
Abstract
Objective:
Masses of the sternoclavicular area are rare, and are not well described in the literature. We aim to present a series of patients with masses in this location and to review all reported English language cases of sternoclavicular masses in pediatric patients.
Methods:
This is a case series of pediatric patients with masses of the sternoclavicular area presenting to a tertiary care pediatric hospital from 2010 through 2017. Data was collected by using ICD-9 and ICD-10 codes to query the electronic medical record. Chart review included age at presentation, mass characteristics, medical and surgical interventions, and pathology results. A review of the literature was then performed.
Results:
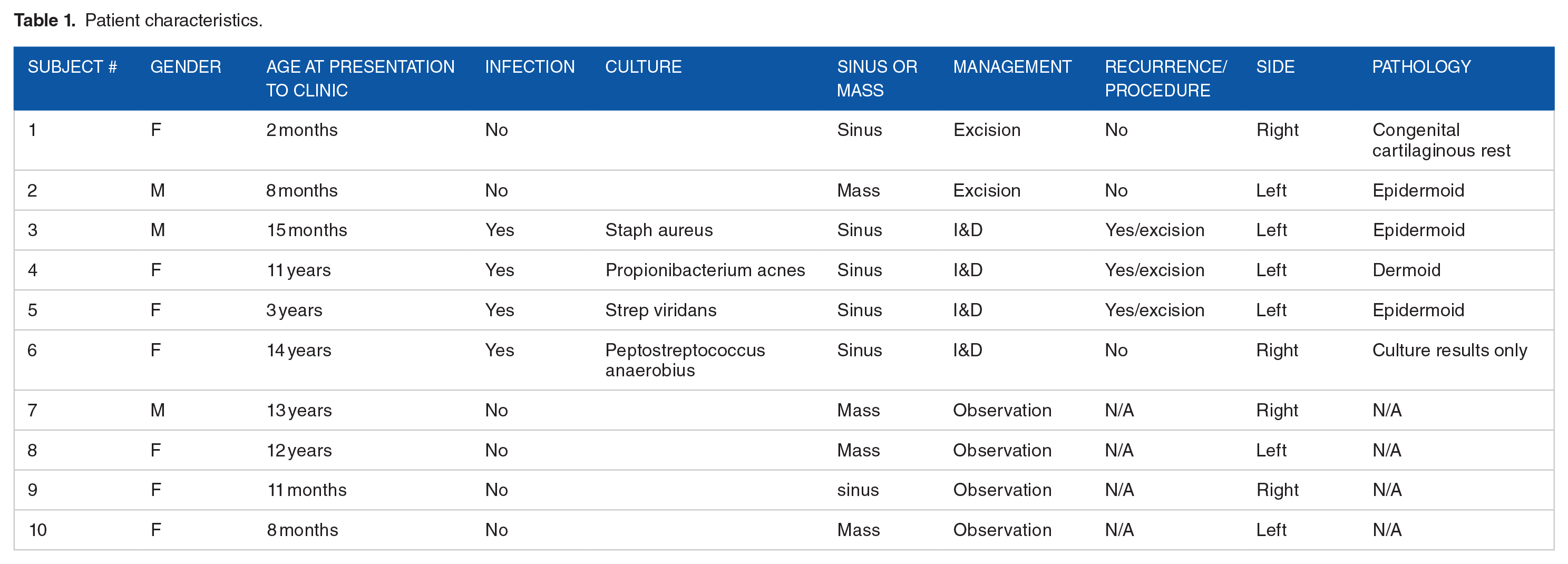
Ten patients with masses overlying the sternoclavicular area were identified. Four patients presented with abscess and were treated with incision and drainage. Three of these patients were then treated with staged excision once infection cleared. Two additional patients were treated with primary excision. Four patients were treated with observation. The most common histopathologic finding was epidermoid. One patient was found to have a dermoid cyst, and 1 had a congenital cartilaginous rest.
Conclusion:
Epidermoids and dermoids are the most common masses overlying the sternoclavicular area. Controversy remains regarding the embryologic origin of sternoclavicular masses. The differential for masses in this area also includes branchial remnants, bronchogenic cysts, ganglion cysts, or septic arthritis.
Introduction
Quickly narrowing the differential of a pediatric neck mass is crucial for patient counseling and surgical planning. While the location of a mass in the neck is one of the most helpful characteristic features to narrow the differential, there is very little published literature to guide surgeons who encounter a mass of the sternoclavicular area. Neck masses of the sternoclavicular area require prompt recognition by practitioners when associated with a sinus in order to prevent risk of infection or abscess.
The most commonly encountered pediatric neck masses are dermoid and epidermoid cysts, which result when the branchial arches entrap epithelial structures during closure.1,2 Branchial cleft cysts are also common and typically located laterally in the neck, anterior to the sternocleidomastoid muscle. Much more rarely seen are bronchogenic cysts, congenital thymic cysts, or hamartomas.2,3 Most studies that assess masses of the sternoclavicular area are singular case studies or assess only 1 type of pathology.
Supraclavicular lymphadenopathy is an important clinical sign which could be a warning sign for an abdominal malignancy. While supraclavicular lymphadenopathy has been well described, masses located directly over the sternoclavicular joint have not been well characterized. These are typically small and superficial, and are often associated with a sinus tract or a deeper fibrous band. This study aims to characterize masses overlying the sternoclavicular joint at a pediatric hospital and to compare these results to the published English language literature, with the goal of helping pediatric physicians to improve surgical decision making and to improve pre-operative counseling for patients with these masses.
Methods
Institutional Review Board approval was obtained to retrospectively access patient charts from January 2010 through 2017 for this study. ICD-9 code 733.21 and ICD-10 codes M85.612 and L02.213 were used to query the electronic medical record for patients seen in a physician’s clinic with masses of the sternoclavicular area. A chart review was done and included pediatric patients aged 18 or under that presented to the clinic during this time period. Patients were excluded if they were lost to follow up, if the mass was not directly overlying the sternoclavicular joint, or if a treatment plan was not specified. Patient gender, ethnicity, age at presentation, size of mass, pathology findings, medical, and surgical interventions were recorded. A review of the literature was then performed in order to comprehensively evaluate all published series of pediatric patients with masses of the sternoclavicular area.
Results
Patient demographics
Twelve patient records were retrieved and 10 met inclusion criteria. Average patient age at time of presentation in otolaryngology clinic was 5.67 years. Seven patients were female and 3 were male. Of the ten patients, 3 patients were white, 3 were Asian, 3 identified as other, and one’s race was not listed. Three patients additionally identified as Hispanic.
Mass characteristics
Mass characteristics were recorded in ten patients. Five patients had evidence of a mass over the sternoclavicular area which was noted at birth. Four patients had masses that were first identified between 8 and 12 months of age, and were described as a “pit” or “pimple” appearance. One patient had a mass over the sternoclavicular area that was first identified at 13 years of age. Masses ranged from 0.1 to 4 cm (average diameter = 1.34 cm). Six patients presented with masses on the left and 4 with masses on the right. Five (50%) patients had cysts that were infected at initial presentation. Age at time of infection ranged from 6 months to 14 years.
Management and pathology results
Four patients were treated with observation only due to asymptomatic mass and parent preference. Average age at presentation for patient who were treated with observation only was 6.6 years. None of these patients had a history of infection. Two of these patients were evaluated with ultrasound only. One was evaluated with ultrasound and MRI.
Of the patients who presented with infection, 3 had a persistent sinus once the incision and drainage site healed, and these patients underwent staged complete excision. The fourth patient who underwent incision and drainage experienced complete resolution following the initial drainage procedure.
Five patients eventually underwent complete surgical excision. Pathologic analysis was done by board certified pathologists at our institution. Of these 5 patients, 3 (60%) of these masses were epidermoid cysts, 1 (20%) was a dermoid cyst, 1 (20%) was a congenital cartilaginous rest. The 5 patients that presented with infection of the mass all had growth on bacterial culture. One grew Peptostreptococcus species, 1 grew Streptococcus viridans, 1 grew Staphylococcus aureus, and 1 grew Propionibacterium acnes. Table 1 summarizes patient characteristics and interventions.
Patient characteristics.
Complications
Of the 4 patients treated with incision and drainage, 1 post-op course was complicated by keloid formation and 1 was complicated by hypertrophic scar. Only 1 of these patients elected to undergo scar revision.
Discussion
This case series of ten pediatric patients with cysts presenting in the sternoclavicular region is the largest series yet reported. Among our patients the most common pathology encountered was epidermal inclusion cysts, followed by equal proportions of dermoid cyst, and congenital cartilaginous rest. We did not identify any significant gender or ethnic differences among patients with masses overlying the sternoclavicular area. Infection of the mass during initial presentation tended to prolong the treatment course, with 75% of patients requiring a second definitive excision following initial incision and drainage. In contrast, none of the patients who underwent complete excision prior to any infection required any additional surgery.
While masses over the sternoclavicular area are not well described, the small number of reported English language series is reviewed here. These series are also summarized in Table 2. The most commonly encountered lesions in this area in the published literature are dermoid sinuses and branchial remnants. More rare entities on the differential include hamartomas, bronchogenic cysts, sternoclavicular ganglion cysts and infectious arthritis. Lesions can be usually be differentiated from sternoclavicular lymphadenopathy based on history, exam and imaging with ultrasound. Likely because of the rare reports of this type of pathology, it seems that there is a relatively large variety of terms used to describe dermoids and branchial remnants in this area.
Review of literature.

Kargl and others describe 5 patients who were treated for a congenital lesion which they coined “sinus sternoclavicularis.” They differentiated these lesions from dermoid or epidermoids due to the presence of the excretory duct associated with the sinus sternoclavicularis. Eighty percent of the patients in the series underwent surgery, and 40% of surgical patients required a second surgery due to initial infection or subsequent complication. Authors argue that history is sufficient for diagnosis without any imaging, and they propose initial surgery with incision and drainage for patients who present with abscess followed by staged definitive excision. 2
Hosokawa and others describe 2 patients with congenital dermoid fistulas of the anterior chest region (CDFACR), and describe skin orifice at the anterior sternocleidomastoid with fistula and/or fibrous tissue that extends to the sternoclavicular joint. The authors discuss 2 separate hypotheses of their origin: disorderly fusion of sternum to clavicle versus remnant of fourth branchial cleft. While no conclusion is made about the embryologic origin of the masses, the authors do conclude that sonography and physical exam are sufficient to differentiate CDFACR from other congenital neck masses. 4 A single case report from Kyoto described this entity in a 1 year old which presented as an abscess associated with a cutaneous pit, and was completely excised. 5 We do not favor the terminology of fistulas, since the lesions only open at 1 end and are instead consistent with a sinus.
Willaert and others describe sternoclavicular dermoid sinuses in 8 children who all had lesions on the left side. They propose this terminology due to the location of lesions and the presence of adnexal structures of endodermal origin adjacent to squamous epithelium, which differentiates them from epidermoids. Although 87% of their patients presented with infection or abscess, the authors treated all patients with complete excision without any recurrence. They advocate for early excision of these sinuses due to risk of developing infection if left alone. 6
Ohno and others describe 7 patients with sinuses near the sternoclavicular joint at the anterior border of the sternocleidomastoid muscle and on the line of the clavicular bone. While most of the surgical specimens consisted of stratified squamous epithelia, 1 tract was composed entirely of columnar epithelium, and 1 contained both squamous epithelium and columnar epithelium. Authors proposed that this pathology of lesions in this location is different than a dermoid fistula and the etiology is due to a remnant of a fourth branchial fistula. 7
Another pathologic finding that is thought to be a remnant of the branchial apparatus is the cervical chondrocutaneous branchial remnant. The other theory is that these masses are due to an ectopic rest of auricular tissue. Other names for this pathologic finding are “wattles”, “accessory tragus”, or “congenital cartilaginous rest of the neck.” 8
In our series, only one of the masses over the sternoclavicular joint was found to be a congenital cartilaginous rest of the neck. In addition to these ectopic rests of normal tissue, an ectopic rest of disorganized tissue can also form over the sternoclavicular area, although this seems to be more rare. Rhabdomyomatous mesenchymal hamartoma is a rare entity that has been described in the sternoclavicular area. These can be well circumscribed or more infiltrative and may recur. 3
The differential diagnosis for a mass over the sternoclavicular area also includes a ganglion cyst. While no patients in this series were found to have a ganglion cyst, Haber and others describe a series of 5 children with this diagnosis. In these cases, none of the masses were present at birth, and there appears to be no predilection to the right or left side. Authors recommend ultrasonography for evaluation and excision only when lesions are symptomatic. 9
Septic arthritis of the sternoclavicular joint is also on the differential for a mass overlying the sternoclavicular area. This joint is affected in only 1% of septic arthritis cases and is characterized by pain with motion of the arm and shoulder on the affected side, pain and erythema of the skin overlying the joint, and elevated white blood cell count and C-reactive protein. 10
A pit or sinus tract in the lateral neck always brings to mind a branchial sinus as a leading diagnosis on the differential. 11 In this particular location no true brachial sinus has been reported in the English literature. The most common pathology seen of the sternoclavicular area at our hospital is the epidermal inclusion cyst. Pediatric practitioners should thus strongly consider epidermal inclusion cysts in their differential diagnosis for pediatric neck masses in this region.
The chief limitation of this study is its small sample size of only ten patients. Future complications may also not be captured in the immediate follow up period. Larger and long-term studies should be conducted to assess long-term outcomes and complications after cyst excision and possible recurrence of masses overlying the sternoclavicular area. Follow up investigations would benefit from prospective data collection as there were likely other patients with masses overlying the sternoclavicular area that were not captured with these ICD-9 and ICD-10 codes.
Conclusions
Neck masses overlying the sternoclavicular joint are an uncommon but important diagnosis among pediatric patients. This case series and review of the literature suggests that epidermoids and dermoids are the most common lesion overlying the sternoclavicular joint. The pediatrician’s differential diagnosis should also include more rare pathology such as bronchogenic cyst and ganglion cyst. Based on our experience, patients presenting during acute infection should be counseled that a second definitive surgery is often required of these masses following initial incision and drainage. If a patient presents prior to any infection, definitive excision is the treatment of choice as it has a low rate of complication.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Note
This manuscript was presented as a poster presentation American Academy of Otolaryngology - Head and Neck Surgery Foundation 2018 Annual Meeting & OTO Experience, October 7-10, 2018 in Atlanta, GA.