
Abstract
Severe combined immunodeficiency (SCID) is a group of diseases characterized by low T-cell count and impaired T-cell function, resulting in severe cellular and humoral immune defects. If not diagnosed and treated promptly, infants affected by this condition can develop severe infections which will result in death. Delayed treatment can markedly reduce the survival outcome of infants with SCID. T-cell receptor excision circle (TREC) levels are measured on newborn screening to promptly identify infants with SCID. It is important for primary care providers and pediatricians to understand the approach to managing infants with positive TREC-based newborn screening as they may be the first contact for infants with SCID. Primary care providers should be familiar with providing anticipatory guidance to the family in regard to protective isolation, measures to minimize the risk of infection, and the coordination of care with the SCID coordinating center team of specialists. In this article, we use case-based scenarios to review the principles of TREC-based newborn screening, the genetics and subtypes of SCID, and management for an infant with a positive TREC-based newborn screen.
Keywords
Introduction
Severe combined immunodeficiency (SCID) is a group of genetic diseases characterized by a severe impairment of both cellular and humoral immune defenses. In the US, the incidence of SCID is 1 in 58 000. 1 Infants with SCID are typically asymptomatic at birth and early infancy due to the protective effect of maternal antibodies, as well as minimal exposure to pathogens. However, when failure to thrive starts to occur and maternal antibodies fall at around 4 to 6 months of age, patients with SCID can develop severe recurrent infections and death by 1 to 2 years of age if not promptly managed. 2 These infections range from common bacterial and viral infections to rare opportunistic infections such as Pneumocystis jirovecii, and other fungal and mycobacterial infections. Infants with SCID can also present with chronic diarrhea and failure to thrive. The curative treatment of SCID is hematopoietic stem cell transplantation (HSCT), which yields the best 5-year survival outcome of 94% in infants who receive transplants before 3.5 months of age. In contrast, the survival outcome drops to 50% in infants who receive transplants after 3.5 months of age and with active infection. 3 Therefore, early diagnosis and prompt management of patients with SCID prior to the development of infections are very critical. Population-based screening was implemented in all 50 states of the US, as well as several other countries, to detect newborns with SCID early, provide timely diagnosis, infection protection measures, and prompt management.
A full-term female infant was born via spontaneous vaginal delivery without complications. Routine postnatal newborn care was completed. A dried blood spot was sent for newborn screening at 24 hours of life. She was clinically well and was discharged home with her mother after 24 hours of life. Her parents denied consanguinity but reported the same country of origin. They also recalled a family history of early infant deaths. At 96 hours of life, the newborn screen reported a positive SCID screen with an undetectable T-cell receptor excision circles (TREC) level. She was referred to the immunologist for further evaluation and management. Due to the absent TREC level in a seemingly well newborn without other possible causes of secondary T-cell lymphopenia, SCID was highly suspected.
Newborn Screening for SCID
TRECs are circular pieces of DNA by-product formed by unused DNA fragments during the V(D)J recombination process of T-cell receptors (TCRs). They are stable and unable to replicate with further cell division, making them an ideal biomarker of thymic production of naïve T-cells. 4 TREC newborn screening was first proposed by Chan and Puck in 2005 to develop a population-based screening by measuring extracted DNA from infant dried blood spots by real-time polymerase chain reaction (PCR). 5 The test was first piloted in Wisconsin in 2008 and was added to the recommended uniform screening panel (RUSP) by the US Department of Health and Human Service Secretary’s Advisory Committee on Heritable Disorders in Newborn and Children (SACHDNC) in 2010. 6 By the end of 2018, the test was implemented in the newborn screening program by all 50 states of the USA, as well as Washington, DC and Puerto Rico. 7 A low TREC level signifies insufficient naïve T-cells, which is one of the key features in infants with SCID, but can also be found in other conditions that cause T-cell lymphopenia. 6 TREC screening for SCID fits the criteria for newborn screening as SCID is a major health condition with high mortality if untreated. The available treatment modalities for SCID yield significantly better outcomes if given early. The test is sensitive and predicted to be cost-effective despite the low incidence of the disease. 8 Furthermore, the specific confirmation tests and curative treatment are available after a positive screening and a confirmed diagnosis. 6
Genetics, Lymphocyte Phenotypes and Clinical Manifestations of SCID
Newborns with SCID may be clinically well at birth and present initially with an abnormally low TREC level on newborn screen. In typical SCID cases, confirmatory test with flow cytometry reveals a CD3 T-cell count that is lower than 50 cells/μL, and absent or very low T-cell function, which is demonstrated by <10% of the lower normal limit of response to phytohemagglutinin (PHA), a commonly used mitogen of T-cell proliferation. 9 Typical SCID can be classified based on lymphocyte phenotypes, as shown in Table 1.9-14 The most common molecular defect is IL2RG mutation, 3 which presents with a T-cell negative, B-cell positive and NK-cell negative (T-B+NK-) phenotype. The IL2RG gene encodes the gamma chain of interleukin receptors for IL-2, IL-4, IL-7, IL-9, IL-15, and IL-21. As IL-7 provides survival and proliferative signals for early T-cell development, defects in this gene lead to profound defects in T lymphocyte count and function (T-cell negative phenotype). Furthermore, as IL-15 is important for NK cell development, the mutation leads to deficiency in NK cells. The IL2RG gene is located on Xq13 and mutations in the gene can lead to an X-linked recessive disorder. 2 The classic symptoms of SCID, if not detected with the newborn screening prior to the symptom onset, include recurrent bacterial and viral infections, opportunistic infections, chronic diarrhea, and failure to thrive. The symptoms usually present several months after birth. Physical examination may reveal oral thrush and signs of focal infections. 15
Classification of SCID based on phenotypes of lymphocytes and common molecular defects.
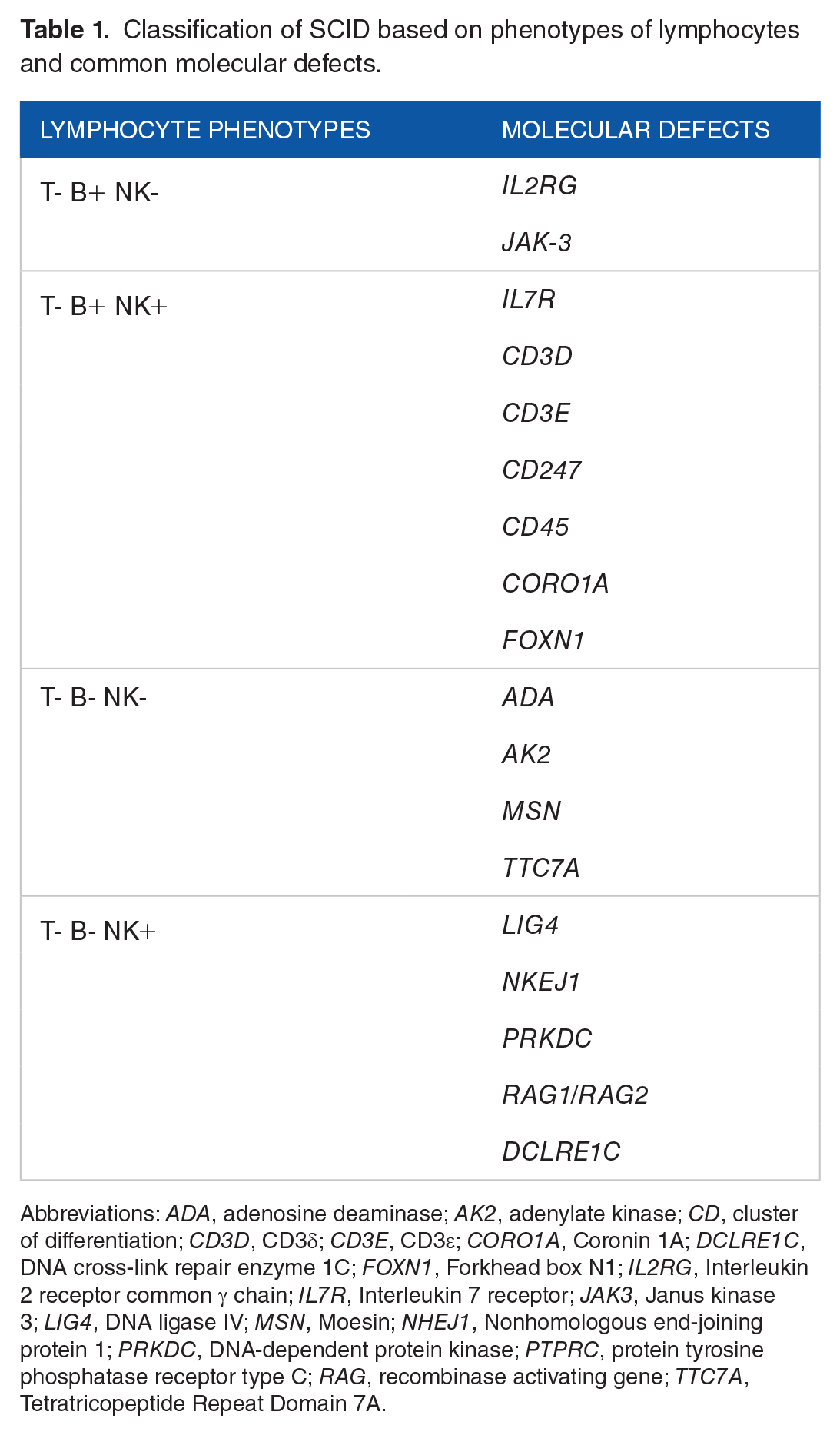
Abbreviations: ADA, adenosine deaminase; AK2, adenylate kinase; CD, cluster of differentiation; CD3D, CD3δ; CD3E, CD3ε; CORO1A, Coronin 1A; DCLRE1C, DNA cross-link repair enzyme 1C; FOXN1, Forkhead box N1; IL2RG, Interleukin 2 receptor common γ chain; IL7R, Interleukin 7 receptor; JAK3, Janus kinase 3; LIG4, DNA ligase IV; MSN, Moesin; NHEJ1, Nonhomologous end-joining protein 1; PRKDC, DNA-dependent protein kinase; PTPRC, protein tyrosine phosphatase receptor type C; RAG, recombinase activating gene; TTC7A, Tetratricopeptide Repeat Domain 7A.
Adenosine deaminase (ADA) deficiency is a form of SCID that is an autosomal recessive disorder. ADA is an enzyme that plays an important role in purine metabolism. Abnormal function of the enzyme results in the accumulation of toxic metabolites and causes premature lymphoid progenitor cell death, which leads to defects in both cellular and humoral immunity. Its phenotype is T-cell negative, B-cell negative and NK- cell negative SCID. Patients with ADA SCID can present with infections, chronic diarrhea, failure to thrive, as well as permanent damage of multiple organs including lungs, brain, skeleton, liver, and kidney due to the accumulation of toxic metabolites. 16 ADA deficiency accounts for 10% to 15% of the SCID cases in the US. 17 Approximately 15% to 20% of patients with ADA deficiency have late-onset immunodeficiency. At birth, they may have normal lymphocyte counts and normal TRECs due to maternal detoxification of toxic purine intermediates in utero. Since these patients may be missed by TREC newborn screening and have poor outcomes from delayed treatment, another screening test is needed to timely detect ADA deficiency. Thus, measurement of adenosine and 2′-deoxyadenosine levels by tandem mass spectrometry (TMS) to screen for ADA deficiency was added to the newborn screen in some states. 18
Some patients with milder forms of SCID may present later in life due to the ability to produce some T-cells. These conditions are termed leaky SCID or partial SCID, a combined immunodeficiency due to a hypomorphic mutation in any of the genes that are known to cause typical SCID. Although patients can produce some T-cells, normally 300 to 1500 cells/μL, their T-cell function is typically impaired. 2 Therefore, TREC newborn screening may not be able to detect leaky SCID patients with near-normal T-cell production.
Some patients with leaky SCID can present with Omenn syndrome, which is caused by oligoclonal autoreactive T-cell expansion due to hypomorphic mutations, most commonly the RAG1 or RAG2 gene, leading to clinical features that resemble graft-versus-host-disease (GVHD). Omenn syndrome is uniquely characterized by lymphadenopathy, hepatosplenomegaly, eosinophilia, elevated IgE levels, and generalized cutaneous manifestations such as erythroderma and exfoliative dermatitis. 19
Maternal T-cells engraftment occurs when alloreactive T-cells from the mother cross transplacentally. This condition is found in infants with SCID due to the absence of T-cells to eliminate maternal lymphocytes, causing materno-fetal GVHD. While unaffected newborns are expected to have a T-cell profile made up of roughly 90% naïve T-cell (CD45RA+ CD62L+), newborns with maternal T-cells engraftment have a predominance of memory T-cells (CD45RO+ CD62L−) on flow cytometry. The typical clinical presentation of maternal T-cells engraftment includes skin rashes and hepatic disease. 20
In patients with immunodeficiency, GVHD can also occur iatrogenically from blood transfusions, when viable T lymphocytes from donors are able to engraft and attack recipient organ systems. Clinical manifestations, including rashes, fever, liver enzyme elevation, diarrhea, and pancytopenia, typically develop between 4 and 30 days after a transfusion. 21 This condition can be prevented by gamma irradiation and leukoreduction with filters of blood products to eliminate viable lymphocytes.
Management of Infants With Positive SCID Screening
The reporting of positive newborn screening for TREC varies by states. Furthermore, each state varies in its referral and management of positive newborn screens for SCID. Regardless of the state’s protocol, all positive TREC screens should receive immediate attention. Generally, pediatricians, family medicine physicians, primary care physicians, primary care advanced practice practitioners, assigned clinic staff, or involved health care personnel of the birth hospital will receive a positive SCID newborn screening result with instruction for immediate consultation with a pediatric specialist. In some states, the positive results are reported to a team of SCID nurse coordinators and clinical immunologists designated by the state. In this case, primary care providers and hospitals where infants remain hospitalized may receive communication and guidance by the SCID coordinating team. This coordinating team will assist with further testing and referrals. In this case, primary care providers will be contacted by the team and will be provided further instructions for management. In the states where a SCID coordinating team is not assigned, primary care providers will be responsible for the coordination of care. 22 Communication with the family is a crucial process and will be provided by either the primary care provider and/or the SCID coordinating team. Studies reported parental anxiety, confusion, and stress upon receiving positive screening results.23,24 An optimum information should be given during the referral procedure, and a follow-up consultation should be provided. Communication scripts could help if primary care providers are allocated to do the first contact, as shown in Supplemental Figure 1. Parents should be informed that this is only a screening test, and the full evaluation and confirmation of diagnosis will be done subsequently at an outpatient visit which will be arranged either by the SCID coordinating team or primary care provider, specific to each state’s process. The confirmatory testing and immunologic assessment should be promptly and ideally should not be delayed for more than 2 weeks after a positive TREC result. 25 Either the SCID team or primary care provider will teach family the precautions necessary while waiting for confirmatory testing. Resources are available to help families understand positive newborn screening for SCID, as listed in Supplemental Figure 2.
Additional Investigation for Diagnosis of SCID
Flow cytometry
It is important to note that the TREC assay is only a screening test, and a confirmatory test is required for the diagnosis of SCID, similar to other diseases that are screened at birth.
Determining the number of lymphocytes by flow cytometry is the initial investigation used to evaluate infants with positive TREC newborn screening to confirm T cell lymphopenia. The distribution and absolute value of T, B, and NK lymphocytes is required for accurate diagnosis of SCID phenotypes. If maternal T-cells engraftment is suspected, flow cytometry for naïve (CD45RA+ CD62L+) and memory (CD45RO+ CD62L−) T-cells should also be performed to distinguish maternal T-cells from infant T-cells. This is especially important in patients with leaky SCID where T-cells are detected.
Complete blood count (CBC)
CBC with differentiation may be used to assess the number of lymphocytes in infants with positive TREC screening. Patients with SCID will most likely have a low absolute lymphocyte count as two-thirds of total lymphocytes are T-cells. Low absolute lymphocyte count indirectly reflects T-cell lymphopenia. If the absolute lymphocyte count is normal, it can be reassuring that the infant is unlikely to have SCID and alternative causes of T-cell lymphopenia triggering an initial positive TREC screen should be considered. However, it is important to keep in mind that low absolute lymphocyte count on CBC is not specific to SCID alone. Additionally, patients with maternal T-cell engraftment and leaky SCID with Omenn syndrome can have normal or high lymphocyte counts. 7
Additional immunology testing
The lymphocyte proliferation assay is an in vitro test to measure peripheral blood T-cell proliferation showing the level of T-cell function. T-cell proliferation occurs in response to stimuli such as mitogens, most commonly phytohemagglutinin (PHA). In patients with typical SCID, lymphocyte proliferation may be very low or absent due to the presence of very low to absent number of T-cells. In leaky SCID, impaired lymphocyte proliferation may be seen even though T-cell numbers are adequate. 15 On the contrary, if the lymphocyte proliferation is normal in response to stimuli, the diagnosis of SCID is highly unlikely.
Quantitative immunoglobulin levels may also be helpful and indirectly reflect adaptive immune function. IgG levels in newborns are affected by maternal IgG and will not be as helpful for diagnosing SCID. IgM does not cross the placenta, so IgM values are reflective of the infant’s own IgM levels. Absent or very low IgM levels are usually observed in infants with SCID. IgA levels can be physiologically low in infants and the presence of low IgA does not necessarily indicate SCID. On the contrary, normal levels of IgM and IgA levels can be reassuring.
Genetic testing
To obtain the molecular diagnosis, a variety of genetic testing is available, including Sanger sequencing, chromosomal microarray analysis, targeted gene panels, and whole exome sequencing. 26 Genetic testing is helpful to determine SCID subtypes, to identify the type of lymphocyte dysfunction, to aid in selecting treatment modalities and transplant protocols, as well as genetic counseling for the family. However, the identification of known pathogenic genes is not necessary for the diagnosis of SCID.
Since SCID was suspected, laboratory testing including CBC with differential counts, flow cytometry, lymphocyte proliferation assay, and a genetic testing panel for SCID were sent. CBC reported lymphopenia, with an absolute lymphocyte count of 1400 cells/μL (3500-14 000 cells/μL). While waiting for the results of the confirmatory tests, her parents were counseled about infection prevention measures.
Prevention Measures
Isolation measures
Infection is associated with poor HSCT outcomes in patients with SCID.3,27 Parents should be advised to place the infant in protective isolation and strictly prohibit visitors and social gatherings, especially from other young children who may inadvertently carry infections from school. Household members must be taught universal precautions and strict hand hygiene measures to avoid the risk of infections. Parents should also avoid social events as they could bring home transmittable diseases, especially in the COVID-19 era. If any family members show signs of infection, strict isolation of the sick family member from the patient is recommended.
Clinic visits should be avoided to minimize sick contacts. If the patient must come for a clinic visit, the facility should disinfect the room thoroughly before the visit. The number of staff members contacting the patient should be limited, and protective equipment should be worn.
Dietary consideration
Well water should be avoided as it might lead to waterborne infection. Untreated water can be contaminated and result in Cryptosporidium, norovirus, Giardia, Campylobacter, or rotavirus infections. 28 Boiled tap water and bottled water should be used.
Vaccination
Live attenuated vaccines, such as the mumps/measle/rubella, varicella, BCG (Bacilli Calmette-Guerin), oral polio, and rotavirus vaccines, can lead to life-threatening disseminated infections and are strictly contraindicated in patients with SCID. Inactivated vaccines do not cause infection but are most likely ineffective. 29
For household members, the live viral polio vaccine is prohibited due to possible viral shredding, leading to an active infection in the immunocompromised patient. 29 Some experts also advise against other live vaccines such as the varicella, measles, and Rotavirus vaccines in siblings for the same reason.15,30 Apart from those vaccines mentioned, all standard vaccines available, including the Coronavirus disease 2019 (COVID-19) vaccine and annual influenza vaccine, should be administered to maintain herd immunity in the family, including extended family members who may come into the home.
Breastfeeding
Breastfeeding should be suspended until maternal cytomegalovirus (CMV) status is known since CMV viral shedding is observed in 95% of CMV-positive mothers. Breastfeeding should also be avoided in the mother who has inactive CMV infection (CMV IgM-negative and CMV IgG-positive). This is because viral excretion through breast milk and viral reactivation can occur in infants with SCID. 31 In SCID infants, CMV can result in life-threatening disseminated infection and is also a major risk factor of mortality after hematopoietic cell transplant. 15 Although a recent retrospective study reported a similar incidence of CMV infection in SCID infants with CMV IgG-positive and negative mothers who breastfeed, further research is still needed to examine the risk-benefit of breastfeeding in this group of patients. 32 While waiting for the result, the mother may choose to continue pumping breast milk in order to maintain production. If the mother is positive for CMV IgG and/or IgM, breastfeeding should be avoided and ready-to-feed infant formula is recommended. 27 If the mother is CMV seronegative, breastfeeding can be resumed. 30 However, the risk of CMV transmission in case the mother acquires CMV infection after the serology screening is possible.
Blood products
If required, blood products should be irradiated, leukocyte-reduced with filters, and CMV-negative to prevent CMV transmission and GVHD from donors’ viable lymphocytes. 33
The patient’s flow cytometry showed:
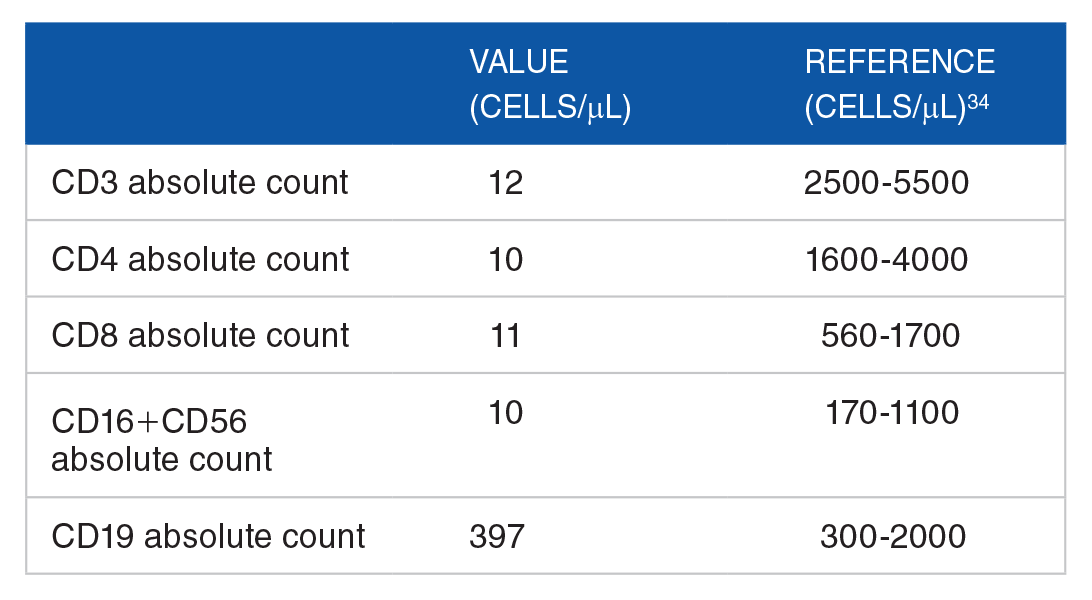
Severely low CD3, CD4, CD8, low CD16+CD56 and near normal CD19 counts indicated T- B+ NK- phenotype of SCID. Mitogen proliferation testing revealed severely low lymphocyte responses to PHA and concanavalin A, compared to control. Chromosomal Microarray was sent to rule out 22q11 deletion syndrome and it was found to be normal. The genetic panel revealed homozygous deletion of exons 18-23 of the JAK-3 gene on chromosome 19. After the diagnosis of JAK-3 SCID was confirmed, the patient was evaluated by the transplant team for HSCT. Pneumocystis jirovecii prophylaxis was initiated at one month of age. Replacement intravenous immunoglobulin was given every 4 weeks. She also received antimicrobial prophylaxis to Mycobacterium Avium Complex (MAC), herpes virus, and fungal pathogens.
Antimicrobial Prophylaxis
Once an infant is confirmed to have SCID, chemoprophylaxis against Pneumocystis jirovecii pneumonia (PJP) with oral trimethoprim-sulfamethoxazole or intravenous pentamidine is advised. Fungal prophylaxis with fluconazole, MAC prophylaxis with azithromycin, 33 and viral prophylaxis against the Herpesviridae family with acyclovir should be considered. Palivizumab is considered during the peak season of RSV, typically from November to March. 30 Immunoglobulin replacement therapy should be initiated as soon as possible. 35
Her clinical course was complicated with maternal T-cells engraftment, for which she was given tacrolimus for GVHD prophylaxis. The patient underwent an unrelated umbilical cord blood transplantation at the age of 3 months. After the transplant, she developed complications including veno-occlusive disease, CMV viremia, and multiple episodes of bacterial sepsis. Despite multiple complications, the procedure succeeded and she is engrafted at the age of 5 months. The patient has done well since then.
Hematopoietic Cell Transplantation
Allogenic hematopoietic cell transplantation by the bone marrow or umbilical cord blood is the mainstay treatment modality of SCID. Transplantation from HLA (human leukocyte antigen)-identical siblings is generally preferred as it provides better 5-year survival rate, independence from IVIG treatment, and better reconstitution of CD3 T-cells and IgA. Overall, the survival rate of hematopoietic cell transplantation is 74%. For patients without prior infection and undergo transplantation before 3.5 months of age, the survival rate may be as high as 94%. The major goal of treatment is to correct T-cell deficiency and T-cell dysfunction. Recovery of B-cell function occurs in some patients and is found to be less consistent depending on the mutations and pretransplant conditioning regimens. 3 The more common long-term complications following hematopoietic cell transplantation include persistent GVHD, autoinflammatory events, chronic HPV infection, growth insufficiency and the need for nutritional support. 36
Chronic GVHD can last for years and affect 15% of SCID patients after transplant. 3 Distinctive clinical manifestations include skin lesions mimicking lichen planus or scleroderma, strictures or stenosis of the gastrointestinal tract, joint contractures, and bronchiolitis obliterans. Mild symptoms can be treated with localized therapies. Severe chronic GVHD with multiple organ involvement requires systemic immunosuppressants, initially with glucocorticoid. 37
Other treatment modalities for SCID patients include gene therapy and enzyme replacement therapy. Gene therapy is performed by inserting a normal copy of the gene into vectors, transducing them into hematopoietic stem cells, and transfusing them into patients to restore the function of the abnormal gene. The treatment has been shown to be effective in ADA-SCID and X-linked SCID and is expected to be more widely available in the near future. 38 Enzyme replacement therapy is used to restore immune function in patients with ADA-SCID as a bridging therapy before transplantation. 18
A term male newborn was born via spontaneous vaginal delivery at the gestational age of 38 weeks. He was diagnosed with truncus arteriosus, perimembranous VSD, and interrupted aortic arch type B by antenatal ultrasound. At birth, he appeared vigorous but cyanotic. Oxygen saturation was 67% to 88%. He was transferred to the intensive care unit for prostaglandin transfusion. CBC reported lymphopenia of 1700/mm3. His initial serum calcium was 8.7 mg/dL. Chest X-ray revealed absent thymus gland. The TREC newborn screening for SCID was performed at 28 hours and reported a strong positive with 40 TREC Ct (cycle threshold)/3 mm punched disk (normal value <35.7, borderline positive 35.7-36.2, and strong positive ⩾36.3 TREC Ct/3 mm punched disk) at 120 hours of age. Since there was a possibility for SCID, isolation protocols were implemented. The positive TREC screening also raised concerns for congenital athymia, and DiGeorge syndrome was suspected due to the conotruncal cardiac defect and borderline hypocalcemia. Flow cytometry and immunoglobulin levels were sent to evaluate his immune function. The patient’s flow cytometry showed:
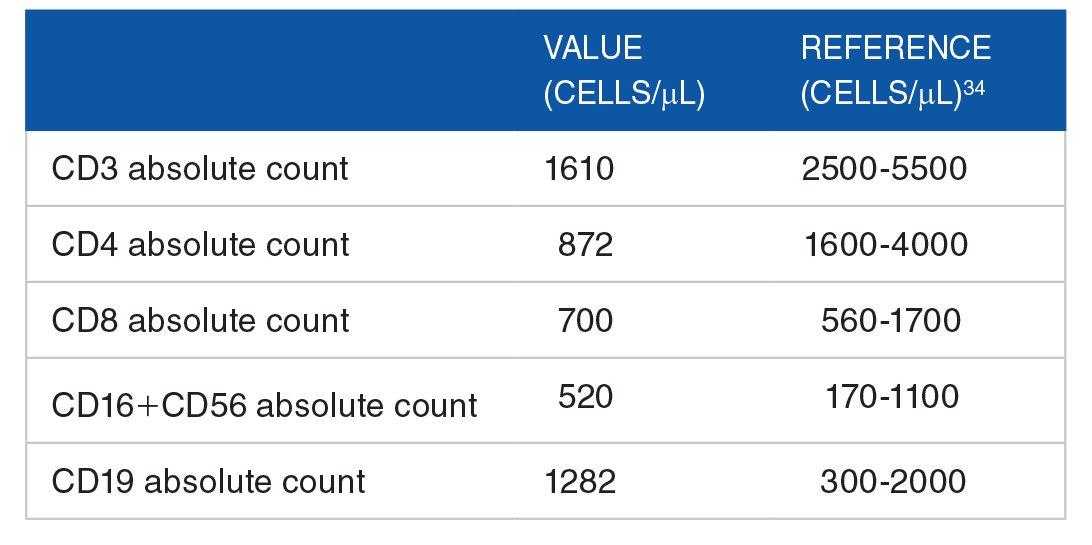
Flow cytometry confirmed T-cell lymphopenia with low CD3, CD4, and CD8 T-cells; however, they were not absent. B-cell and NK-cell subsets were normal. IgG and IgM were normal. Mitogen proliferation reported low lymphocyte responses to PHA and concanavalin A indicating decreased T-cell function. The reduced but not absent T-cells number and function are compatible with partial Di George syndrome rather than SCID. Chromosomal microarray revealed microdeletion at 22q11.21, confirming the diagnosis of DiGeorge syndrome. The patient underwent corrective cardiac surgery, received PJP prophylaxis, calcium and vitamin D supplement, and was discharged at the age of 2 months.
Non-SCID Etiologies of T-Cell Lymphopenia
TREC newborn screening for SCID has a sensitivity as high as 100% but a positive predictive value is only at 0.8% to 18%, depending on the cut-off value.39,40 Low TREC copies indicate T-cell lymphopenia, and can be seen in any condition with decreased T-cell production, not only SCID. 6 In fact, most infants with positive TREC newborn screening did not have SCID but had T- cell lymphopenia that was related to other causes.1,41 Therefore, it is important to consider other conditions that can cause T-cell lymphopenia when the TREC newborn screening is positive.
Genetic syndromes that cause T-cell lymphopenia
Congenital athymia (CA) is a rare condition characterized by the absence of the thymus gland at birth. Its estimated incidence in the USA is between 17 and 24 live births each year. 42 Several genes play roles in thymic development, for example, FOXN1, PAX1, TBX1, and CHD7. The defects of these genes can result in CA and syndromes associated with midline defects, including 22q11.2 deletion syndrome and coloboma, heart defect, atresia choanae, retarded growth and development, genital and ear abnormality (CHARGE) syndrome. Maternal diabetes and exposure to retinoic acid are also associated with abnormal development of the thymus gland. Patients with CA typically presented with similar clinical presentation as SCID with T-negative, B-positive, NK-positive phenotypes. However, distinguishing CA from SCID with genetic testing is crucial because CA could be treated with cultured thymus tissue implantation (CTTI) while generally the treatment for SCID is HSCT. CTTI has been shown effective to restore T-cell function via the migration of stem cells from bone marrow to the implanted thymus tissue, resulting in naive T-cells development.43,44
22q11.2 deletion syndrome (22q11.2del) is the most common microdeletion syndrome in humans, leading to a spectrum of clinical features including cardiac defects, hypocalcemia, thymic aplasia, and facial dysmorphisms such as hypertelorism, bulbous nose tip, and micrognathia. 45 DiGeorge syndrome (DGS) is a syndrome caused by 22q11.2 deletion with the core triad of (i) thymic aplasia and/or cellular immune defects, (ii) hypocalcemia and/or parathyroid defect, and (iii) conotruncal cardiac anomalies. 45 T-cell lymphopenia is commonly found in 75% to 80% of infants with DGS, ranging from severe T-cell deficiency with thymic aplasia in complete DGS to mild T-cell lymphopenia in the partial form. 46
According to the data from 11 states, DGS was the most common syndromic cause of non-SCID T-cell lymphopenia identified through TREC newborn screening, accounting for 57% of genetic syndromes that trigger a positive TREC screen. 1
Down syndrome (DS) is the most common chromosomal disorder found in humans, with a prevalence of approximately 1 in 700 live births. 47 It is caused by extra genetic material from chromosome 21, resulting in various multisystem anomalies including hematological alteration. Compared with the normal population, infants with DS frequently have significantly lower TREC levels, and low absolute T-cells count is frequently found. 48
Other causes of genetic non-SCID causes of T-cell lymphopenia are shown in Table 2.1,49

Abbreviations: CHARGE, coloboma, heart defect, atresia choanae, retarded growth and development, genital and ear abnormality; CLOVES, congenital lipomatous overgrowth, vascular malformations, epidermal nevi, and spinal/skeletal anomalies; EEC, ectodermal dysplasia, ectrodactyly, and clefting; EXTL3, exostosin-like glycosyltransferase 3; SCID, severe combined immunodeficiency; TAR, thrombocytopenia and absent radius.
A preterm female newborn was born via cesarean section at the gestational age of 24 weeks after her mother had been diagnosed with chorioamnionitis. The infant had a weight of 600 grams and the Apgar scores were 3, 3, 6 at 1, 5, and 10 minutes after birth. She was intubated, required high-frequency ventilation, and was given surfactant therapy. Her clinical course was later complicated by a large patent ductus arteriosus (PDA), persistent pulmonary hypertension of the newborn (PPHN), and neonatal sepsis. A dried blood spot was sent for newborn screening at the age of 24 hours and reported a borderline positive of 35.8 TREC Ct/3 mm punched disk (normal value <35.7, borderline positive 35.7-36.2, and strong positive ⩾36.3 TREC Ct/3 mm punched disk) at 120 hours of age.
Non-SCID Etiologies of T-Cell Lymphopenia (Cont.)
Secondary T-cell lymphopenia
Any conditions in which lymphocytes are lost from circulation can cause T-cell lymphopenia, including congenital heart disease (CHD), chylothorax, hydrops, intestinal atresia, and gastroschisis. 26 There is also a case of lymphopenia caused by thymic teratoma which resolved after resection of the tumor. 49 Infants with CHD can have significantly lower TREC levels when compared with normal newborns, regardless of the CHD defect and even without hydrops and before cardiac surgery. 50 The TREC value of infants with 22q11.2 deletion and conotruncal heart defects is significantly lower compared to those with non-syndromic conotruncal and non-conotruncal defects. This effect could be attributed to the common embryology of the heart and the thymus, endogenous glucocorticoid production induced by hypoxia, and suppression of lymphopoiesis due to stress. 51
Maternal medications are also reported to cause low absolute T-cell numbers in infants, including azathioprine and fingolimod. Decreased lymphocyte count has been reported in infants whose mothers received antenatal corticosteroids. 52 Perinatal stress and infection can also cause thymic involution and low TREC levels. 53
Preterm birth
T-cell lymphopenia can be associated with preterm birth, typically in infants born at or before the gestational age of 32 weeks. The condition simultaneously resolves in most infants that are retested. 49 Studies show a linear association between prematurity and TRECs, where TREC value increases 9.6% with every increasing week of gestational age.53,54
Idiopathic T-cell lymphopenia
Cases of T-cell lymphopenia and immune dysfunction without identifiable underlying immunologic and genetic causes are termed idiopathic T-cell lymphopenia. It is a diagnosis of exclusion. This condition accounts for approximately 3% of non-SCID causes detected by newborn screening. 1
Other non-SCID causes of T-cell lymphopenia are shown in Table 3.1,49
Other Non-SCID conditions identified by TREC screening.

The infant was born extremely preterm with multiple perinatal and postnatal stressors, including maternal chorioamnionitis, neonatal sepsis, respiratory distress, PPHN, and PDA. All of these factors can cause T-cell lymphopenia, thus, the screening results in preterm newborns with complications should be interpreted with caution. At the age of 30 days old, her condition improved. The respiratory support was adjusted to synchronized intermittent mandatory ventilation. Medical closure of the PDA was successful, and the infection subsided. The newborn screening was repeated at 30 days and reported as normal.
Although protocols vary in each state, repeating TREC levels is often considered in patients who are born prematurely or have suspected secondary lymphopenia from other causes such as cardiac defects, hydrops, or severe medical conditions that require neonatal intensive care unit admission. A repeat screening is helpful to determine if TREC levels normalize once an infant’s medical condition improves or resolves.
Limitation
Limitations of our review include possible reporting and publication bias, which might affect the findings reported in the article.
Conclusion
TREC newborn screening was implemented to identify patients with SCID before the onset of symptoms. Primary care physicians play a vital role in the initial evaluation and management of patients with SCID. Prior to making the definitive diagnosis, parents should be advised on how to prevent infections as infections reduce the survival outcome of patients with SCID significantly. Additional investigations, mainly flow cytometry and genetic testing, should be obtained to establish a definite diagnosis. These laboratory tests are typically arranged by a coordinating pediatric center with immunologists. Once the diagnosis is confirmed, patients should be placed on the appropriate prophylaxis to prevent infection and referred to a transplant center, where patients with SCID can undergo stem cell transplantation.
Since TREC newborn screening can also be positive with several other conditions that cause T-cell lymphopenia, it is important for primary care physicians to be familiar with non-SCID etiologies that may trigger a positive newborn screen. Other possible causes of low TREC levels should be considered and evaluated with the aid of the coordinating center and immunologists.
Although SCID is a severe condition with high morbidity and mortality, early diagnosis by newborn screening and timely multidisciplinary management can result in excellent clinical outcomes.
Supplemental Material
sj-docx-1-pdi-10.1177_11795565231162839 – Supplemental material for Positive Newborn Screening for Severe Combined Immunodeficiency: What Should the Pediatrician Do?
Supplemental material, sj-docx-1-pdi-10.1177_11795565231162839 for Positive Newborn Screening for Severe Combined Immunodeficiency: What Should the Pediatrician Do? by Wimwipa Mongkonsritragoon, Jenny Huang, Mary Fredrickson, Divya Seth and Pavadee Poowuttikul in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-docx-2-pdi-10.1177_11795565231162839 – Supplemental material for Positive Newborn Screening for Severe Combined Immunodeficiency: What Should the Pediatrician Do?
Supplemental material, sj-docx-2-pdi-10.1177_11795565231162839 for Positive Newborn Screening for Severe Combined Immunodeficiency: What Should the Pediatrician Do? by Wimwipa Mongkonsritragoon, Jenny Huang, Mary Fredrickson, Divya Seth and Pavadee Poowuttikul in Clinical Medicine Insights: Pediatrics
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.