
Abstract
Background:
To accelerate access to pediatric HIV care in Cameroon, operational challenges in implementing HIV pediatric care need to be identified. The aim of this study was to assess the knowledge, attitudes, and practices of health care workers regarding pediatric HIV infection in Cameroon.
Methods:
A descriptive cross-sectional study was conducted over a 4-month period (April to August 2014) in 12 health facilities in 7 regions of Cameroon selected using systematic random sampling. Data were collected from interviews with health care providers and managers using standardized self-administered questionnaires and stored in the ACCESS software.
Results:
In total, 103 health care providers were included in this study, of which 59 (57.3%) were health workers and 44 (42.7%) community agents. Most of the health workers in charge of HIV pediatric care were nurses, requiring effective medical task shifting that was institutionalized in Cameroon. The knowledge of health care providers in relation to pediatric HIV care was acceptable. Indications for prescription of test for early infant diagnosis were known (96.1%), but their attitudes and practices regarding initiating antiretroviral therapy (ART) in infants less than 2 years (5.2%) and first-line ART protocols (25.4%) were insufficient, due to little information about standard procedures.
Conclusion:
Capacity building of health care providers and large-scale dissemination of normative national documents are imperative to improve HIV pediatric care in the health care facilities.
Introduction
Human immunodeficiency virus (HIV) infection remains a major concern in the world despite the progress recorded in the fields of Prevention of Mother To Child Transmission of HIV (PMTCT) and antiretroviral therapy (ART). 1 In 2012, Africa was the continent most affected by this infection accounting for 91% of HIV-infected children aged less than 15 years. 2 In 2006, the proven effectiveness of early initiation of ART in the first year of life on reducing HIV-related mortality in infants led the World Health Organization (WHO) to recommend routine ART initiation of all HIV-infected infants in 2013. 1 In 2015, this recommendation was, respectively, extended to the children greater than 5 years old and then to every HIV-infected person, irrespective of clinical and immunological stage.3–6 Moreover, the strategic United Nations AIDS (UNAIDS) 90-90-90 treatment targets aim to have 90% of people living with HIV (PLHIV) knowing their status, 90% ART coverage of PLHIV, and 90% of viral suppression for PLHIV on ART by 2020. 7 These rapidly changing treatment guidelines may contribute to provider confusion and limit knowledge of pediatric HIV care.
In resource-limited setting, the mean age at ART initiation was often late and varied between 4 and 9 years, after severe immunodeficiency had set in 70% of cases.8–10 In 2012, there was a substantial gap between treatment need and access to ART (34%) among the pediatric population, compared with adults (64%) in the 22 priority countries of the Global Plan.2–6,8–10 This worrisome situation required appropriate solutions and inspired the recommendations of the 2013 WHO pediatric ART guidelines. World Health Organization’s new recommendations raised a new challenge for early infant diagnosis (EID) and access to ART before the age of 24 months. In 2012, only 39% of HIV-exposed infants had access to EID services within the first 2 months of life. 11 Few health facilities developed activities for the care of children to the extent they did for adults. Health care teams, in insufficient numbers, were not trained enough in the field of pediatric HIV.12,13
In 2012, a small proportion of children in need of ART (15%) were actually on ART, compared with adults (49%) in Cameroon. This gap could be related to poor knowledge of pediatric HIV by health care providers in Cameroon. To accelerate access to pediatric HIV care in Cameroon, it seemed sensible to assess care practices in the health facilities. The aim of this study, therefore, was to assess the knowledge, attitudes, and practices of Cameroonian health care providers on pediatric HIV care.
Methods
Study design
A descriptive cross-sectional study was conducted from April 18 till August 19, 2014 (4 months) in 12 health care facilities offering pediatric HIV care in 7 regions of Cameroon (Center, East, Littoral, North, North-West, West, and South-West).
Selection of the 12 health care facilities
This was based on the assumption that health facilities located in the same environment and covering pediatric populations of similar sizes had the same type of organization and faced similar difficulties. Health care facilities were selected by using a combination of samples techniques: stratified and systematic random sampling. The following variables were considered for sample stratification: urban or rural location and weight of health care facilities. The latter was based on the number of HIV-infected children currently in care and organized in 5 categories: category I (<50 children), category II (between 50 and 150 children), category III (between 150 and 250 children), category IV (between 250 and 350 children), and category V (>350 children). Using the above criteria, the 137 health facilities caring for HIV-infected children in Cameroon were subsequently organized in 4 groups for simplification of sampling: group 1, categories I and II from urban setting (56 health facilities, n = 1728 children, 32%); group 2, categories III to V from urban setting (5 health facilities, n = 2069 children, 39%); group 3, categories I and II from rural setting (74 health facilities, n = 1277 children, 23%); and group 4, categories III to V from rural setting (2 health facilities, n = 324 children, 6%). In each group, health facilities were classified in increasing order based on the number of HIV-infected children currently in care. The sampling interval corresponded to the total number of children in care divided by the number of health facilities to be selected. The later was obtained by applying the percentage of children followed in each group to 12 health facilities: group 1 (n1 = 4), group 2 (n1 = 4), group 3 (n1 = 2), and group 4 (n1 = 1). The selection starting point was determined by pulling randomly a number between 1 and the sampling interval; the first health facility was the one whose accumulated number of HIV-infected children currently in care integrated this value. Finally, the 12 selected health care facilities included the following: 6 Approved Treatment Centers (ATC) belonging to 4 regional hospitals (Bertoua, Garoua, Bafoussam, and Bamenda) and 2 central hospitals (Laquintinie Hospital, Douala, and “Mother and Child Center of the Chantal Biya Foundation,” Yaoundé); 6 treatment units (TU) belonging to 1 regional hospital (South-West regional annex, Limbe) and 3 district hospitals (DH) in Littoral, South-West and North-West regions (“Cité des palmiers” DH, Douala, Kumba DH, Batibo DH), and 2 private hospitals in North-West region (Shisong Catholic Hospital and Mbingo Baptist Hospital, Bamenda).
Study population
Among selected health care facilities, the study population consisted of health care providers in charge of pediatric HIV care including physicians, nurses, psychosocial agents (PSA), community agents, pharmacy clerks, pharmacists, and psychologists who provided written informed consent.
Data Collection
Two standardized and anonymous auto-questionnaires were developed and validated during study preparation meeting including the main investigators and investigators from the Division of Operational Research in Health (DORH) of the Ministry of Public health and from the Center Pasteur du Cameroon (CPC): (1) The “operational level 2” auto-questionnaire administered to the health workers in charge of HIV pediatric care and (2) the “operational level 3” auto-questionnaire administered to community agents in charge of HIV pediatric care. During data collection, an interviewer was always available to guide if necessary the health care providers.
Procedures
The data were collected by 12 interviewers during a 4-months period (April to August 2014) and were entered in an “ACCESS” database by a data administrator of CPC Epidemiology and Public Health Service. The auto-questionnaires were distributed to the staff having consented to participate in the study. The completed auto-questionnaires were validated by the main investigator before data entry.
Ethical Considerations
The administrative authorizations of the Cameroonian Ministry of Public Health (references: No. D21-65/L/MINSANTE/SG/DROS/SPA of March 23, 2014) and various health care facilities were obtained. The study was also approved by the National Ethics Committee for Research in Human Health (No. 2014/03/477/CE/CNERSH/SP, March 29, 2014).
Variables
Using the auto-questionnaires administered to the staff in charge of HIV pediatric care in ATC/TU, the following data were collected: socio-demographic and occupational characteristics (age, sex, function in the health facility, initial training level, number of years at current post), type of services offered from pediatric HIV screening to HIV pediatric care, working conditions, knowledge, attitudes, and practices regarding pediatric HIV care (ART initiation; psychological, social, and nutritional support; HIV status disclosure; and transition to adult service).
Data Analysis
The data were described using frequency and corresponding proportions for categorical variables or medians with interquartile ranges (IQRs) for quantitative variables. The following proportions in relation to health care providers in charge of HIV pediatric care were estimated: knowledge on HIV infection (modes of HIV transmission to children, HIV diagnosis in children, principles of ART initiation, and prevention of opportunistic infections), counseling for HIV screening, and searching for HIV-infected children lost to follow-up. This descriptive analysis was conducted using R software, version 3.4.3.
Results
Study population
In total, 103 health care providers from 12 health care facilities participated in this study, of whom 59 (57.2%) were health workers and 44 (42.7%) community agents (Table 1). The median age of the staff was 39.0 years (IQR: 32.0-48.0) and most of them were women (73.9%). The median seniority at the current post was 4.4 years (IQR: 2.0-8.0). More than half (62.1%) of the staff in charge of pediatric HIV have been trained on pediatric HIV care.
Sociodemographic and occupational characteristics of health care providers in charge of HIV pediatric care (Cameroon, 2014), N = 103.
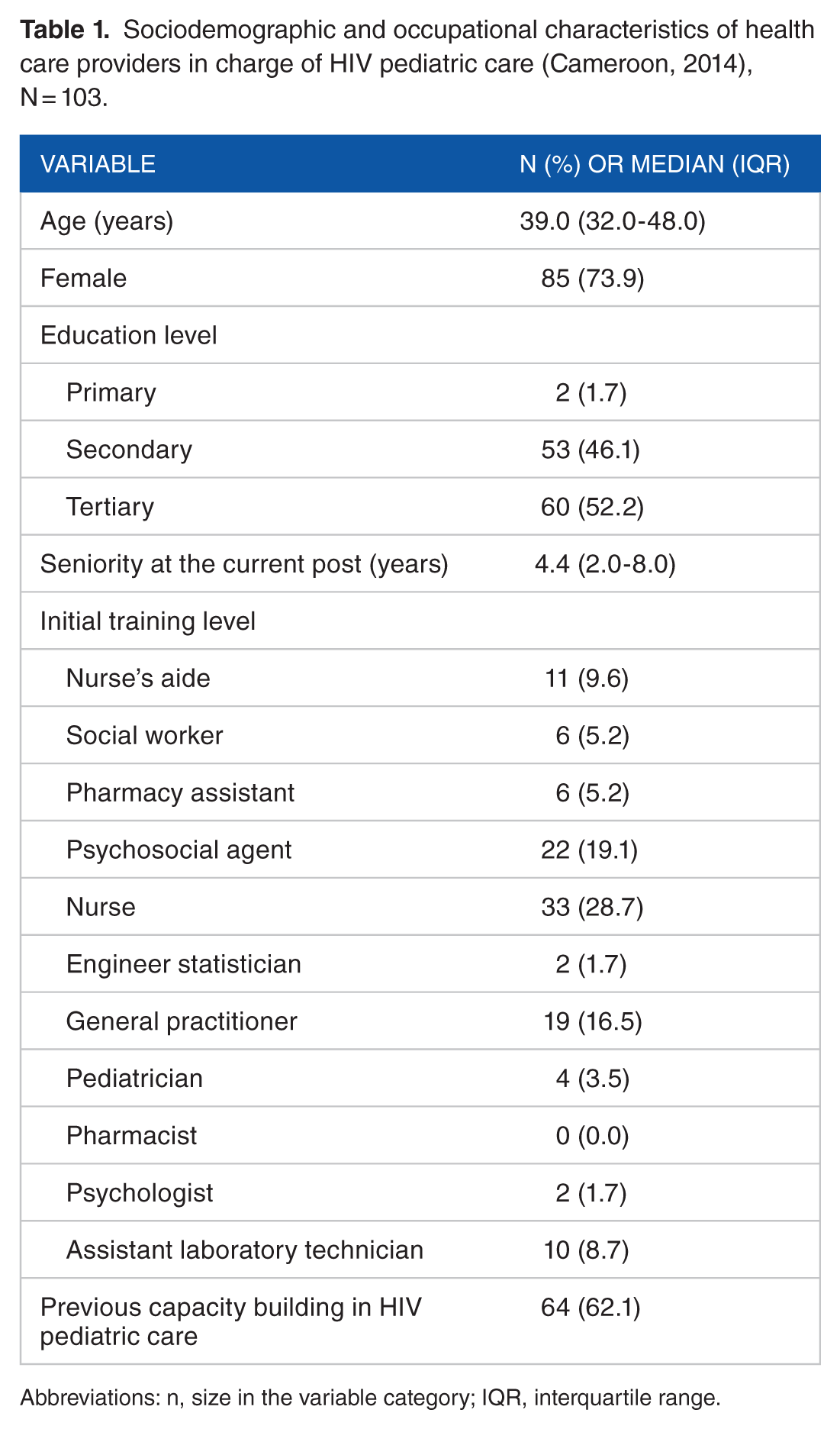
Abbreviations: n, size in the variable category; IQR, interquartile range.
Knowledge, attitudes, and practices of staff in charge of pediatric HIV
Pediatric HIV prevention and screening
Knowledge of the modes of HIV transmission in children was reported by health care providers as follows: mother to the child (98.1%) and sexual mode of transmission (34.0%). Only 20.5% of the community agents knew the sexual mode of transmission. Most of the staff interviewed (96.1%) reported that pediatric HIV infection is confirmed by a positive polymerase chain reaction (PCR). For health care providers, malnutrition and persistent cough consisted of symptoms of clinical suspicion of HIV in children in the respective proportions of (3.9%) and (1.9%). Counseling for HIV screening in children was reportedly practiced by 92.2% of health workers. Respondents reported the main indications of HIV screening to be HIV-exposed infants and sibling of HIV-infected child (85.4%), hospitalization for severe disease (45.8%), and acute severe malnutrition (ASM; 39.0%). In case of refusal of HIV screening by a parent, a discussion with the second parent, with consent from the first parent, was proposed by 47.6% of the health workers, while a minority (1.7%) reported that they will test the child for HIV without the consent of either parents. About 15.5% of participants reportedly did not carry out any specific activity to identify HIV-exposed infants in the labor room. Medical consultation for HIV-exposed or infected children was reportedly practiced by 76.7% of the health workers. The frequency of HIV-exposed-infants’ visits was reported to be monthly (50.0%) or adjusted to Expanded Program of Immunization (EPI) schedule (32.0%). Among the 47 health workers who implemented specific activities to track HIV-exposed infants, 18.4% of them reportedly used telephone calls (Table 2).
Knowledge, attitudes, and practices of health care providers in charge of HIV pediatric care (Cameroon, 2014).

Abbreviations: ART, antiretroviral treatment; ATC, approved treatment center; EPI, Expanded Program of Immunization; n, size of the variable in the category; NA, not applicable; PCR, polymerase chain reaction; PMTCT, prevention of mother-to-child transmission of HIV; TU, treatment unit.
Recommended attitudes and practices.
Initiation of ART in children
The initiation conditions for ART in HIV-infected children with a positive PCR result were reported by 79.7% of the staff. Other indications for initiation of ART were poorly known by providers, particularly children with serology HIV positive (35.6%) and children co-infected with HIV/TB (22.0%). Only 5.2% of staff knew that HIV-infected infants aged less than 2 years were an indication initiation of ART.
The initial ART regimen was prescribed by the health workers without seeking a second opinion (5.1%) or after preliminary validation by the adult therapeutic committee (52.5%), the pediatric therapeutic committee (35.6%), or the closest ATC/TU therapeutic committee (10.2%).
Follow-up of children on ART
On ART initiation, most of the respondents reportedly followed up the children monthly (62.7%), while the rest reported quarterly (20.3%), every 6 months (15.3%), or in case of disease (13.6%) follow-up. The CD4 count was prescribed every 6 months (83.1%) or not at all (8.5%). Viral load exam as a follow-up biomarker was not requested by 40.7% of the health workers. In health facilities offering therapeutic education (50.5%), 34.0% of the health care providers used educational tools. The HIV status disclosure was offered by 56.8% of the sampled health care facilities, and it involved essentially adolescents aged 11 to 17 years (52.3%). The main issues reported by the health workers in implementing this activity were reluctance of the parents/guardians (67.0%), insufficient health workers’ skills (13.6%), and lack of preparation of the child (14.6%). The criteria used to define lost to follow-up varied from 1 to 3 months of absence since the last medical appointment. Some health care providers (26.2%) did not track children lost to follow-up. The national medical file for HIV-infected children was available in the services according to 66.7% of health workers. Among the 66.7% of facilities that offered nutritional support services, 44.7% of them used therapeutic food with local products, either offered free of charge (33.3%) or paid for by the parents/family (44.7%).
Discussion
This is the first study, which aimed to assess the practices of pediatric HIV care in Cameroon. Most of the health workers in charge of pediatric HIV care were nurses, requiring effective medical task shifting, whose efficacy has been proven in Malawi 13 and was institutionalized in Cameroon in 2013. The median seniority at the current post was short (4.4 years [IQR: 2.0-8.0]), showing a high turnover of health care providers in the health care facilities. This situation could prevent health facilities to achieve their goals of care.
The knowledge, attitudes, and practices of health care providers were satisfactory in certain aspects of pediatric HIV care but needs to be strengthened. Many facility entry points (maternity, some pathological situations, sexual abuse) which would increase chances of finding pediatric HIV cases were not elicited by the health care providers interviewed, thus portraying some hesitation to propose HIV screening to families with unknown HIV status. Counseling for HIV screening introduced by the health care providers in the entry points of pediatric care is efficient in improving access to health care. 14 Knowledge on many aspects of curative care (ART regimens, management of HIV-tuberculosis co-infection and severe acute malnutrition, and HIV co-morbidities) was limited, translating to a lack of capacity. A little more than a third of health care providers did not receive capacity building in pediatric HIV care. According to 15.5% of health care providers interviewed, there was no specific activity useful in identifying HIV-exposed babies in the labor room. This observation could partly explain the huge proportion of HIV-exposed infants lost to follow-up between the maternity and ATC/TU services in the health care facilities offering EID of HIV. Clear directives must be developed to ensure the continuum of the care between these services. 15 Only 32.0% of health workers coupled HIV-exposed infants’ medical appointments with the EPI vaccination calendar. Nevertheless, this strategy has been strongly recommended in Cameroon since 2008, and studies have shown this strategy to be effective in facilitating the integration of services, reducing risks of stigmatization and decreasing lost to follow-up. 16 Therapeutic education activities remained weakly implemented in the health care facilities offering pediatric HIV care. This situation reflects the difficulty of health care providers in addressing frequent adherence issues among children on ART in resource-limited settings.17–19 Capacity building of health care providers is imperative to improve psychological and social support of HIV-infected children.
This study was conducted in only 12 out of 137 health centers in Cameroon in 7 of the 10 regions of the country. This could pose the problem of representativeness and generalization of results despite random sampling. An observational phase of practices could help minimize potential biases of prevarication or social desirability that could be observed in Knowledge Attitudes Practices (KAP) surveys. Notwithstanding the above, the findings of this study reflected the management practices of most health facilities in Cameroon due to the total number of HIV-infected children (approximately 43% [2257/5300]) on ART in Cameroon in the 12 health facilities included in the study and could be used for the operational plan to accelerate the management of pediatric HIV care.
Conclusions
The knowledge of health care providers of pediatric HIV care was acceptable, but their attitudes and practices were insufficient due to little information concerning the standard procedures. Capacity building of health care providers and large-scale dissemination of normative national documents are imperative to improve HIV pediatric care in health care facilities.
Footnotes
Acknowledgements
We are particularly grateful to the Ministry of Public Health (MOH) of Cameroon, the central- and intermediate-level officials, the health facility authorities of the study sites, and through them all the staff of the 12 CTA/UPECs team for their commitment and excellent collaboration. Our appreciations are also extended to institutions that contributed to the conduct of this study, particularly Pr Sinata Koulla Shiro (MOH), the Center Pasteur of Cameroon, the National Ethics Committee and Bordeaux School of Public Health/University of Bordeaux.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
All authors have contributed to this publication and hold themselves jointly and individually responsible for the content version.
Availability of Data and Materials
The datasets analyzed during this study are not publicly available but are available from the corresponding author on reasonable request.
Consent to Publish
All authors have agreed to the submission to Clinical Medicine Insights: Pediatrics and the manuscript is not currently under submission in any other journal.