
Abstract
Objective:
To examine our institutional experiences with ultrasound-guided peripherally inserted central catheter (US-PICC) placement by a dedicated US-PICC team under the umbrella of an existing pediatric sedation service.
Methods:
Retrospective review of quality data examining 968 US-PICC encounters over a 5-year period from 2012 to 2016. Data for each encounter included line indications, success rate, dwelling time, need for sedation, and incidence of complications including venous thrombosis, infection, and accidental removal.
Results:
US-PICC lines were successfully placed in 89% of patients with an average age of 5.4 years. Extended antibiotic treatment was the most common indication for US-PICC placement and the mean dwell time was 23 days. Long-term complications were noted in 6.1% of cases, with venous thrombosis and line infection complicating 1.7% and 0.9% of encounters, respectively.
Conclusion:
Results suggest that our endeavor of creating a dedicated US-PICC team under an existing pediatric sedation service is successful with regard to the number of lines placed, success rates, and incidence of complications. This approach may be beneficial to other institutions seeing to maximize resource utilization and streamline patient care.
Introduction
Peripherally inserted central catheter (PICC) placement is a commonly performed procedure in pediatrics which requires special training. 1 These catheters are inserted via peripheral veins then advanced ultimately to reside in the major veins, the superior vena cava or inferior vena cava. Imaging is often used to aid placement, most commonly ultrasound. Indications for PICC placement vary but include the need for reliable intravenous access, long-term antibiotic therapy, and total parenteral nutrition (TPN).1,2 Historically at our institution, US-PICCs were placed by several different providers including intensive care unit (ICU) physicians, nurse practitioners, and interventional radiologists. This approach was inefficient and was associated with family and provider dissatisfaction secondary to practice variation and provider availability for concurrent procedural sedation. Data over the last several years have shown an upward trend in the number of dedicated, nurse-led PICC teams in both adult and children’s hospitals. 3 These dedicated nurse PICC teams receive additional training in anatomy, physiology, and ultrasound techniques and have been associated with improved safety and cost-effectiveness.3-6 However, in the pediatric population, PICC placement is commonly complicated by the need for concurrent procedural sedation to facilitate line insertion, alleviate pain, and optimize arm positioning. 7 This can complicate the process by necessitating additional coordination with a separate anesthesia or sedation service. After an assessment of patient needs and available resources, a dedicated pediatric US-PICC team was developed under the umbrella of an already existing pediatric sedation service at our institution in 2012. There is a relative paucity of literature addressing this particular service model, especially with regard to quality, safety, and resource utilization. This study describes our experiences with a single team providing both US-PICC procedures and sedation over a 5-year period.
Methods
Our hospital is a 136-bed tertiary academic children’s hospital within a hospital and part of a large healthcare system in the Midwest. Our team was created to place PICC lines under ultrasound guidance, typically in the upper extremity (the basilic, cephalic, or brachial veins) and less commonly in the lower extremity (saphenous vein). Training for our team members consisted of education by the PICC vendor (https://www.bardaccess.com/products/nursing), 8 working with the adult US-PICC team, and then a period of proctored line placements supervised by experienced providers. Placement is via the modified Seldinger technique aided by ultrasound guidance for locating and accessing the vein. We also utilize a magnetic tracking system and continuous electrocardiography to ensure adequate placement in the deep veins (https://www.bardaccess.com/products/imaging/sherlock-3cg), 9 though final placement is confirmed by chest radiography. Catheter size is 3 to 5 French and may be single, double, or less commonly triple lumen. Catheters are secured using a sutureless device, and covered with an antimicrobial disk and sterile dressing. This method is utilized for infants and children at our institution. For neonates and younger infants, such as in the neonatal intensive care unit (NICU), our team may place US-PICCs if the patient weighs greater than 3 kg and the veins visible under ultrasound can accommodate a 3-French catheter, the smallest placed by our team. If the patient does not meet these criteria, advanced practice providers in the neonatal ICU will typically place different types of central lines, as appropriate (eg, umbilical catheters, other types of lines placed under direct visualization).
When the US-PICC team was created, patient and quality data were recorded for each line attempted. The US-PICC nurses recorded the information on a data collection form, and the information was then put into a spreadsheet by office staff. The purpose of this process was to track the number of cases and our complication rate for internal quality metrics. Because we relied on the procedure nurses to record data, and completion of the sheet was not monitored or enforced, some data points were not recorded for every US-PICC. The summary presented in this report contains data on our US-PICC service from March 2012 to May 2017.
Demographic information obtained included the patient’s age in years and, if below 1 year old, age in weeks. Indications for US-PICC placement were tracked and separated into various common categories including need for long-term antibiotics, TPN, difficult intravenous (IV) access, ongoing blood draws, other long-term IV infusions, and chemotherapy. Placement in the general ward, operating room (OR), pediatric ICU, or neonatal ICU was documented in addition to the need for sedation to complete the procedure. We defined sedation as moderate or deep sedation as outlined in the 2002 practice guidelines from American Society of Anesthesiologists. 10 Patients requiring only anxiolysis were considered as having not been sedated.
To determine the team’s efficiency, several US-PICC metrics were followed over the study term. We tracked number of procedures completed within 24 hours of the request and the reason for delay if the line was not placed in that time frame. The procedure duration was also tracked and delineated by the procedure time-out and the time of completion. The success rate was calculated by subtracting the number of aborted procedures from the total number of attempts, divided by the total attempts. Furthermore, reasons for aborting the procedure were documented and included clinical instability, inability to establish venous access, and inability to thread the catheter in place.
Post placement metrics included line dwell time and long-term complications. We defined a complication as either a deep or superficial venous thrombosis (VT), infection necessitating therapy or removal of the line, or technical difficulties including accidental removal or other damage to the line. All data were collected, tracked, and analyzed by members of the US-PICC and sedation teams. All data are from placement of US-PICCs, not other types of lines placed by other providers.
Results
In total, 968 US-PICC lines were placed at our institution during the study period. About 954 of those were the placement of an initial US-PICC line, with the remaining 14 being exchange of a new US-PICC over a wire or replacement of the initial US-PICC completely because of a complication or technical problem. The average patient age was 5.4 years. However, as shown in Figure 1, age was not normally distributed, with many of our patients in infancy. About 40% of lines were placed on infants below 1 year of age, of which the average age was 16 weeks (N = 384).
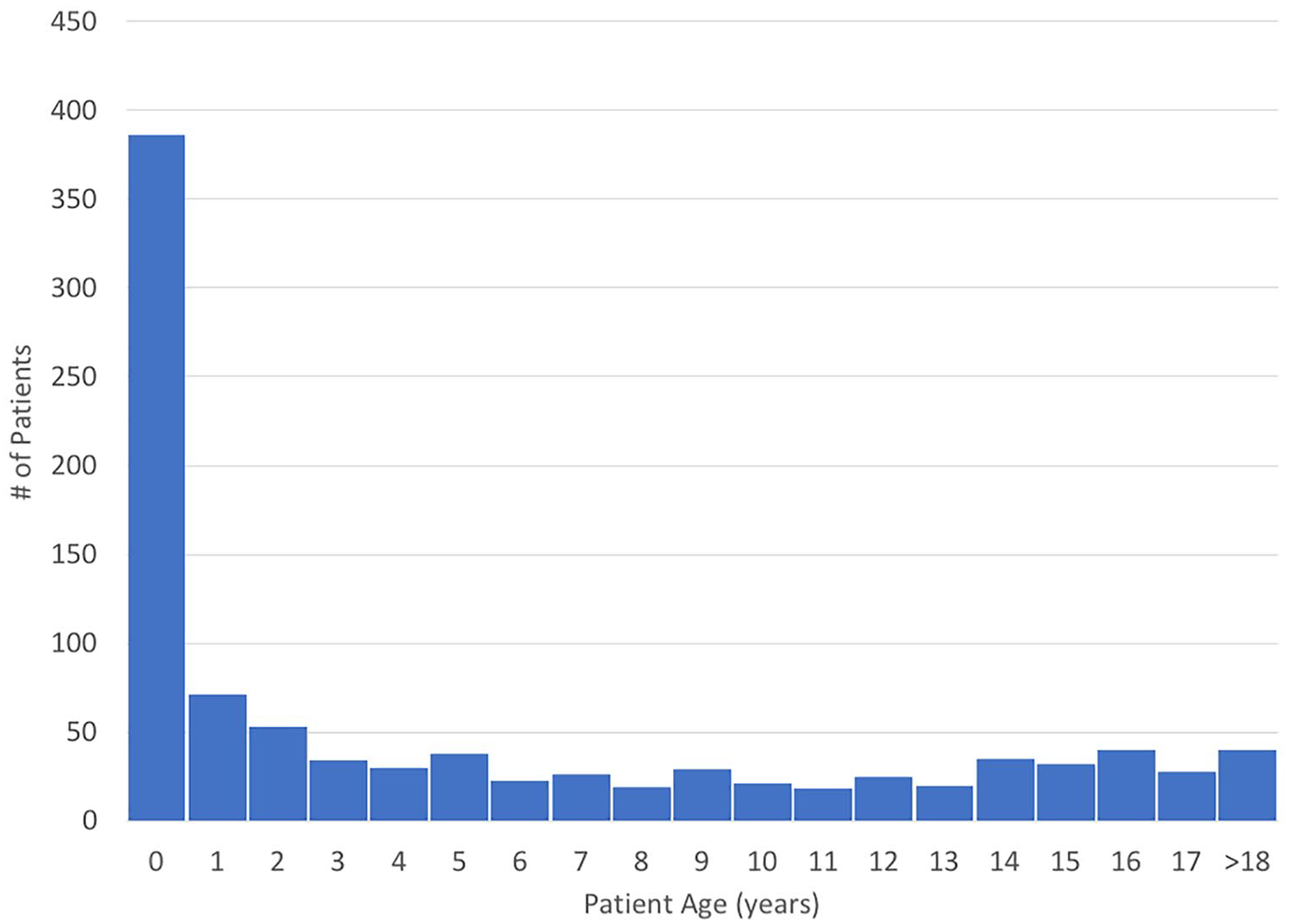
Distribution of patient age (N = 968). Patients less than age 1 are counted as age zero.
The reasons for US-PICC placement are shown in Figure 2. There was no limit on the number of indications that could be chosen for a line; therefore, multiple indications could be selected for each. The most common indication for placement was the need for long-term antibiotic therapy, followed by other indications as noted in Figure 2. Figure 3 shows the number of indications given for each US-PICC line; a single indication was most common, though 2 or 3 indications was not unusual.

Distribution of indications for ultrasound-guided peripherally inserted central catheter (US-PICC) line placement; 951 US-PICC had indications given, though more than 1 indication could be selected for each. IV indicates intravenous; TPN, total parenteral nutrition.

Number of indications given for each ultrasound-guided peripherally inserted central catheter line (N = 951).
Table 1 shows details regarding the placement of the US-PICC line itself. Regarding location of placement and use of sedation, this information was available on 961 of the lines. About 319 (33%) were performed with our sedation team, and an additional 202 (21%) were placed without sedation. These patients would have been on either the general floor, the intermediate unit, or outpatients; while this breakdown was not strictly tracked, the vast majority were on the general floor. Of the remaining, 27 (3%) were placed in the OR under general anesthesia, 400 (42%) in the pediatric ICU, and 13 (1%) in the neonatal ICU. In the ICUs, those patients were most commonly already sedated and intubated, or less commonly sedated by the attending physician rather than the sedation team.
Information on ultrasound-guided PICC placement location, sedation needs, timing of placement, and reasons for the procedure not being completed.
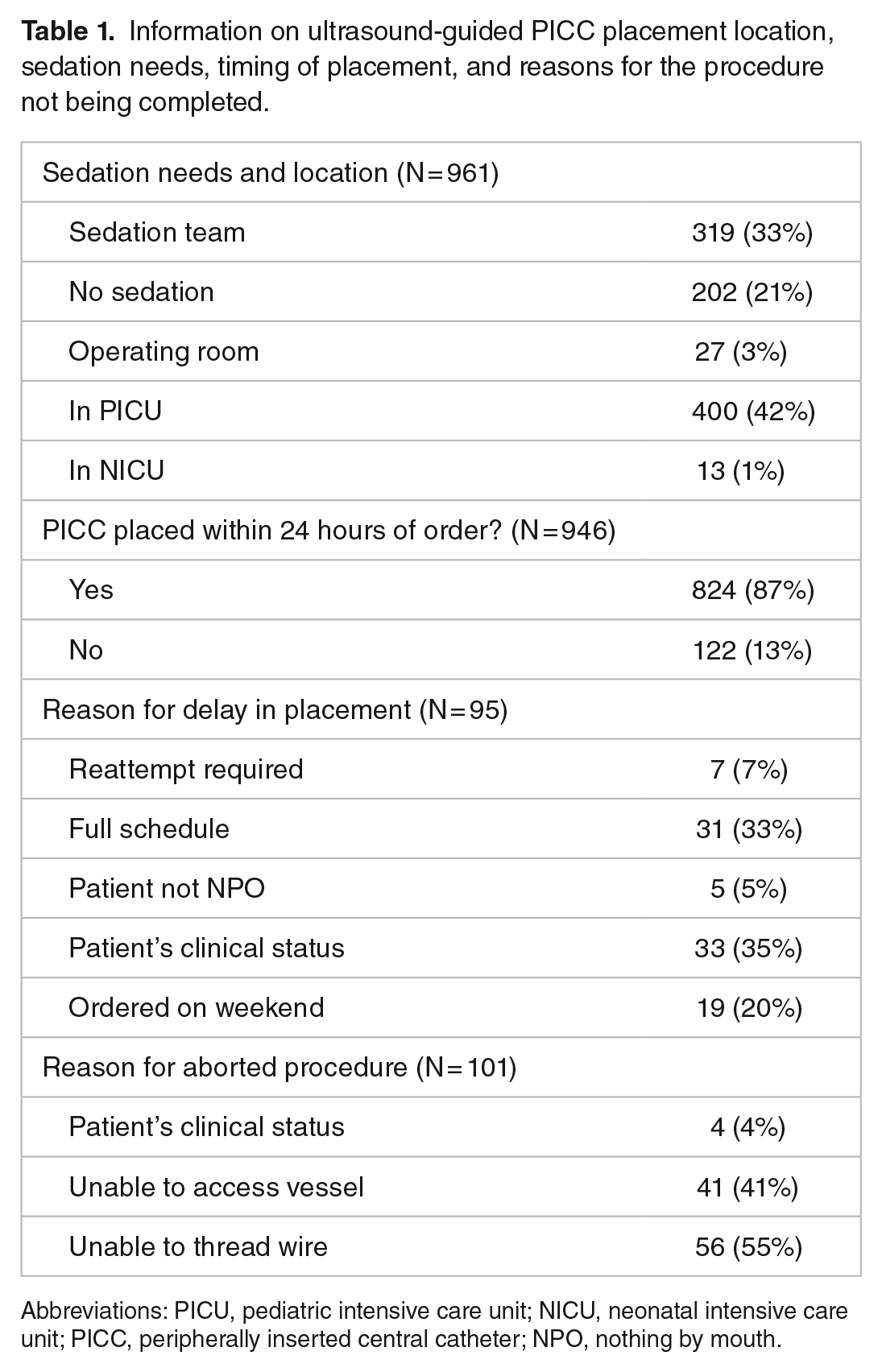
Abbreviations: PICU, pediatric intensive care unit; NICU, neonatal intensive care unit; PICC, peripherally inserted central catheter; NPO, nothing by mouth.
As shown in Table 1, we had information on time to placement on 946 lines, 87% of which were attempted within 24 hours of consultation. The most common reasons for delay in placement were the patient’s clinical status necessitating a delay or an already full schedule for the PICC and/or sedation team. US-PICC lines were successfully placed in 858 cases, for a completion rate of 89%. Of the 110 cases that were unsuccessful, the reason for failure was indicated in all but 9, the most common being inability to successfully access a vessel and inability to thread the guidewire fully. As shown in Figure 4, the majority of US-PICC lines were placed within 90 minutes.
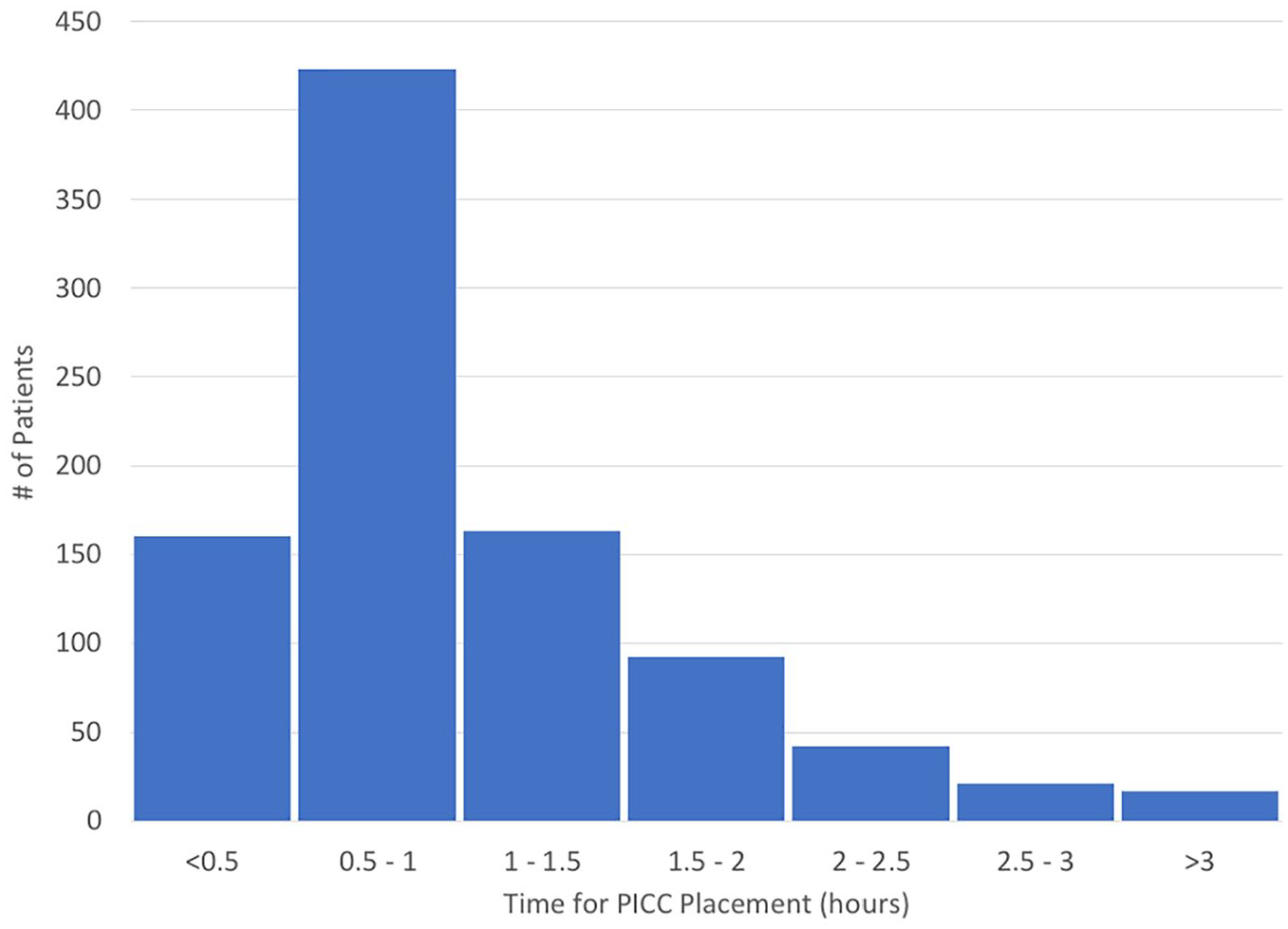
Duration of ultrasound-guided peripherally inserted central catheter procedure (N = 918).
Average dwell time was 23 days, though we only had this information for 773 of our lines. The longest dwell time noted in our study period was 200 days. Complications are shown in Table 2. We recorded both complications of the line placement itself and long-term complications that are of more clinical relevance. Long-term complications of any type were noted in 59 patients (6.1%). Regarding the most significant complications, deep and superficial VTs were noted in 10 and 7 patients, respectively (1.7% total rate). Line infection was identified and treated in 9 patients (0.9%).
Complications of ultrasound-guided peripherally inserted central catheter line placement.

Discussion
PICCs are increasingly utilized in pediatrics for consistent long-term venous access and are commonly placed by dedicated and specialized nursing teams. Recent data suggest that more than 60% of hospitals in the United States utilize designated nurse PICC teams, which has led to increasing PICC use in more diverse patient populations and indications. Use of these teams has also led to an increased adherence to infection control procedures and a decrease in rates of insertion complications. 3 Thus, PICC teams represent a progressively vital component of health care delivery.
While the data in adult populations support the benefits of designated nurse PICC teams, the data in pediatric patients are less well established.4-6,11 A specific limitation of US-PICC placement in the pediatric population is the frequent need for procedural sedation to ensure adequate motionlessness during catheter placement. This process often includes involving another physician service to coordinate sedation in addition to the US-PICC team and the primary service, which can lead to frustration and dissatisfaction among patients, their caregivers, and providers.
We present a unique model of service where our dedicated nurse US-PICC team is housed under our existing pediatric sedation service. Our team model starts with sedation certified nurses who then cross-train in US-PICC line placement. Training consists of shadowing and assisting the adult US-PICC team, completing training provided by the supplier of PICC equipment, and supervised pediatric US-PICC placement until a satisfactory number of encounters are completed. A unique advantage of this approach is that a single phone call allows the scheduler to plan US-PICC line placement with or without sedation based on the availability of the US-PICC nurse, sedation nurse, and sedation physician. To our knowledge, we are the first to describe our experience with a combined US-PICC line and sedation service model.
The data presented here suggest that our endeavor has thus far been a successful one. Our dedicated team placed more than 950 US-PICCs in a 5-year span, averaging more than 150 per year. For a medium-sized tertiary care pediatric center with just over 100 beds, this number is respectable compared with other institutions with higher bed volumes and greater patient catchment areas. 1 The incidence of VTs at our institution was low, encompassing only <2.0% of encounters, compared with 9.3% in a recent review. 2 Other studies have reported incidences of VTs in centrally inserted catheters between 18.3% and 35%, confirming the lower incidence of thrombotic events in peripherally inserted catheters, generally, and in our service model specifically.12,13 Infectious complications were also noted to be infrequent, with a central line–associated bloodstream infection (CLABSI) rate of 0.9%. Other authors report this metric as the number of infections per 1000 catheter days; however, in our population we did not have dwell times in about one fifth of our lines. However, using the average dwell time of 23 days and applying that to the whole cohort, our infection rate is about 0.40/1000 catheter days, well beneath the reported incidence of infectious complications noted in recent reviews between 1.0 and 2.6/1000 catheter days.14,15
While our observations are encouraging, they do have some limitations. First, we represent only one institution in the United States and our findings may not be applicable, generalizable, or easily implemented at other children’s hospitals. However, we are a medium-sized tertiary, academic pediatric care center that may share various characteristics with other children’s hospitals, including demographics, diversity of patient pathology, and indications for US-PICC placement. Furthermore, as with any quality review, data collection could be limited by incomplete documentation or unrecognized complications. However, being the main children’s hospital for our referral area ensures that US-PICC placement is almost exclusively performed in our institution and followed in our system, rendering adequate identification of complications much more likely. Finally, while our current outcomes are encouraging, further study is needed to define the potential benefits of our model on cost and resource utilization.
Conclusion
Our endeavor of creating a US-PICC team under the auspices of an already existing pediatric sedation service has been successful with regard to number of lines placed, team efficiency, and complication rates. Cross-training nurses in both sedation and US-PICC placement helps achieve success due to mutual cooperation, and housing the service under an existing sedation program allows efficient coordination of all probable aspects of the procedure. This approach may be beneficial to other institutions seeking to streamline patient care and maximize use of available resources.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GD, KH, HB, KC, AF, and KH conceptualized and designed the study. KH conducted the initial analysis. SCR drafted the initial manuscript and conducted the literature search. All authors reviewed and revised the manuscript for important intellectual content and approved the final manuscript as submitted.