
Abstract
Hypoglycemia is the most common metabolic disorder encountered in neonates. The definition of hypoglycemia as well as its clinical significance and management remain controversial. Most cases of neonatal hypoglycemia are transient, respond readily to treatment, and are associated with an excellent prognosis. Persistent hypoglycemia is more likely to be associated with abnormal endocrine conditions, such as hyperinsulinemia, as well as possible neurologic sequelae. Manifestations of hypoglycemia include seizures which can result in noteworthy neuromorbidity in the long haul. Thus, hypoglycemia constitutes a neonatal emergency which requires earnest analytic assessment and prompt treatment. In this review, we have tried to cover the pathophysiology, the screening protocol for high-risk babies, management, long-term neurologic sequelae associated with neonatal hypoglycemia, with evidence-based answers wherever possible, and our own practices.
Introduction
Physiology of glucose homeostasis
Glucose homeostasis in neonates needs harmony among use and generation of glucose. An increase in blood glucose concentration after meal results in increased insulin secretion which in turn stimulates the liver to store glucose as glycogen (Figure 1). Once the liver and muscle cells become saturated with glycogen, additional glucose is stored as fat. On the contrary, a decrease in blood glucose concentration stimulates glucagon secretion which activates glycogenolysis in the liver to release glucose back into the bloodstream. Amid starvation, the liver tries to keep up a normal glucose concentration by means of the process of gluconeogenesis, which involves framing glucose from amino acids and the glycerol. Muscle cells provide glycogen and protein to be separated into amino acids, which are then used as substrates for gluconeogenesis in the liver. Few vital organs including brain catabolize unsaturated fats to ketones, acetoacetate, and β-hydroxybutyrate and use them as fuel asset. The hypothalamus stimulates the sympathetic nervous system, causing secretion of epinephrine by the adrenal glands. This permits additional release of glucose from the liver. With prolonged and sustained hypoglycemia, growth hormone and cortisol are secreted, which decreases the rate of glucose utilization by the body. Promptly after birth, there is a sudden fall in blood glucose levels (BGLs) and as the pathways of glycogenolysis and gluconeogenesis are initiated because of the surge in levels of cortisol, catecholamines, and glucagon, BGLs increase within the first 1 to 2 hours of life. Subsequently, with the start of standard enteral feeds and initiation of hepatic gluconeogenesis process, BGLs get stabilized and euglycemia is attained, within 3 to 5 days of life.1–3

Glucose homeostasis.
Definition
Fetal brain receives a glucose concentration that is around 9 mg/dL lower than those of maternal plasma, so the actual glucose concentration in fetus is around 54 mg/dL. Soon after birth, with separation of placenta, there is a physiological decrease in the BGL of the newborn, with a nadir at around 1 to 2 hours of life.5–7 Therefore, the BGL which is considered to be “normal” is variable and depends on multiple factors including birth weight, gestational age, body stores, feeding status, availability of energy sources, as well as presence or absence of disease.2,8 There is no universal definition for hypoglycemia. 9 To date, we have failed to predict an evidence-based operational threshold for neonatal hypoglycemia to prevent subsequent neurologic sequelae. We take 45 and 50 mg/dL as cutoff values to treat hypoglycemia for term and preterm neonates, respectively. Following these guidelines, we have not seen any neurologic sequelae in our cohort of neonates with asymptomatic hypoglycemia (unpublished data). Based on the current evidence available in the literature, the concentration of blood glucose at which one should consider intervention is considered as the operational threshold for hypoglycemia.10,11 Hussain 12 suggested various operational thresholds for therapeutic intervention based on the clinical scenario such as blood glucose concentrations <45, <63, and <36 mg/dL for symptomatic newborns, for hyperinsulinemia newborns, and for at-risk neonates, respectively. Stanley and Baker 13 postulated that there should be no difference in cutoff value between a neonate and a child and common cutoff should be 60 mg/dL. World Health Organization defines hypoglycemia as “blood glucose level (BGL) of less than 45 mg/dL.” 9
Classification and Causes of Neonatal Hypoglycemia
Neonatal hypoglycemia is broadly divided into transient and persistent types, mainly based on the duration of hypoglycemia (Table 1).12–14
Causes of hypoglycemia in neonates.

Copyright: Aakash Pandita.
Types of transient hypoglycemia
Early transitional-adaptive hypoglycemia. It occurs due to early adaptive responses to birth process (↓ glycogenolysis and gluconeogenesis and ↑ insulin secretion; Table 2).11,15 Examples of this type include infants born to mothers who received excessive glucose infusion intrapartum, infants of diabetic mothers (IDMs) (↑ insulin), infants with hypothermia (↑ glucose utilization), asphyxiated infants (↑ anaerobic metabolism of glucose, glycogen depletion), and preterm infants (↓ glycogen stores).
Secondary-associated hypoglycemia. This is often secondary to a variety of associated illnesses, which include disorders of the central nervous system, such as perinatal asphyxia, intracranial hemorrhage, and congenital anomalies. Other disorders associated with this type of hypoglycemia are sepsis, cold injury, and congenital heart disease. The nervous system disturbance associated with this type of hypoglycemia may have an adverse impact on the regulation of hepatic glucose production.
Classic transient neonatal hypoglycemia. This type of hypoglycemia is typically seen in small for gestational age (SGA) infants, who are also predisposed to polycythemia. Small for gestational age infants have inadequate stores of energy and defective gluconeogenesis. Furthermore, there is excessive glucose utilization because of brain sparing (major consumer) compared with the liver (major producer). Most of these infants are symptomatic (80%).
Types of hypoglycemia.

Copyright: Aakash Pandita.
Screening for Hypoglycemia
Blood glucose concentrations should not be measured in healthy asymptomatic term infants born after an uncomplicated pregnancy and delivery. Blood glucose is required for at-risk infants or infants who demonstrate signs and symptoms suggestive of hypoglycemia. 14
Infants at risk of hypoglycemia are as follows14,16:
Preterm infants with gestational age less than 37 weeks;
Infants who are large for gestational age;
Infants with fetal growth restriction;
IDMs;
Infants who have experienced perinatal stress due to
• Birth asphyxia/ischemia • Erythroblastosis fetalis • Polycythemia
Infants who require intensive care;
Infants whose mothers were treated with β-blockers or oral hypoglycemic agents;
Family history of a genetic form of hypoglycemia;
Congenital syndromes (eg, Beckwith-Wiedemann) and abnormal physical features (eg, midline facial malformations and microphallus) associated with hypoglycemia.
Screening protocol
Optimal timing and intervals of glucose monitoring is still a debatable issue (Table 3). Timing and duration of monitoring for hypoglycemia depends on the risk factors, such as IDMs are prone to early hypoglycemia, namely, 1 to 2 hours and rarely their hypoglycemia extends beyond 12 hours (range: 0.8-8.5 hours), whereas in preterm and SGA neonates, the hypoglycemia risk may extend up to 36 hours (range: 0.8-34.2 hours). Feeding should start by 1 hour and then sugar should be checked 2 to 4 hours after this feed, just before the second feed. However, if the baby is symptomatic, than sugar check has to be immediate11–16 (Table 3).
Screening schedule for hypoglycemia.

Clinical Manifestations
Most of the infants with low blood glucose concentrations are asymptomatic, and hypoglycemia in these infants is usually detected during screening for hypoglycemia in at-risk infants. In the symptomatic infant, signs are nonspecific and reflect responses of the nervous system to glucose deprivation. These can be categorized as neurogenic or neuroglycopenic findings.11–16
Neurogenic (autonomic) symptoms result from changes due to neural sympathetic discharge triggered by hypoglycemia:
Jitteriness/tremors;
Sweating;
Irritability;
Tachypnea;
Pallor.
Neuroglycopenic symptoms are caused by brain dysfunction from impaired brain energy metabolism due to a deficient glucose supply:
Poor suck or poor feeding;
Weak or high-pitched cry;
Change in level of consciousness (lethargy, coma);
Seizures;
Hypotonia.
Along with these symptoms infants may also present with apnea, bradycardia, cyanosis, and hypothermia. As these findings are nonspecific, further evaluation for other possible causes (eg, sepsis) should be conducted if symptoms do not resolve after normalization of the blood glucose concentration. Abnormal behaviors related to feeding such as demanding frequent feeds, not waking for feeds, and not sucking effectively should be investigated for hypoglycemia.
Recently, British Association of Perinatal Medicine published guidelines recommend measurement of blood glucose for any infant who has any one of the following features 14 :
Perinatal acidosis (cord arterial or infant pH <7.1 and base deficit ≥−12 mmol/L);
Hypothermia (<36.5°C) not attributed to environmental factors;
Suspected/confirmed early onset sepsis;
Cyanosis;
Apnea;
Altered level of consciousness;
Seizures;
Hypotonia;
Lethargy;
High-pitched cry.
Diagnosis of Hypoglycemia
Point-of-care glucose meters are used as a rapid screening method in most of the nurseries. But these glucose meters show large variations in values compared with laboratory methods, especially at low glucose concentrations, and are of unproven reliability to document hypoglycemia in newborns.14–16 So, it is important to stress on the fact that although glucometers are used for screening, all low values need to be confirmed by lab to make the diagnosis of hypoglycemia certain. Likewise, laboratory confirmation of the plasma glucose concentration should be performed in any infant who shows signs consistent with hypoglycemia. However, treatment should be started immediately after the blood sample is obtained and before confirmatory results are available. Laboratory measurement of glucose concentration is affected by the type of the sample. Glucose concentration measured in whole blood is approximately 15% lower than that in plasma and may be further reduced if the hematocrit is high. Prompt analysis should be performed because delays in processing and assaying glucose can reduce the glucose concentration by 18 mg/dL/h (0.3 mmol/L/h) due to red cell glycolysis. 10 Thus, to avoid errors in estimation, blood sample for estimation of glucose should always be sent in sodium fluoride vial. Continuous glucose monitoring using a sensor that measures interstitial glucose concentration was reported to be reliable (when compared with blood glucose measurement), safe, and tolerable.16–18 However, it is unclear how to interpret the clinical significance of low interstitial BGLs and whether treatment should be initiated. Further studies are needed to determine whether continuous interstitial glucose monitoring has a useful role in the screening and management of neonatal hypoglycemia.19–28
Managing Asymptomatic Hypoglycemia
Management plan for asymptomatic hypoglycemia based on blood sugar level (BSL) is summarized in Table 4 (Figure 2). Repeated boluses of 10% dextrose should be avoided as it predisposes to rebound hypoglycemia by causing an increase in insulin levels.
Treatment of asymptomatic hypoglycemia.


Management of hypoglycemia.
Oral feeds—issues
Always direct breastfeeding should be tried first and expressed breast milk may be given if the infant is unable to suck properly. The advantage with breast milk is that it promotes ketogenesis which serves as an alternate source of energy for the brain. Formula feeds should be given only if the breast milk is not available. 14
Management of Symptomatic Hypoglycemia
A 2 mL/kg of 10% dextrose (200 mg/kg) has to be given to newborn children with symptomatic hypoglycemia, keeping in mind the end goal to quickly rectify BGL. The bolus needs to be followed by a glucose infusion rate (GIR) of 6 to 8 mg/kg/min. Regardless of bolus and GIR, if BGL remains beneath 45 mg/dL, GIR has to be increased in increments of 2 mg/kg/min every 15 to 30 minutes until a maximum of 12 mg/kg/min. Blood glucose level has to be observed every 30 to 60 minutes till glucose level is >50 mg/dL for 2 back-to-back readings, and afterward every 4 to 6 hourly until the point when the baby is off intravenous dextrose and is on full feeds. Following 24 hours of intravenous dextrose treatment, once at least 2 successive BGLs are >50 mg/dL, the GIR can be decreased at the rate of 2 mg/kg/min at regular intervals of 4 to 6 hours with BGL monitoring. Decrease in GIR must be joined by attendant increment in oral feeds. Once a rate of 4 mg/kg/min of GIR is accomplished, oral feed is sufficient, and the BGLs are reliably >50 mg/dL, the GIR can be halted (Figure 2). It is essential to guarantee nonstop glucose infusion ideally using an infusion pump and with no interruption. Utmost care should be taken and one should try not to stop glucose infusion unexpectedly, as extreme rebound hypoglycemia may happen. Furthermore, one should abstain from using more than 12.5% dextrose infusion through a peripheral vein because of the danger of thrombophlebitis.20–22 It is always a better idea to have 2 functional intravenous sites every time when one treats a hypoglycemic neonate so that in case one becomes nonfunctional the other one can be used without interruption of the infusion. Different groups practice different guidelines for the management of hypoglycemia. In Table 5, we provide different guidelines being practiced across the world including the recent guidelines by British Association of Perinatal Medicine. No guideline distinguishes between a term and a preterm neonate for the management of hypoglycemia.
Guidelines for the management of hypoglycemia.

Abbreviation: AAP, American Academy of Pediatrics; BSL, blood sugar level; NNF, National Neonatology Forum of India; PES, Pediatric Endocrine Society.
Copyright: Aakash Pandita.
Persistent Hypoglycemia
Persistent hypoglycemia is defined as persistent low plasma glucose concentrations beyond the first 7 days of life.10,11 This waiting period of at least 7 days is necessary because it is difficult to distinguish newborns with a pathologic hypoglycemia disorder (transient or permanent) from normal newborns. Hyperinsulinism is characterized by inappropriate secretion of insulin in the presence of low plasma glucose. It is the most common cause of persistent hypoglycemia in the neonates. Other less common causes of persistent hypoglycemia are counterregulatory hormone deficiency, defects in gluconeogenesis and glycogenolysis, galactosemia, and hereditary fructose intolerance.
Diagnosis of Hyperinsulinism
Hyperinsulinism is diagnosed based on the presence of the following features 29 (Table 6):
Inadequate suppression of insulin secretion in the presence of hypoglycemia;
Low levels of plasma free fatty acids and ketones (insulin suppresses lipolysis and ketogenesis);
Glycemic response (within 30 minutes of administration of glucagon at the time of the hypoglycemic event) of greater than 30 mg/dL which indicates the presence of adequate hepatic glycogen stores.
Diagnostic criteria of hyperinsulinemic hypoglycemia (at blood glucose <50 mg/dL).

Glucagon may be given intravenously at 0.03 mg/kg.
When BHB is low and FFAs are high, disorders of fatty acid oxidation or defects in carnitine metabolism should be excluded. Within 48 hours of birth, BHB and FFAs are difficult to assess because of the physiological hyperinsulinemia state. In some cases, hyperinsulinemia may not be the only cause of hypoglycemia and other comorbidities should be considered.
Other investigations for identification of cause of hyperinsulinism include the following:
Serum ammonia for hyperinsulinemic hyperammonemic hypoglycemia caused by activating mutation of glutamate dehydrogenase;
Plasma acylcarnitine profile and urinary organic acids (increased plasma 3-hydroxybutyrylcarnitine and urine 3-hydroxyglutarate) for congenital hyperinsulinism (CH) caused by mutation in short-chain 3-hydroxyacyl CoA dehydrogenase enzyme;
Genetic testing for molecular diagnosis of CH adapted from Yorifuji et al. 29
Management
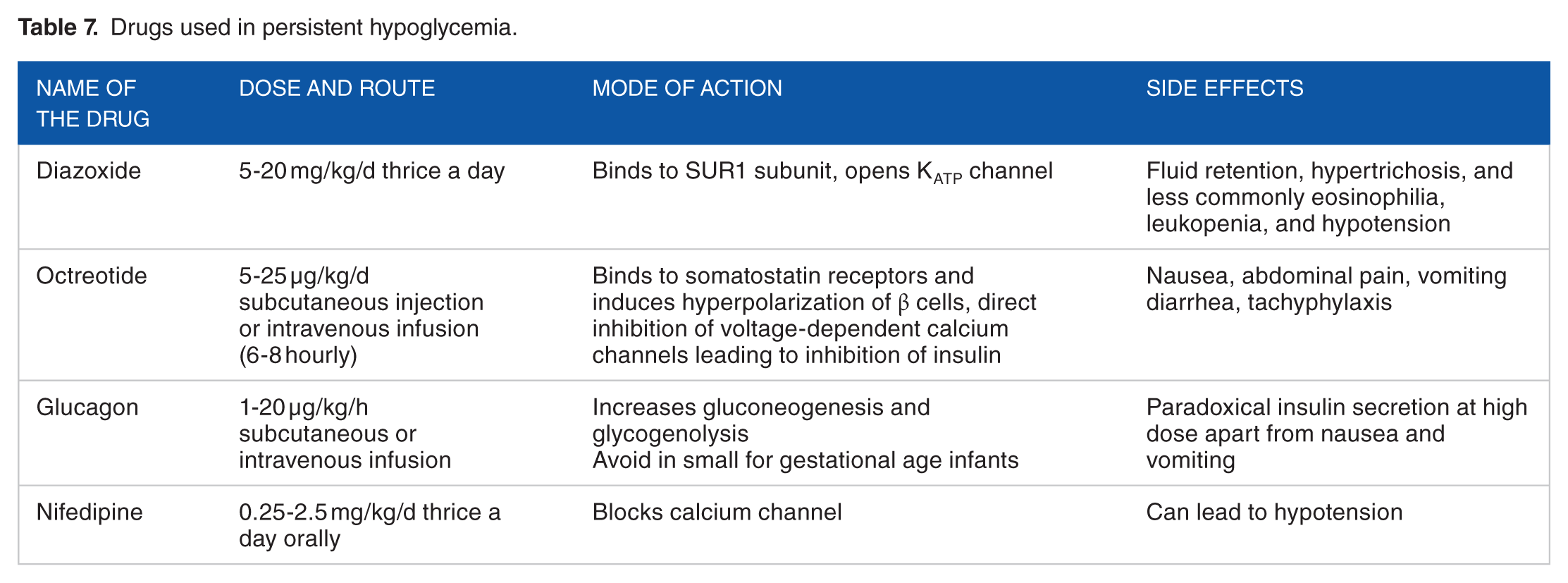
Hyperinsulinemic hypoglycemia is managed with drugs and surgical treatment is considered in cases which fail to respond to medical management. Drugs used in the management of hyperinsulinemic hypoglycemia include diazoxide, somatostatin analogues such as octreotide and sirolimus, glucagon, and nifedipine30–35 (Table 7).
Drugs used in persistent hypoglycemia.
Surgical treatment is warranted in patients who fail to respond to medical management. Surgery can be curative in patients with focal lesions. However, infants with diffuse disease may require a near-total pancreatectomy with or without drug therapy and frequent feeding to maintain euglycemia.
Neurodevelopmental Outcome
Hypoglycemia is known to cause long-term neurologic impairment dependent on the severity and duration of hypoglycemia.14,36 There is conflicting evidence regarding the extent of injury hypoglycemia causes in both preterm and term infants (Table 8).
Long-term prognosis of hypoglycemic infants (blood sugar level <47 mg/dL): CHYLD study. 37

Abbreviations: CHYLD, Children with Hypoglycemia and Their Later Development; CI, confidence interval; RD, risk difference, RR, risk ratio.
Symptomatic hypoglycemia
Hypoglycemia-induced brain injury can be detected by magnetic resonance imaging (MRI). However, there is paucity of data regarding the threshold level and duration of hypoglycemia that is known to be associated with brain damage detected by MRI. It is important to stress on that neonatal hypoglycemia should be aggressively treated because of the risk of its adverse effects.36,38
Asymptomatic hypoglycemia
A retrospective observational study reported infants with transient neonatal hypoglycemia (<40 mg/dL) after adjusting for confounding factors to have lower scores for literacy and math at fourth grade. 39
Preterm infants
Similar to term infants, studies report neurodevelopmental impairment due to asymptomatic episodes of hypoglycemia in preterm patients. We use a higher cutoff for preterm neonates (50 mg/dL) based on the following evidence. A multicenter retrospective data in preterm infants showed a correlation between prolonged hypoglycemia (plasma glucose <47 mg/dL [2.6 mmol/L] and lower Bayley mental and psychomotor scores at corrected age of 18 months. 40 Cerebral palsy or developmental delay was 3.5 times greater (95% confidence interval [CI]: 1.3-9.4) in the hypoglycemic infants. However, only arithmetic and motor scores were lower in hypoglycemic infants at 7.5 to 8 years of age. 41 Furthermore, long-term neurodevelopment impairment may be greater in preterm infants with repeated hypoglycemic episodes who are also SGA. In coherence to the above fact, a smaller head circumference at 18 months corrected age and lower psychometric testing scores at 3.5 and 5 years of age were reported in a prospective study of 85 SGA preterm infants with repeated episodes of hypoglycemia. 42 Another large prospective cohort involving neonates >35 weeks did not report any difference in neurosensory or processing impairment at 2 years of age, among children with neonatal hypoglycemia (BSL <47 mg/dL) and those without neonatal hypoglycemia (risk ratio [RR]: 0.95; 95% CI: 0.75-1.20; P = .67). Neurosensory impairment was defined as any of the following findings: developmental delay (BSID-III [Bayley Scales of Infant Development III] cognitive or language composite score of <85), motor impairment (BSID-III motor composite score of <85), cerebral palsy, hearing impairment requiring hearing aids, or blindness in both eyes. Another important finding of the study was children with BSL lying outside the range of 54 to 72 mg/dL were more prone to increased neurosensory impairment. With increase in the duration of time, the BSL was outside this range, the more was the impairment risk for neurosensory impairment (RR: 1.40; 95% CI: 1.09-1.79; P = .008). Furthermore, neonates with hypoglycemia who went on to develop neurosensory impairment, especially cognitive delay had a steeper rise of glucose levels for first 12 hours of birth, compared with neonates with no impairment (mean difference: 4.9 mg/dL; 95% CI: 1.4-8.3 mg/dL; P = .007). 43 Similar findings have been reported in animal studies in the past. 44 Follow-up (CHYLD [Children with Hypoglycemia and Their Later Development]) study at 4 years involving neonates ≥32 weeks of gestation also did not report any difference in primary outcome between hypoglycemic and euglycemic neonates (37.4% vs 38.5%; risk difference: 0.01; 95% CI: −0.07 to 0.10 and RR: 0.96; 95% CI: 0.77-1.21). In post hoc analysis, the risk of a low executive function score and a low visual motor integration score was highest in neonates with severe hypoglycemia and in neonates exposed to at least 3 episodes of hypoglycemia, respectively 37 (Table 8). The impairment was more in neonates with severe (<36 mg/dL) or recurrent hypoglycemia (>2 episodes).
Conclusions
Neonatal hypoglycemia is a common condition. It is more common in certain high-risk groups such as infants who are sick, septic, hypothermic, preterm, SGA infants, asphyxiated, infants born to diabetic mothers, and large for gestation age infants. It is important to recognize hypoglycemia to initiate prompt treatment and prevent long-term neurologic impairment. It is mostly asymptomatic but prompt recognition is important to achieve optimal neonatal outcomes. Furthermore, one should avoid giving repeated boluses while managing a neonate with hypoglycemia. A low blood sugar with glucometer should not delay treatment but should always be confirmed with laboratory value and the sample should be sent in a fluoride vial. Although there is a robust evidence that very low BSL is associated with neurologic impairment, the line of demarcation between normal and abnormal is still bleak. The answer to this question lies in a good-quality multicenter randomized controlled trial.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
VRK and AP wrote the manuscript and did final corrections. AP and GG did the critical appraisal of the manuscript. All the authors accepted the final corrections.