
Abstract
Jenunoileal atresia is a congenital defect that causes small bowel obstruction in newborns. They are classified into 5 types and simple abdominal x-ray can aid in the diagnosis and with prompt resuscitation and surgery provides positive outcome. We present a 5-day-old newborn male baby was presented with features of intestinal obstruction since birth. Diagnosis of atresia of the small bowel was made through plain abdominal x-ray and was successfully operated. During the recovery, the baby developed surgical site infection which was managed promptly.
Background
Case Presentation
A 5-day-old male baby was referred to our center with the chief complaint of vomiting since birth. The vomitus was described to be greenish with the smell of fecal matter by the mother, which was mostly after being breastfed. It was reported that he did not pass meconium until the third day of life where he passed a small amount of dark mucoid stool. He had no fever, and was passing urine normally. The baby was delivered vaginally at term with the birth weight of 3900 grams. He cried immediately after birth and was breastfed within the first hour after delivery. The mother started antental clinic at 12 weeks of gestation and made 5 visits and received supplements according to the national guidelines. She was tested negative for HIV and syphilis. Mother was normotensive with normal blood sugar levels.
On examination the baby had grade-5 jaundice, dehydrated with clubbed feet and his vitals were stable. Body weight on admission was 3100 grams. Abdominal examination showed symmetrically distended abdomen, hyper tympanic percussion note with exaggerated bowel sounds. The rectum had little soft fecal matter. Duodenal atresia was suspected and Abdominal USS and erect abdominal X-ray were done. Abdominal X-ray showed dilated bowels with multiple air-fluid levels (Figure 1), abdominal USS showed normal findings. Lab work up showed Hb of 14.8 g/dL, potassium of 3.8 mmol/L and sodium of 135 mmol/L. He was kept nil orally, given IV fluids and scheduled for an emergency laparotomy.
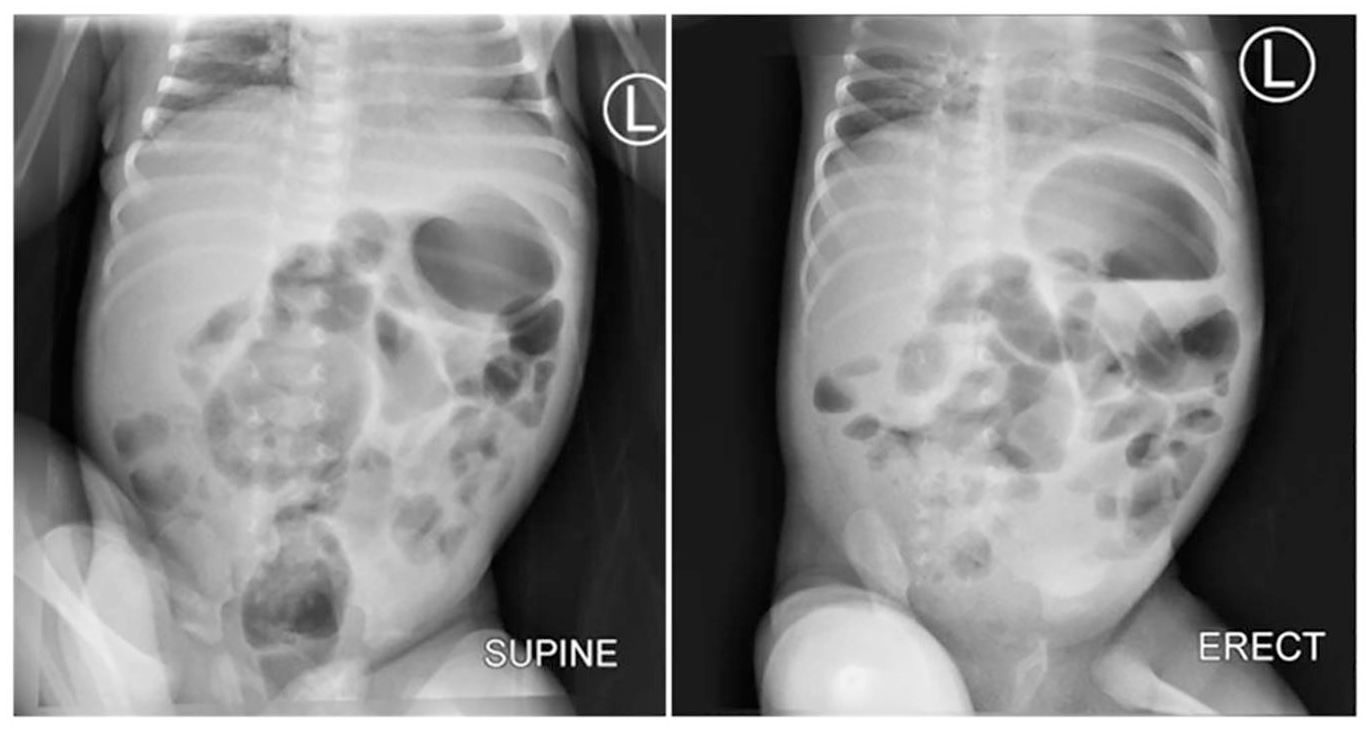
Supine and erect abdomen x-rays done 12 days later shows multiple dilated jejunal and ileal loops with multiple air fluid levels suggestive of ileal obstruction. No evidence of pneumoperitoneum.
Intra-operatively, a complete atretic ileum approximately 45 centimeters proximal from the ileocecal junction was found (Figure 2). The proximal ileum was dilated while the distal ileum was collapsed. An ileal-ileal side-to-side anastomosis was done and the small bowel continuity was established (Figure 3). The post-operative diagnosis was Type-3A mid-ileal atresia. The baby was kept nil per oral, given IV fluids; Dextrose Normal Saline, IV Antibiotics and analgesia.

Type IIIA ileal atresia.

Side-to-side anastomosis (arrow).
Post operatively, the baby continued to do well clinically, started to tolerate oral feeds and passing stools normally. The jaundice gradually subsided. On day 4, the child started having serous discharge per abdominal incision with hyperemic skin hence diagnosis of surgical site infection was made. The baby was dressed twice a day and kept on intravenous Meropenem as pus culture and sensitivity isolated Escherichia coli. During the stay bedside dressing and debridement improved the wound.
On the 20th day post operative, the baby was discharged with oral codliver oil by the pediatric team and mother was counseled to continue dressing at a nearby health center. He was reviewed 2 weeks later at the surgical outpatient unit where the wound had healed fully and was tolerating feeds well.
Discussion
Intestinal atresia can occur in any location on the small bowel as a solitary as in the index case, or even multiple lesions. Distally located atresia usually presents with delayed symptoms compared to proximal ones. Occasionally, JIA is associated with other malformations such as cardiac anomalies, gastroschisis, and cystic fibrosis. 1
Clinical presentation includes; abdominal distension, bilious or non-bilious vomiting, and delayed or no passage of meconium. Physical examination should include a general assessment of the severity of illness, abdominal distension, evidence of peritonitis, respiratory compromise from aspiration or splitting of the diaphragm, signs of dehydration, jaundice and congenital anomalies such as Down’s syndrome, congenital heart disease and anorectal malformation of which was excluded clinically from our case. 1
Approximatelty 95% of intestinal obstructions are diagnosed within the first 2 weeks of life but for ileal atresias the diagnosis can be made as early as 24 hours of life, but can extend to 30 days and for our case the diagnosis was made within the first 3 days of life after being referred to our facility. 4
Advances in radiological workups have aided to reaching diagnoses through ultrasound scans, x-rays and contrast studies. On plain abdominal X-rays one may see; numerous loops of dilated bowels, multiple air-fluid levels proximal to the obstruction. 5 In our case plain abdominal x-ray showed multiple air-fluid levels just as in the study by Jumbi et al which was done in Nairobi. Ultrasound sonography (USS) is shown to be useful when there is utero obstruction, where dilated bowels are filled with fluid. In postnatal period; air is introduced in the gut making USS less useful as in the index case. 6
Management of ileal atresia includes insertion of nasal gastric tube for drainage and decompression, intravenous fluid resuscitation, use of total parenteral nutrition (TPN) and operative management. 7 Surgery can be an open or laparoscopic assisted surgery (LAS). The LAS in the treatment of neonatal JIA is safe and feasible and with shorter operative and restoration of enteral feeding times. The post-operative outcomes in LAS are similar with OS where primary end to end anastomosis is done as in the index case. Treatment of this malformation is plication or tapering enteroplasty with end-to-side anastomosis as was done in this case. Initial enterostomy with delayed closure has been done in few cases with good results, but it showed no added advantage over primary anastomosis, with a lower rate of postoperative complications.8-10
There is better postoperative outcomes in patients that used TPN where they have faster recovery and shorter hospital stay but for this case the patient was put on maintenance dextrose normal saline and lactated ringers solution. 1 TPN could not be used because of financial constraints hence experienced prolonged recovery time. Surgical site infection (SSI) also attributed to prolonged stay in the hospital despite covering the patient with broad spectrum antibiotics. The lancet infectious disease journal showed Countries with a low Human Development Index (HDI) carry a disproportionately greater burden of SSI than countries with a middle or high HDI and might have higher rates of antibiotic resistance. 11
Conclusion
Jejunoileal atresia is a rare congenital anomaly that causes small bowel obstruction in newborns, particularly premature. Basic radiologic modality like plain abdominal x-ray can aid the diagnosis. Resection of the blind end with end-to-end anastomosis is the procedure for treatment after adequate resuscitation.
Footnotes
Acknowledgements
The authors would like to thank the child’s mother for permission to share her child’s medical history for educational purposes and publication.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GG and JL conceptualized and drafted the manuscript. MG was the lead surgeon. DM and SC reviewed the medical records. AS prepared and reported the radiology films. All authors have read and approved the final manuscript.
Consent
Written informed consent was obtained from the child’s mother for publication for this case report; additionally, accompanying images have been censored to ensure that the patient cannot be identified. A copy of the consent is available on record.
Ethical Approval
Approval was obtained from the department of General Surgery and the appropriate hospital institutional review board has approved the publication of this case report.