
Abstract
With the use of seatbelts comes a unique injury profile that has been called “the seatbelt syndrome.” The classically described “seatbelt sign” has become a pattern of injury, describing potential underlying damage. As a clinician, clues to the underlying damage follow a thorough physical examination including the removal of all clothing to locate abrasions and bruises to the skin that potentially follow a seatbelt pattern. Delayed presentation of an intra-abdominal injury in the setting of a seatbelt sign has been well documented; however, the question is how long to observe these patients. We present the case of a 17-year-old woman involved in a motor vehicle collision who presented to the emergency department (ED) hemodynamically stable with a lower abdominal wall seatbelt sign. Her initial imaging revealed only an abdominal wall contusion. She was admitted for observation. Approximately 12 h later she started developing abdominal pain, and by 14 h abdominal distention, with repeat imaging showing free fluid and free air. She was taken to the operating room for an exploratory laparotomy and was ultimately discharged back home on day 7.
Keywords
Case Report
A 17-year-old woman with no significant past medical or surgical history presented to the emergency department (ED) as a level 2 trauma activation. The patient was a restrained backseat driver’s side passenger in a car traveling approximately 45 mph when a delivery truck ran a red light hitting the driver’s side. The front seat air bags did deploy. She denied loss of consciousness and was ambulatory at the scene. Emergency medical service (EMS) reported approximately 6 in of intrusion into the driver’s side door. Her only complaint on arrival was generalized body aches and abdominal pain. Her last menstrual period was 2 weeks prior to arrival.
Vitals on arrival to the ED are as follows: 97.2°F, blood pressure of 108/62 mm Hg, heart rate of 90 beats/min, respiratory rate of 19 breaths/min, and 100% pulse oximetry on room air. Her physical examination was notable for a horizontal abrasion across the abdomen below the level of the umbilicus consistent with a positive seatbelt sign. Multiple other abrasions were noted at the anterior left knee, anterior left shin, and left shoulder. Her remaining physical examination was unremarkable. A focused assessment with sonography for trauma (FAST) was negative. A subsequent computed tomography (CT) abdomen/pelvis with intravenous contrast only per trauma protocol (performed approximately 2 h from the time of the crash) demonstrated a contusion to the lower anterior abdominal wall with no other findings (Figure 1). Her laboratory evaluation was unremarkable, including lactic acid. Given the large contusion to the lower anterior abdominal wall and risk of delayed intra-abdominal injury, even with normal vitals and negative imaging, she was admitted to the trauma service for observation.
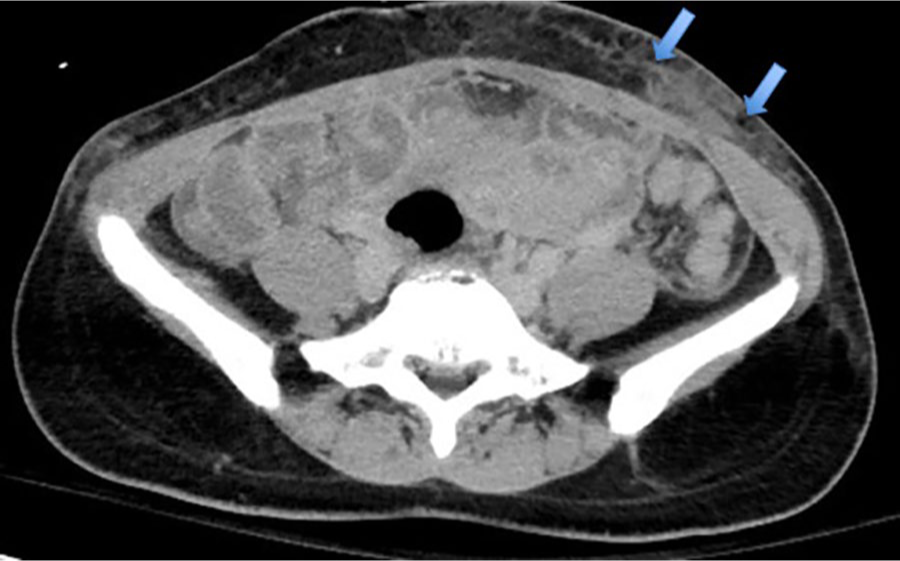
CT abdomen/pelvis with intravenous contrast per trauma protocol demonstrating a contusion to the lower anterior abdominal wall.
Hospital Course
Approximately 12 h later she developed worsening abdominal pain, and by 14 h, she had abdominal distention with the absence of flatus/bowel movements. Repeat vitals at 14 h are as follows: 99.2°F, blood pressure of 102/56 mm Hg, heart rate of 96 beats/min, respiratory rate of 21 breaths/min, and 100% pulse oximetry on room air. A repeat abdominal examination was notable for percussive tenderness to the bilateral lower quadrants. A repeat CT abdomen/pelvis with intravenous and oral contrast was performed showing new free fluid favoring extravasation of contrast and concern for perforation. There are a few punctate droplets of air seen within the peritoneal cavity (Figure 2). There is also some enhancement of the peritoneal wall suggesting peritonitis. The patient was taken to the operating room (OR), where she underwent an exploratory laparotomy, small bowel resection for a full-thickness perforation in the ileum, lysis of adhesions, and placement of JP drain x2. Her remaining hospital stay was uncomplicated, and she continued to improve clinically and was discharged on day 7.
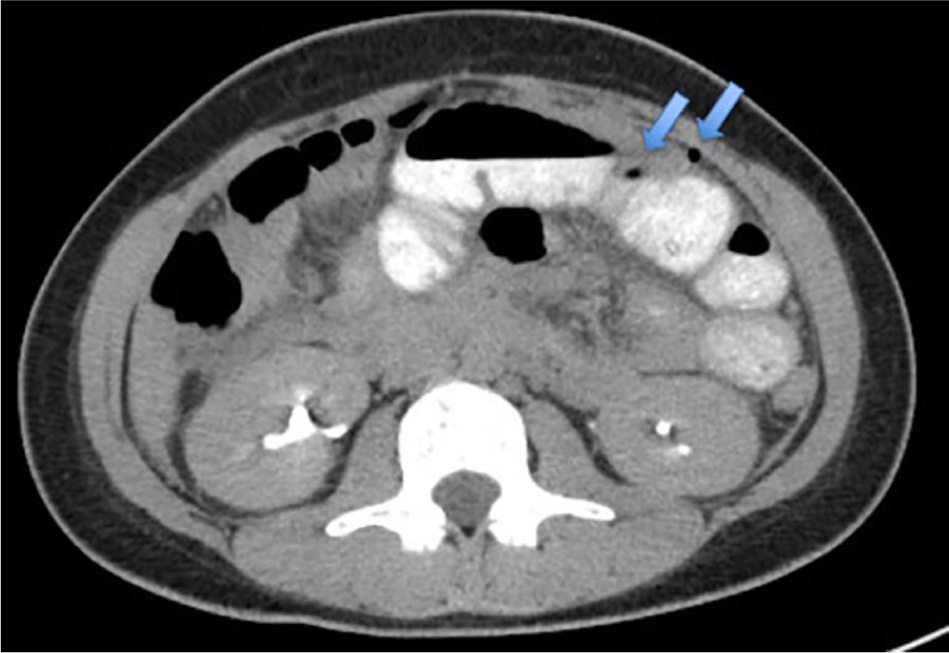
CT abdomen/pelvis with intravenous and oral contrast showing new free fluid favoring extravasation of contrast and concern for perforation. There are a few punctate droplets of air seen within the peritoneal cavity.
Discussion
As a clinician, clues to the underlying damage involve a thorough physical examination to locate abrasions and bruises to the skin that potentially follow a seatbelt pattern. In unstable trauma patients with abdominal injuries, the decision to proceed to the OR is rather straightforward. 1 However, in hemodynamically stable trauma patients with a seatbelt sign and negative initial imaging, trying to predict the potential internal injuries and clinical course of the patient relies on observation, repeated physical examinations, and repeat imaging if necessary.
Blunt abdominal trauma occurs most commonly in the setting of a motor vehicle accident and classified based on the mechanism of injury: deceleration force or compression force. 2 Compression occurs with a direct blow to the abdomen, such as from the seatbelt or steering wheel.2,3 The patient can suffer a hyperflexion injury around the abdominal restraint. A deceleration force causes shearing and stretching between mobile and fixed parts of the gastrointestinal intact. 2 The result is a high-pressure blowout to the intestines, resulting in bowel perforations and mesenteric injury. In addition, the chest restraint can result in fractures to the sternum, ribs, clavicle, and damage to major thoracic vessels.1,3
A retrospective analysis was performed between 2005 and 2010 at a level 1 trauma center involving 41 patients with a seatbelt sign that underwent a laparotomy. 1 The nature of the study was to correlate the pattern of injury with the patient’s clinical course and outcome. 1 The 41 patients were classified into 3 groups based on the timing of surgical intervention (immediate, early, and late). The immediate group consisted of 12 patients who were taken to the OR immediately within 30 min to 1.6 h. The early group consisted of 22 patients who were stable and underwent CT evaluation and ultimately required the OR within 1 to 12 h. The delayed group consisted of 7 patients who had negative initial imaging, were admitted and observed, with injuries identified later that required the OR (12-51 h). 1 The analysis found that most of the patients in the delayed group were backseat passengers (none of them were the driver) and younger (age 8-36 years). 1 Reasons for the delayed time to laparotomy included clinical deterioration (perforation of terminal ileum, proximal jejunum, and mesenteric injury found on laparotomy), repeat CT of the abdomen/pelvis revealing a small bowel perforation not evident on initial radiography, and pancreatic injury that required endoscopic retrograde cholangiopancreatography (ERCP). 1
Approximately 12% to 15% of blunt abdominal trauma patients with a seatbelt sign have underlying injuries within the abdomen.4,5 It is for this reason that if a patient has a positive seatbelt sign, even with normal vitals and unremarkable initial imaging, then they be observed for any subtle signs of bleeding, peritonitis, abdominal distention, or increasing pain. The issue is how long to observe these patients.
Borgialli et al, as published in The Journal of Academic Emergency Medicine, looked at the association between intra-abdominal injuries and the presence of a seatbelt sign in pediatric patients. There was a total of 3740 children (median age of 12 years) who suffered blunt torso trauma from a motor vehicle crash. 5 Approximately 585 patients had a positive seatbelt sign on the initial trauma assessment. Overall, nearly 15% of those with a positive seatbelt sign had underlying abdominal injuries with 6.8% of those requiring surgical intervention. 5 This study concluded that patients with a positive seatbelt sign were 4.5 times more likely to require acute intervention for intra-abdominal injuries and 9.5 times more likely to require a laparotomy. 5
In another case, a 31-year-old man presented after a motor vehicle accident. The patient had abdominal pain, low back pain, a positive seatbelt sign, and an abdominal CT that revealed only a tear to his abdominal wall musculature. Approximately 24 h later he had an increase in abdominal pain, tenderness, and exhibited tachycardia. Repeat CT revealed mesenteric fat stranding within the pelvis and a small amount of free fluid. Subsequent exploratory laparotomy showed a mesenteric injury and devascularization of the terminal ileum. 6
As we have demonstrated in our case and a few cases published within the literature, delayed presentation of an intra-abdominal injury in the setting of a positive seatbelt sign has been well documented; however, the issue is how long to observe these patients. A retrospective review, as published in the Journal of Trauma and Acute Care Surgery, involved 3574 patients at an academic level 1 trauma center that suffered blunt abdominal trauma between 2010 and 2012. 7 Jones et al 7 concluded that injuries in the setting of blunt abdominal trauma become clinically evident by 9 h. They found that all patients had a symptom or clinical sign within 9 h of the blunt trauma. 7
Conclusions
A patient presenting with abdominal wall ecchymosis after blunt abdominal trauma in the setting of a motor vehicle crash has an increased chance of having some type of intra-abdominal injury, regardless of the size of the seatbelt sign. Our patient demonstrated that patients with a seatbelt sign be observed for at least 12 h, an increase from 9 h as previously published in the Journal of Trauma and Acute Care Surgery, so as to not miss any potential intra-abdominal injury and risk discharging a patient too early. Our patient had normal vitals on arrival, an unremarkable laboratory evaluation, a negative FAST, and a negative CT scan, with only scattered abrasions and a horizontal lower abdominal seatbelt sign. A patient may be relatively asymptomatic, have stable vital signs, no clinical evidence for peritonitis, and even negative initial imaging. As a clinician, identifying the seatbelt sign is critical, rather you are evaluating a small seatbelt sign or even a patient ambulatory through triage. Performing a thorough physical examination, maintaining a high index of suspicion for potential intra-abdominal/thoracic injuries, and observing the patient for a delayed presentation are crucial in reducing morbidity and mortality.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Note
G.M.T. is the guarantor of this article. All the authors are physicians.
Author Contributions
All authors exhibited substantial contribution to the generation of this paper.
Informed Consent
Informed consent was obtained from the patients.