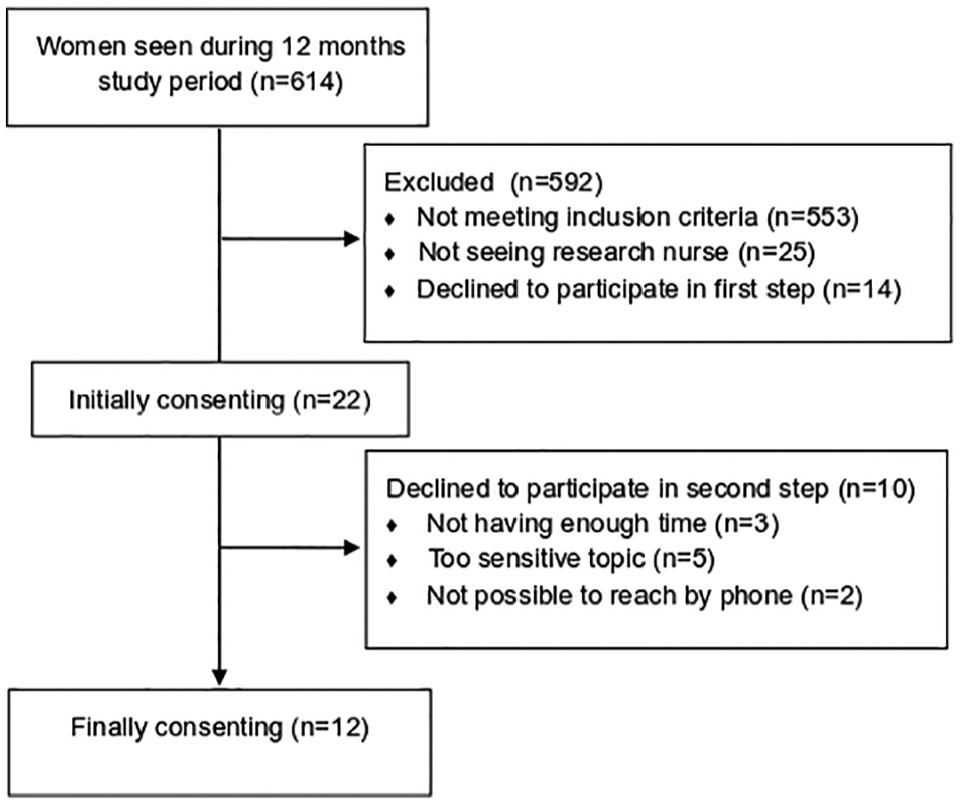
Recruitment of participants.
Patients eligible for publicly funded surgery should have an obesity duration of >5 years and BMI >40 or BMI >35 with one or more comorbidity. Privately funded bariatric surgery is offered to patients with BMI >30 and at least one serious attempt to weight-loss. Participants’ characteristics are shown in Table 1.
Participants’ characteristics.

One woman had both a legal abortion and a miscarriage in her history.
Data recording
As part of practice at the bariatric center, all patients filled out the questionnaires Short Form 36 (SF-36) and the Obesity Problems scale (OP-9) at their first visit, where anthropometric data also were obtained. In addition to being added to the hospital records, results were stored together with some demographic data in the Scandinavian Obesity Surgery Registry (SOReg). 16 The SF-36 is a validated generic instrument for measuring quality of life (QoL), independently of underlying conditions; measurements are divided into domains representing various aspects of life. Values from these domains are then joined together into 2 compound scores, physical and emotional; higher values in the test indicate a better QoL. 17 The OP-9 scale is a psychometrically valid disease-specific instrument designed to measure obesity-related problems in 9 different domains; a higher value indicates more obesity-related problems. 18 These questionnaires provided background information on participants for comparison with the reference group scheduled for surgery (see Table 2).
Comparison of participants with reference group.

Abbreviation: BMI: body mass index.
Values for reference group based only on patients with complete questionnaire data.
Statistics
Questionnaire data were retrieved from the SOReg central registry and analyzed using WinSTAT for Excel (R. Fitch Software, Cambridge, MA, USA). Mann-Whitney U test was performed as normal distribution could not be presumed; the level for statistical significance was set at a P value of <.05.
Recruitment
Recruitment was in 2 steps. First, an invitation letter including a written consent to participate was handed out by our research nurse (I.S.) to women (n = 22) who fulfilled inclusion criteria at the scheduling visit at the bariatric center. Second, these women were contacted individually by telephone by the first author (E.N.C.) 1 week afterward; this provided an opportunity for the potential participants to ask questions and to book place and time for an interview (see Figure 1). Twelve women finally agreed to participate.
Written informed consent was obtained from all participants. The study was approved by the Ethics Review Board in Lund (# 2016/50).
Interviews
Interviews were conducted either at the hospital or, if the participants so preferred, in their own home. The semi-structured interview guide, developed by E.N.C. and S.J., covered the following topics: decision-making to have bariatric surgery, psychological aspects on reproduction, fertility, expectations on surgery and future fertility, and information (see Supplemental Material 1). The lengths of the interviews were 38 to 95 minutes (mean: 54 minutes). All interviews were recorded and transcribed verbatim.
Data analyses
The interview material was analyzed inductively using thematic analysis, in accordance with the methods of Braun and Clarke. 19 This method was chosen because the approach was explorative, with the aim of increasing knowledge about individual expectations and motivations. First, the authors individually familiarized themselves with the data by reading the interviews, and then E.N.C., S.J., and I.S. were noting their first impressions. The analyses were then made in group by E.N.C., a clinical doctor working at a fertility center with previous experience of overweight and obese infertile women; S.J., a psychologist from another fertility center with previous experience of qualitative research; and I.S., a research nurse at the bariatric center and the only one with a clinical relationship to the participants. ATLAS.ti 8.2.34 was used to facilitate the manifest analysis. The first author created 35 diverse initial codes (see an example of the coding in Figure 2). Thereafter, E.N.C., I.S., and S.J. organized these into 4 broad themes: (1) better self-image, (2) gynecological health, (3) healthy pregnancy, and (4) emotional aspects, with a total of 17 underlying categories. In the next stage of the analysis, the 4 themes were restructured into 3 main themes: (1) “A better me,” (2) “A fertile me,” and (3) “A pregnant me,” which in total had 11 subcategories. After this, E.N.C. and S.J. worked together on the model and the authors agreed on a final understanding of the themes and subcategories shown in Figure 2.

The data analysis: example of coding organized into subcategories, main themes, and master theme.
Results
To get back on track was identified as a master theme, affecting the 3 underlying main themes, see Figure 2. The quotations presented are identified by a number indicating participant (1-12).
To get back on track
All participants had decided to go through surgery because they wanted to achieve a change in their lives. Having struggled with different weight-loss methods, they described how obesity affected all parts of their lives. They wanted to get rid of these difficulties, as well as the risks associated with obesity. All participants knew that surgery involved risks, but rather looked forward to the possibilities that might come with the weight-loss. Independently of having previous experience of not being obese, the participants expressed how they wanted to return to normality, describing obesity as an obstacle to move forward with their lives and to have a family: I want to get back on my feet first and I want to be comfortable with my body before I . . ., I look at it this way, that if I’m not content then I can’t be a role model to my child. . . . Because they see more than you think. I’d rather be done there. I am dreaming of having children, but it’s just not now. (Participant 8)
A better me
The participants described a feeling of how life was set on pause since they had become obese. They talked about being inhibited both psychologically and physically, and that this would turn back to normal when they lost weight, described as “the real me” is in there, somewhere: Like, I’ve always had this ideal body, that I don’t want to be super skinny, not at all, but a bit chubby, like, still having the curves. I don’t like to be the way I am now, for example, that I’m like, overweight. . . . I’ve got an ideal body. It’s just hiding, somewhere in here, right now. (Participant 3)
Self-image
Several of the participants described a feeling of being alienated from themselves. Looking in a mirror or at a photo, they did not recognize the “other” person that they had become with the overweight: Yeah, kind of. I’m feeling like a stranger, almost, like, in my own body. Because I still see myself as the size I used to be, like, when I went to high-school, in the beginning of high-school before things started to slip. I’ve even kept clothes, as if, from back then, because that’s like, the size I’m supposed to be, and that really wasn’t slim but more the way I was comfortable. (Participant 4)
Self-esteem
Obesity negatively affected self-esteem. Milder psychiatric problems, such as anxiety and depression, were self-reported by 8 participants which connected these problems to obesity. They were at the same time hoping that surgery and the following weight-loss would affect them also psychologically, in a positive way: I mean, I can go out and see people, but I kind of get stomach aches and I feel real sick, but it is possible, I mean, I do survive. ‘Cause before I met her (the CBT therapist) I couldn’t, but then I had both lost some weight and got some of my self-esteem back. I guess I think it’s difficult to tell if it depends on the weight or the self-esteem, but I think both go hand in hand in my case. (Participant 12)
Relationships
The majority described the stigma of being obese, and that they already “knew” what others were thinking about them. This was holding them back from going out and building new relationships, which led to isolation. Losing weight was considered as a means to be more outgoing, being able to be more open to new relationships: Well yes, if you consider the “love-part” I think it could affect in a positive way, hopefully then, erh . . . since I don’t have a lot of people around me, but the ones I have are very close, erh, and it might also affect friendships positively. Because it feels like I have lost many since I myself have withdrawn. (Participant 9)
Some of the participants discussed that this might be a threat to existing relationships, for example, with their current partner: Then, when I said that I had applied for this kind of operation, he let this one slip: “but then you’re gonna . . ., then you might dump me when you become . . .” and I just; “when I become what?,” I said. “Don’t finish that sentence now ’cause then you’ll get a hell, so to speak. Do you think I’m with you because it’s like, some sort of a consolation prize.” (Participant 1)
Sexuality
Although nobody reported that they had received any explicit negative comments on their bodies in a sexual content, sexual desire was inhibited by their own thoughts of how their bodies would look in a sexual situation: And about sex life and so on . . ., it’s ugly, you must have a nice body. (Participant 11)
Losing weight was described as a means to get more confident in a sexual situation, and they were hoping that they would be more relaxed in their sex life: Better. I mean I think it’s gonna . . ., I mean I think . . ., ‘cause I think . . ., I think that then you might dare to take more initiatives, too. If you’re comfortable with your body, then I guess it’s more that you take what you want. So, I suppose it’s gonna . . . Because it’s like that, that if you’re feeling self-confident then everybody else is noticing as well. (Participant 12)
Not an easy way-out
Many of the participants were somewhat worried about what other people would think of their going through the operation, as “taking the easy way-out.” For themselves it was not an easy choice, but rather something that they had been thinking about for years before taking the step. It was considered their last, but maybe not only, choice: I really enjoy being active so that’s not the problem. To me, it’s the food. Erh, and then I just got to that point when I felt like, that you don’t get any younger. Look, I do not care about getting older, like I’m 28 now, but it’s not getting easier and I’ve looked things up and I don’t think having a gastric bypass is taking the easy way, I rather see it as the last resort. (Participant 1)
A fertile me
There was great awareness of the negative effects of obesity on female fertility. Gynecological problems such as polycystic ovary syndrome, menstrual irregularities, and endometriosis were spontaneously mentioned as contributing to the urgency of losing weight. The participants considered obesity to be the most probable underlying mechanism to these problems. For most of the participants, the main purpose of the operation was not to achieve pregnancy, but all of them saw the picture of improved possibilities to get pregnant as another positive and important part of having bariatric surgery: Yeah, like I told you, that when you lose weight you get your period and then when you get your cycle going and, like, regular then you’ll have a baby. You can have children. That’s no problem. (Participant 11)
Gynecological problems
Several participants described irregular menstrual periods and hormonal problems as the underlying mechanism to their weight-gain. They also had great expectations on that weight-loss would regularize their cycles and improve their hormonal balance: I have PCOS and so on, which led to my overweight. I gained 35 kg and noticed that something had to be wrong. So, I went to the Youth Service and she started to suspect that it was PCOS, but I was referred to the gynecologist to see and then they almost instantly confirmed that. We got to see the picture and there were a lot of cysts and then I gained, like, another 20-25 kg after that. So, it all happened very fast. In a few years I gained a lot of weight, since it started. (Participant 4)
To achieve pregnancy
Most of the participants pointed out the irregular menstruations caused by obesity as the greatest obstacle to get pregnant: . . . since I have not succeeded to get pregnant and I think it depends a lot on my weight. (Participant 7)
Several of them also had knowledge about the negative effects of obesity on pregnancy and mentioned the increased risk of miscarriage: No, but really, you never know why you have a miscarriage. That is . . ., it’s like you could never really know, but I’m also aware that you’re more likely to have a miscarriage and so on, if you’re overweight. (Participant 12)
To qualify for pregnancy
Of the participants who were in a relationship, 2 had already found out that they needed help from hormonal stimulation, in vitro fertilization (IVF), or insemination, and another 2 with a history of infertility had also been considering fertility treatments. Because there are BMI limits in the publicly funded IVF clinics, the operation was also seen as a mean to qualify for treatment: And then me and my partner want to have children. Then first you must live together for a year, I think it is, it used to be two, I’ve heard. So, we can apply for it now, but it’s no use trying to apply since I’ve got to get below BMI 30 to have an insemination or IVF. (Participant 4)
A pregnant me
All participants described a wish of having children in a more, or less, close future, and that having a family was very important to them. None of them had heard anything negative about pregnancies after bariatric surgery: No. And I know that it really doesn’t stop you to get pregnant. . . . So that’s why I don’t consider it any problem. Because I know that you still can get pregnant. Yes. . . . Because otherwise . . ., like if I couldn’t get pregnant . . . then I ’d never have the surgery. Because that’s my biggest dream in life. That’s just having children. So . . . (Participant 12)
A healthy pregnancy
The participants knew that obesity causes high-risk pregnancies, and that this meant a risk for mother as well as child. Participants also mentioned that pregnancy could lead to extra weight-gain which might put them in an even worse situation: And then I went to get new birth control pills and then I was talking a bit with the midwife and then she actually said that it would be danger . . ., that it could be dangerous to both of us, the fetus and me, if I got pregnant because of the obesity so to say. So, I guess it would be a lot easier if I lost weight. I really don’t want it to be dangerous neither to me nor the baby if I get pregnant. (Participant 2)
Pictures of pregnancies after bariatric surgery
None of the participants were worried that bariatric surgery would affect future pregnancies negatively. Some of them were reflecting on the possibility that the fetus would suffer from lack of nutrients, but the fact that friends and family members who already had gone through the operation had delivered successfully afterward was encouraging enough: We were discussing a bit, me and my cousin then and another friend who also had had the surgery, that since you can’t eat that much, I mean I myself, so that the baby can get sufficient nutrition and so on, but since others who had the surgery have managed well, so probably the baby gets sufficient nutrition, it seems so, erh, that’s probably the only thing I’ve really considered . . . actually. (Participant 7)
A healthy parent
The thought of having a family also meant a dream of being an active parent, the opposite of what several of them had experienced themselves. Several reflected over self-esteem, and how your own self-esteem affects your children: I’m thinking a bit ahead. My parents really were, like I said, both of them, huge before, but they have lost weight and it took them a life-time so I’m scared that it’s like, going to take a lifetime and then . . . before something happens, and I don’t want that. While I am still young . . ., yes. I still haven’t had children yet and, like, all that stuff. Because they were like, real big when we were . . ., when they had us too, me and my sisters. And then . . ., erh, they haven’t had the energy to be as active as maybe other parents have been and so on and I don’t want that, if I’d be a mum one day. (Participant 10)
Discussion
Our study highlights that one of the underlying motivators of childless young women to go through bariatric surgery is to regain fertility. The master theme To get back on track can be seen as the hope that all of the participants had in common that surgery would improve their lives in several areas, not only physically. In accordance with Wysoker 13 several of the participants described surgery to be the last resort. This, as well as findings of low self-esteem and social avoidance, has also previously been reported by Homer et al 11 and can be connected to pressure on today’s young women from established norms and picturing in media; there is evidence that awareness of ideal standards can adversely affect self-esteem among women, regardless of their actual body weight and shape. 20 Young women, indeed, are a vulnerable group, with Swedish data showing the highest frequency of self-reported mild or severe anxiety and hospitalization due to self-injury. 21
The 3 themes found in our analysis all interact; to go on with their lives, To get back on track, was influenced by the 3 subthemes as what they wished for their future. Among our participants, a couple focused on other physical comorbidities that seemed to represent the “tipping point” 12 to choose surgery, but during the interviews, the return to A better me and A fertile me seemed just as or even more important. To many young women, the wish to return to normality 11 also mean building a family, 15 and all of the participants could see themselves as a parent in the future. They had expectations on getting more active and outgoing, which might lead to a relationship for the participants who were single. Among the participants, there was a strong belief that bariatric surgery enhances fertility, based on stories from family, friends, and acquaintances fortified by the information given from the bariatric center that fertility might be regained when menstrual irregularities dissolve. Half of the participants had previous experience of difficulties to conceive. It was their own conclusion that obesity was the cause, sometimes supported by health care professionals. A previous study 22 on motivation to seek bariatric surgery stated the importance of other bariatric surgery patients, health professionals’ recommendations, and media. Our participants described positive pictures of pregnancy from other bariatric surgery patients as their primary source of information. They had not much knowledge of possible risks in pregnancies after bariatric surgery and had not received any information on this subject from health care professionals. These are new findings that need to be confirmed in other studies.
To the best of our knowledge, this is the first qualitative study providing insight into morbidly obese childless young women’s broader expectations on childbearing, relationships, fertility, and future pregnancy. The participants represent the Swedish population ethnically well, with a wide range of fertile age. After 12 interviews, no new themes emerged, and data saturation was considered being reached. The main limitation is regarding which patients who accepted to participate. As sexuality and fertility could be sensitive topics, selection bias cannot be excluded. This was, however, a qualitative hypothesis–generating study, and the participants were representative of the reference group in terms of anthropometric data, obesity problems, and QoL. A quantitative approach using questionnaires, on the other hand, might be susceptible to bias related to eligibility for surgery. Patients are aware of the criteria to qualify for bariatric surgery, and when asked for the reason to choose bariatric surgery, the accepted comorbidities were the participants’ first answers. The use of the semi-structured interview technique allowed us to get in-depth data on the participants’ life situation, psychosocial well-being, and their thoughts regarding future childbearing as well as previous information, and its source. Using thematic analysis which minimally organizes and describes your data set in (rich) detail, 19 we could extract how expectations on fertility influenced the participants’ decisions to go through surgery. The interviews and analyses were conducted by a gynecologist, and to reduce the risk of researcher bias, the analyses were performed together with a psychologist working in a fertility clinic and a nurse from the bariatric surgery center.
Our group was heterogeneous regarding previous experience of pregnancy and self-reported infertility, as well as in most other demographic aspects. The sample can thus be reasonably representative of surgery-seeking obese women in the age group of 20 to 35 years in Sweden, but findings might not apply to women in other regions though. Findings might also change over time, and follow-up studies are necessary.
In Sweden, BMI limits varying of <30 to <35 apply to the admission to subsidized IVF treatment. American College of Obstetricians and Gynecologists stated in 2009 that bariatric surgery should not be considered a treatment for infertility 23 and lifestyle modification is considered first-line treatment. 24 As this might take time, there is a risk that other causes for infertility might remain occult, and thereby prolonged time to infertility treatment needed. Our study shows that among patients there are high expectations on bariatric surgery as a resolution to obesity-related infertility.
Conclusions
Obese childless women seeking bariatric surgery have high expectations on future childbearing, considering the operation as a means to come back to a normal life including improved fertility.
Supplemental Material
Nilsson-Condori_xyz2479469f4f0e4 – Supplemental material for To Get Back on Track: A Qualitative Study on Childless Women’s Expectations on Future Fertility Before Undergoing Bariatric Surgery
Supplemental material, Nilsson-Condori_xyz2479469f4f0e4 for To Get Back on Track: A Qualitative Study on Childless Women’s Expectations on Future Fertility Before Undergoing Bariatric Surgery by Emma Nilsson-Condori, Stina Järvholm, Ann Thurin-Kjellberg, Ilona Sidlovskaja, Jan L Hedenbro and Britt Friberg in Clinical Medicine Insights: Reproductive Health
Supplemental Material
Nilsson-Condori_xyz24794b45719bc – Supplemental material for To Get Back on Track: A Qualitative Study on Childless Women’s Expectations on Future Fertility Before Undergoing Bariatric Surgery
Supplemental material, Nilsson-Condori_xyz24794b45719bc for To Get Back on Track: A Qualitative Study on Childless Women’s Expectations on Future Fertility Before Undergoing Bariatric Surgery by Emma Nilsson-Condori, Stina Järvholm, Ann Thurin-Kjellberg, Ilona Sidlovskaja, Jan L Hedenbro and Britt Friberg in Clinical Medicine Insights: Reproductive Health
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research grants from the Hjalmar Svensson Foundation and the Swedish Government Funds for Clinical Research.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Design of the study: ENC, SJ, JLH, ATK, BF. Enrolment of patients: IS, ENC. Thematic analysis: ENC, SJ, IS. Statistical analysis: ENC and JLH. Interpretation of data, writing of the article and approval of the present version: ENC, SJ, ATK, IS, JLH, BF.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.