
Abstract
Background:
Breast milk contains all the nutrients infants need for their first 6 months of life. However, only a minority of Saudi Arabian mothers exclusively breastfeed, so the influencing factors must be examined to encourage more to do so. The study aimed to determine the prevalence of exclusive breastfeeding at 6 months and its associated factors in Tabuk, North West Saudi Arabia.
Methods:
A total of 589 mothers of healthy infants aged between 6 and 24 months were interviewed while attending Well-Baby Clinics within 5 primary health care centers. Interviews deployed a structured questionnaire to collect sociodemographic information and detailed data concerning breastfeeding practices. A logistic regression analysis was then performed on the data to identify the factors independently associated with exclusive breastfeeding practice for infants at 6 months.
Results:
Exclusive breastfeeding was practiced by 31.4% of mothers for the first 6 months of their infant’s life. The logistic regressions indicated that exclusive breastfeeding at 6 months was less likely to be practiced by working mothers, Saudi nationals, and for babies born via cesarean delivery or at low birth weights. Conversely, the mother’s awareness of the recommended exclusive breastfeeding duration was positively associated with exclusive breastfeeding.
Conclusions:
Programs promoting 6 months of exclusive breastfeeding should target high-risk groups. Two factors identified by this study are modifiable: working mothers and mothers’ awareness of the exclusive breastfeeding duration recommendation. Strategies to improve exclusive breastfeeding rates should therefore focus on workplace facilities and increasing awareness of the exclusive breastfeeding recommendation.
Introduction
There is general consensus that breast milk provides the best nutrition for healthy infants as it contains the complete range of nutrients required by infants for healthy growth and development in their first 6 months of life.1–3 In addition to these nutrients, breast milk also encourages increased resilience against infections, boosts infants’ neurodevelopment, and reduces the likelihood of infant with noncommunicable diseases such as cardiovascular disease, diabetes, obesity, and hypertension later in their life.4,5 Because of these benefits, the World Health Organization’s (WHO) current recommendation is that all mothers should feed their infants solely with breast milk, exclusive of any other nutritional sources, for the first 6 months of their infant’s life. 6
Research studies to date examining breastfeeding practices in both developed and developing countries have found high rates of breastfeeding initiation and also that this high initiation rate is accompanied by a steep fall in exclusive breastfeeding in the first 6 months of life.7,8 Taking Australian data from 2004 to 2005 as an example, although a high initiation rate of 92% was found for exclusive breastfeeding, the rate then dropped to 71% of infants who exclusively breastfed at 1 month of age, 56% at 3 months, and 14% at 6 months. 9 Similarly, in Saudi Arabia, findings from a research study indicate that 77.8% of infants began exclusive breastfeeding within 24 hours, falling sharply to 32.9% at 2 months of age, 19.2% at 4 months, and 12.2% at 6 months. 10
Extensive research has examined this pattern of changes in breastfeeding practice during the first 6 months of an infant’s life, and various studies have explored the most influential factors in relation to exclusive breastfeeding from among sociodemographics (such as parents’ education levels, living rurally or in a city, income level, and parity), biosocial factors (including the available support for breastfeeding), culture (such as breastfeeding attitudes and social norms), and employment law and policy.10–12 The relative influence of each factor differs across different nations and regions, over time, and even within population subgroups.10,11,13
A recent review by Al Juaid et al 14 in the Saudi Arabian context found a scarcity of data relating to the prevalence and predictors of exclusive breastfeeding and also that these vary between and within the different provinces of Saudi Arabia. Two different studies, one conducted by Amin et al 10 in 2011 and the other by El-Gilany et al 15 in 2011, illustrate this disparity in results. Both research studies aimed to assess the prevalence and predictors of exclusive breastfeeding at 6 months in Al-Hassa, Saudi Arabia. Amin et al found that 12.2% of mothers practiced exclusive breastfeeding for the first 6 months of their infant’s life, whereas El-Gilany et al reported a prevalence of 24.4%. These 2 studies examined various common factors, and several of these were associated with exclusive breastfeeding, ie, breastfeeding initiation, residence, and employment status. However, they disagreed on some of the other factors (such as mother’s age, educational status, number of children, and family income) and reported conflicting associations with exclusive breastfeeding in relation to them.
The clear variations in previous findings with regard to the prevalence and possible predictors of exclusive breastfeeding in Saudi Arabia indicate that a greater understanding of the associated factors is required to support and inform the creation of campaigns promoting exclusive breastfeeding in the country, in order that more infants are exclusively breastfed in line with the WHO recommendations. Therefore, this study is important in determining the prevalence of exclusive breastfeeding at 6 months and identifying the factors that may discourage mothers in Tabuk, North West Saudi Arabia, from exclusive breastfeeding at 6 months.
Method
This cross-sectional study was performed in Tabuk, Saudi Arabia, between May and September 2015. Tabuk is the capital of the Tabuk region and the largest city in North Western Saudi Arabia, with a population of 534 893 according to the 2010 census. The Epi Info statistical program was used to calculate the sample size from a total of 12 760 live births registered in Tabuk in 2014, assuming a 50% prevalence of exclusive breastfeeding by mothers when their infants reached 6 months of age, a confidence limit of 5%, and a 95% confidence level. The resulting sample size was 560 infants.
Tabuk’s 21 primary health care centers (PHCCs), each covering approximately equal numbers of the population, provide maternity care and childcare to users primarily from low- and medium-income groups. Five PHCCs, 1 for each region of Tabuk, were selected for the study using random sampling and were each posted a letter from the regional health administrator of Tabuk with a factsheet outlining the objectives of the research and asking for assistance from their health professionals in facilitating questionnaire completion.
Nearly all mothers in Saudi Arabia, especially those with children below 3 years of age, are referred to a PHCC Well-Baby Clinic twice a year or more for various reasons, including for their children to be vaccinated (5 times in the first year of life, once at 18 months and then at 2 and 4 years of age), to receive prenatal care and/or for family planning purposes.
Mothers attending the Well-Baby Clinics at the chosen PHCCs who were literate and had a healthy child aged between 6 and 24 months were eligible to take part in the study. Mothers who met these criteria were approached in person and invited to attend an interview after being given a proper orientation. Those who consented to attend the interview were given an information sheet and asked to sign a consent form confirming their participation. The data for the research were collected during business hours at the clinic so that participants could be interviewed to complete their questionnaire answers without losing their places on the waiting list.
Data collection
In all, 614 mothers were invited to participate in the research, and 589 eligible mothers completed the structured questionnaire while attending Well-Baby Clinics, resulting in a response rate of 95.6%. For assistance, they attended interviews with trained, Arabic-speaking, female nursing staff. Data on 2 main areas were gathered: sociodemographics and breastfeeding habits. The information gathered on the mothers’ sociodemographic circumstances related to their age, education, nationality, employment status in the first 6 months after delivery, whether they cohabited with their husband, their number of children, their method of delivery of their infant, and family income in Saudi riyals. There were 4 income categories: <5000 Saudi riyals constituted a family of low socioeconomic class, 5000 to 10 000 Saudi riyals meant a family in the lower-middle socioeconomic class, 10 001 to 15 000 Saudi riyals meant a family in the upper-middle socioeconomic class, and an income of >15 000 Saudi riyals meant a family in the higher socioeconomic class. The father’s age, education, nationality, and employment status and the age, sex, gestational age, and birth weight of their infants were also gathered. Data on breastfeeding practices specifically related to whether the infant had breastfed; if so, how long exclusive breastfeeding had lasted, the mothers’ knowledge of breastfeeding recommendations, and their reasons for breastfeeding and stopping breastfeeding. When the participant had more than 1 child below 2 years of age, her responses related to her youngest child.
A pilot study with 25 participants was conducted to test the questionnaire design to gather their feedback and make any necessary changes. This study established that the questionnaire required an average of 15 minutes to complete. The participants were removed from the sample for the final study.
Definitions
Preterm delivery is defined in this research as any live infant born at less than 37 weeks’ gestation. Low birth weight is defined as any live infant born weighing less than 2500 g. Information on the infants’ gestational age and birth weight was gathered from the health records of the mothers and infants attending the PHCCs. The outcome variable (exclusive breastfeeding for the first 6 months of life) is defined by the WHO’s recommendation as an infant being fed only human breast milk without any other solids or liquids, including water, with the exceptions of drops and syrups that provide minerals, vitamins, and necessary medications at 6 months of age. 6 This is expressed in terms of the proportion of infants being exclusively breastfed for the first 6 months of life.
Ethical approval
The researcher sought and received ethical approval for this study from the Research Ethics Committee at the University of Tabuk.
Data analysis
All the questionnaire data were allotted suitable codes before analysis using the SPSS program, version 21.0. Initially, univariate logistic analyses of the outcome variable (exclusive breastfeeding at 6 months of age vs mixed or formula feeding) were conducted for each factor. Significant predictors of exclusive breastfeeding from the univariate logistic analysis were then added into a multivariate logistic regression analysis. The odds ratios and their 95% confidence intervals were calculated. P ≤ 0.05 was chosen as an acceptable statistical significance level. This form of assessment was based on the algorithm of Hosmer and Lemeshow, 16 which was also used by Tan. 11
Results
Table 1 displays the sociodemographic information of the participants. It shows that more than half (61.1%) of the 589 eligible mothers were between 25 and 35 years of age, and 52.3% of the participating mothers had received fewer than 12 years of education. Most were from Saudi Arabia (90.2%), and most were not in paid employment (77.6%). In all, 46.3% of the mothers had household incomes of between 5000 and 10 000 Saudi riyals per month. Most of the deliveries had been vaginal (68.8%), and almost all (94.7%) the infants in the study had been born at full term. Finally, 45.7% of the 589 infants in the research were female, and 54.3% were male. Most (86.9%) of the infants were born at normal weight.
Sociodemographic information on the study participants (N = 589).

Non-Saudi: from other Arab countries such as Jordan, Egypt, Syria, and Yemen.
Figure 1 shows that 96.1% of mothers exclusively breastfed their babies in the first 48 hours of life, falling to 82.7% when their infants were 1 month of age, after which there was a rapid decline in exclusive breastfeeding, from 66.0% at 3 months to 31.4% at 6 months.
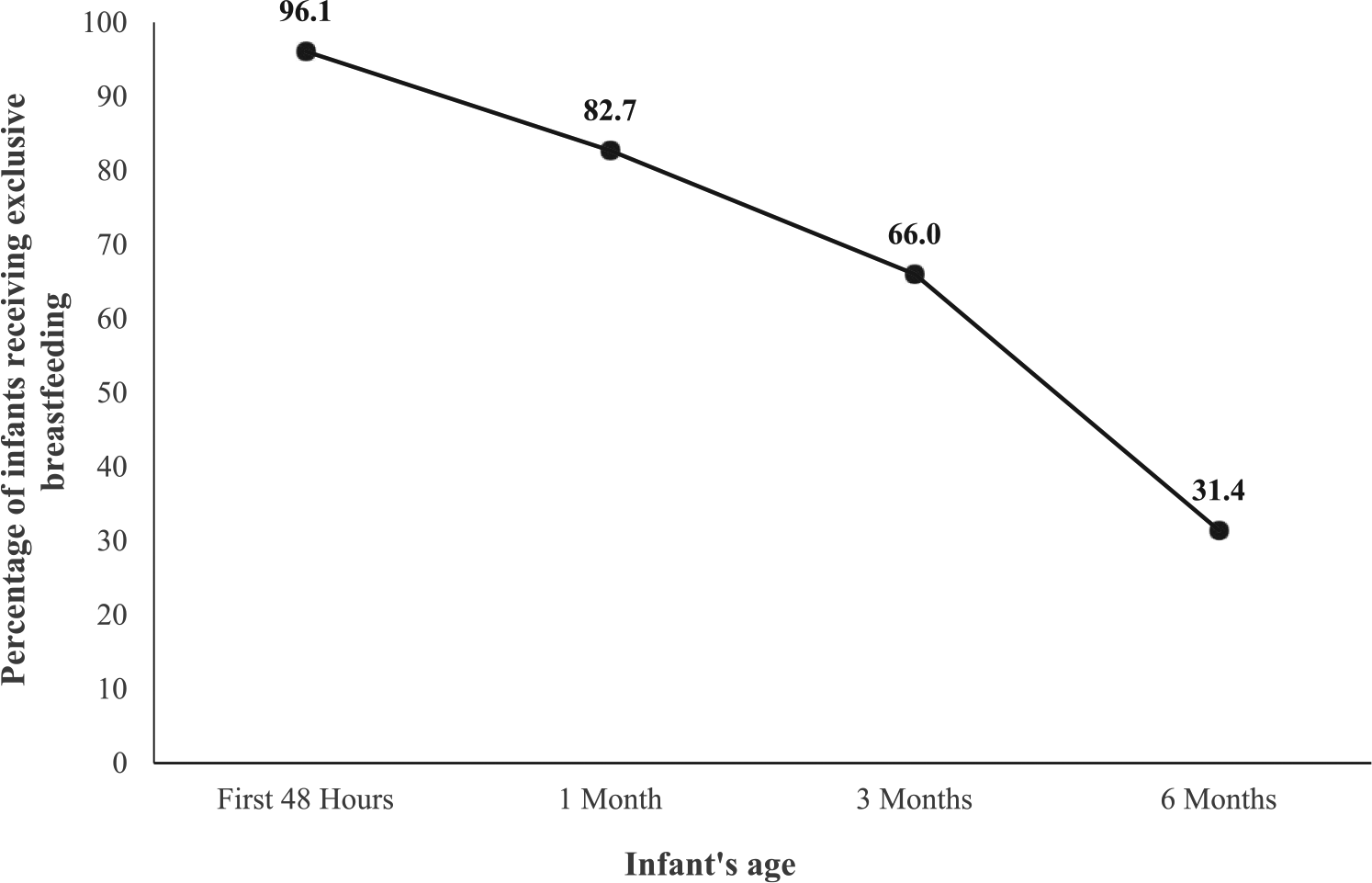
Distribution of rates of exclusive breastfeeding at different ages (N = 589).
Table 2 presents the results of the logistic regression analysis of the sociodemographic participant data and exclusive breastfeeding status at 6 months after delivery. A univariate analysis found that 5 factors had significant associations with exclusive breastfeeding: mother’s nationality, mother’s employment status, mode of delivery, mother’s awareness of the recommendations for exclusive breastfeeding, and infant’s birth weight. These 5 factors were entered into a multivariate model which produced the finding that exclusive breastfeeding at 6 months was less likely to be reported by mothers with Saudi nationality, those in employment, those who had had cesarean deliveries, and those who had given birth to infants with low birth weights. Conversely, a positive association was observed between exclusive breastfeeding and mother’s awareness of the recommendation on the duration of exclusive breastfeeding.
Factors associated with exclusive breastfeeding at 6 months (N = 589).
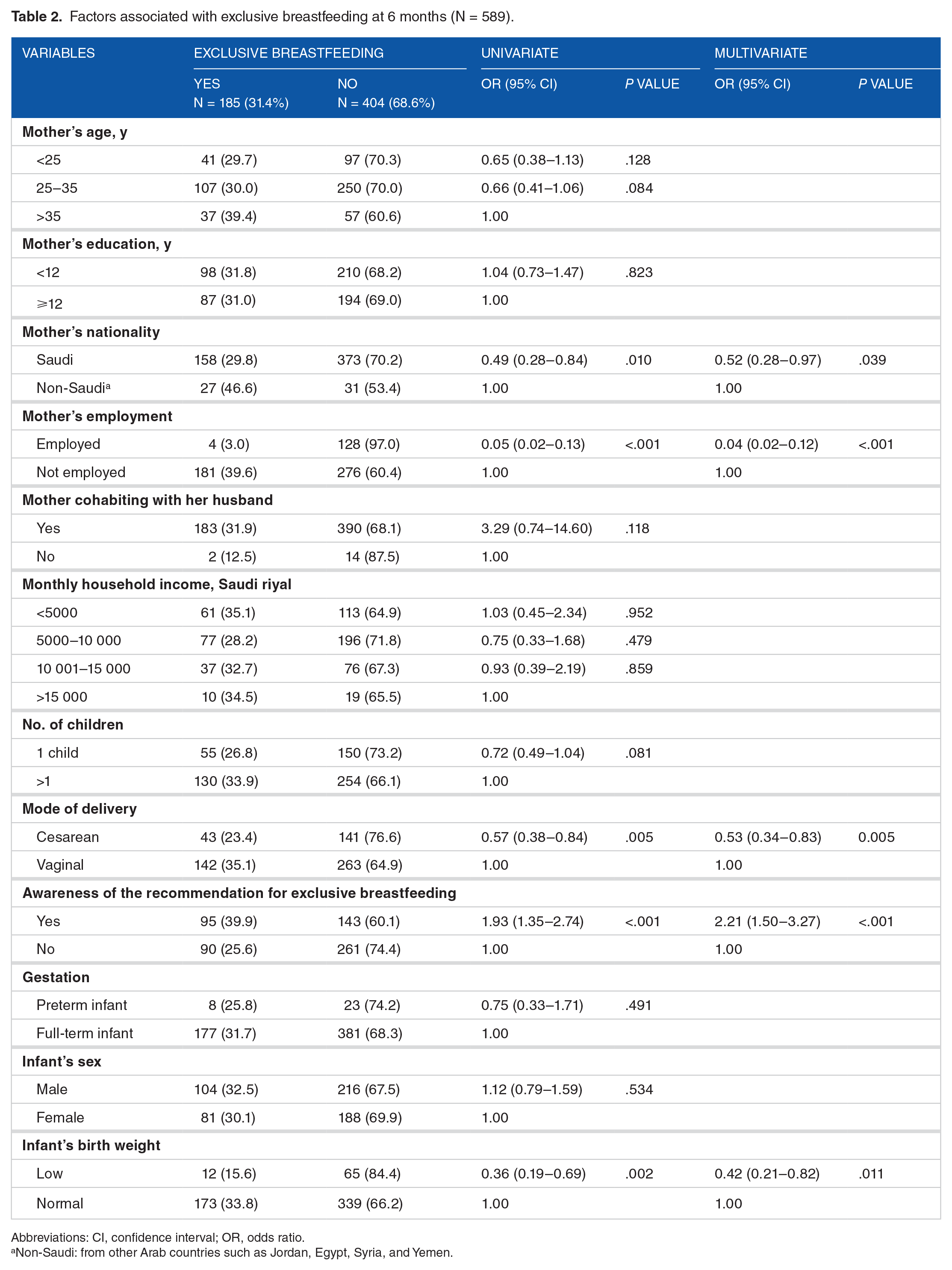
Abbreviations: CI, confidence interval; OR, odds ratio.
Non-Saudi: from other Arab countries such as Jordan, Egypt, Syria, and Yemen.
Discussion
This research study surveyed a total of 589 mothers from urban communities, of whom 31.4% reported having exclusively breastfed their infant for the first 6 months of life. Prior research studies in Saudi Arabia have presented inconsistent findings regarding the prevalence of exclusive breastfeeding of 6-month-old infants, ranging from 1.7% to 24.4%. 14 Similarly, the reported exclusive breastfeeding rates have also varied across different Middle Eastern countries: only 1% of mothers in Jordan were reported to breastfeed exclusively for 6 months (the lowest rate reported in Middle East countries) 17 ; in the United Arab Emirates, 1.9% 18 ; in Egypt, 9.7% 19 ; in Qatar, 18.9% 20 ; in Turkey, 54%; 7 and in Iran, 66.4%. 21 Several factors exert an influence on exclusive breastfeeding. The infant’s place of birth inevitably causes variations in breastfeeding due to the specific local culture and feeding traditions, the parents’ socioeconomic status, their ethnic background and education, and the level of urbanization and modernization of their place of residence. 22
This research identified 5 factors associated with mothers’ exclusive breastfeeding of their infants at 6 months of age. The first of these is that mothers of Saudi Arabian nationality were less likely to breastfeed at 6 months than non-Saudi mothers from other Arab countries living in Saudi Arabia. To the best of this author’s knowledge, no previous studies have explored the differences in breastfeeding practices between mothers of Saudi and non-Saudi nationality because holding Saudi nationality has been used as an eligibility criterion in prior studies in the country, making such a comparison impossible.10,15,23 Some international studies have, however, found that breastfeeding practices vary across different ethnicities.24,25 Taking a Malaysian study as an example, 11 Chinese mothers in Malaysia were found to have a lower likelihood of exclusive breastfeeding than Malaysian mothers. The authors of that study proposed the possible explanation that Chinese mothers living in Malaysia often hire an experienced nurse to care for their infants. A similar reason could also be valid in this study as Saudi women often employ foreign nannies or maids to assist with childcare and feeding, 10 and this could help to explain Saudi mothers’ low rates of exclusive breastfeeding.
In line with prior research in Saudi Arabia,10,15 this study also found that mothers’ employment was negatively associated with breastfeeding, as babies whose mothers worked had a lower likelihood of being exclusively breastfed at 6 months of age than those whose mothers were not in employment. The negative association between employment and exclusive breastfeeding reported in these studies was also found in Lebanon, Iran, and Malaysia.11,26,27 This might be universal simply because mothers who could spend sufficient time with their young infants can more easily exclusively breastfeed them than those lacking time due to working or other reasons. 28 Furthermore, working mothers in Saudi Arabia are only legally entitled to 2 months of maternity leave on full pay, but breastfeeding facilities in working environments are not generally available. It is therefore easy to understand why working mothers are discouraged from exclusive breastfeeding, factors which mothers who stay at home need to consider. Middle Eastern women have generally enjoyed improved education and employment opportunities in recent years, but these heighten the risk of lower rates of exclusive breastfeeding.10,29 For this reason, and the strong association between maternal employment and exclusive breastfeeding, programs providing support and resources in places of work and childcare centers are needed (eg, by supplying breast pumps) to help mothers to continue breastfeeding their infants after maternity leave ends.
In this study, an association was also found between delivery method and exclusive breastfeeding status. Cesarean births were associated with lower rates of exclusive breastfeeding at 6 months. This concurs with previous research in Saudi Arabia15,23 which reported low exclusive breastfeeding rates at 6 months among mothers who had cesarean deliveries. Similarly, a meta-analysis of a total of 53 studies from 33 countries found an association between cesarean births and lower rates of exclusive breastfeeding. 30 Ideally, all hospitals should practice the Ten Steps to Successful Breastfeeding policy recommended by the WHO, 31 which aims to promote the successful initiation and continuation of exclusive breastfeeding and which has been shown to increase breastfeeding rates in time and exclusivity. 32 However, the Ten Steps to Successful Breastfeeding policy has not become a standard practice in Saudi Arabia, with only 28 hospitals of 400 Saudi hospitals adopting it. 33 This could explain why mothers who gave birth by cesarean delivery did not initiate or continue exclusive breastfeeding. 34 Furthermore, prelacteal feed (which is also significantly negatively associated with exclusive breastfeeding) is common in mothers who have had cesarean deliveries. It has been proposed that it may appear natural to them to continue to feed their infant using the food they began with and that they had a plausible reason to do so. 35 This is highly relevant because in this research in Tabuk, Saudi Arabia, 31.2% of births were by cesarean delivery, a higher proportion than has been recorded in other parts of the country.10,15,23,36 Cesarean births have become more common worldwide and are now the most common surgical procedure in the United States, used in 31.8% of all births, whereas in China and some areas in South America, between 40% and 50% of births are reportedly cesarean deliveries. 30 Further research is required to build understanding of the influence of cesarean deliveries on exclusive breastfeeding.
This study further identified that mothers whose infants were born at low birth weight were less likely to exclusively breastfeed them at 6 months of age. To the best of the author’s knowledge, only 1 prior Saudi Arabian study has investigated the association between infant birth weight and exclusive breastfeeding for 6 months, 15 and it concluded that an association existed between low birth weight and a low prevalence of exclusive breastfeeding in the first 6 months of life. Another study by Jones et al 8 found that very low birth weight was positively associated with the likelihood of breastfeeding and also with a lower chance of exclusive breastfeeding in comparison with infants born at normal or above-normal birth weights. Another study found that beliefs exist, especially among mothers without health education, that low birth weight babies require additional foods in addition to breast milk to encourage weight gain and, further, that mothers are unable to produce sufficient breast milk for their needs. These beliefs lead to supplementary foods being introduced too early in an infant’s life. 37 Therefore, mothers should receive reassurance that breast milk on its own is sufficient to meet even a low birth weight infant’s nutritional requirements so that they do not feel they need to supplement breast milk with other foods.
One unexpected finding produced by this research was the positive association between exclusive breastfeeding and the mother’s knowledge of the recommended duration for which exclusive breastfeeding should last. Mothers who reported awareness of the recommended period of 6 months were found to be 2.2 times more likely to breastfeed exclusively than mothers who were unaware of the recommendation. Although this study found a low rate of awareness of the recommended duration of exclusive breastfeeding (40.4%), previous research studies in Saudi Arabia have reported even lower rates.10,38,39 For example, in the first of Al Binali’s 2 studies in Abha (in South West Saudi Arabia) which used a sample of female teachers, only 28% of the mothers reported awareness of the recommended exclusive breastfeeding duration. 38 In the second of Al Binali’s 39 studies, using a sample of female health workers, 37.7% of the mothers were aware of the recommended duration. Similar low levels of awareness, with the associated risks of the introduction of dietary supplements before the age of 6 months and early breastfeeding cessation, have also been discovered by prior studies in developing countries. 10 Overall, these findings underline the importance of raising awareness among new mothers of the recommended time period for which an infant should solely receive breast milk.
As with all research, this study has some limitations which should be taken into consideration when examining its findings. The cross-sectional research design is the most important of these as it prevents the drawing of causal inferences from the associations indicated between influential factors and exclusive breastfeeding practice. Second, this design is also limited by potential recall bias because data on exclusive breastfeeding are dependent on mothers’ recollections about the time since they gave birth, and some women may have difficulty in accurately remembering the points in time at which they introduced complementary liquids or foods into their child’s diet. A third limitation is that the study only accessed mothers attending state-run PHCCs and therefore excluded mothers at other health centers (such as privately run ones) who might fall within other socioeconomic categories and might therefore display different patterns and influences with regard to exclusive breastfeeding. Fourth, this study did not gather data on psychosocial factors, including self-efficacy, self-concept and social support, and hospital practices such as rooming-in, early infant-to-breast contact, demand feeding, and antenatal classes, each of which might also significantly contribute to the maintenance of exclusive breastfeeding and can be included in future research in this field. Finally, this study’s sample only contained mothers attending PHCCs for infant vaccinations in 1 region of Saudi Arabia, so its findings may not be generalizable to the country as a whole.
Conclusions
The prevalence of exclusive breastfeeding of infants at 6 months of age was found to be low among the study sample, offering further support to the results of previous Middle Eastern studies.7,14,17–21 Negative associations were identified among working mothers, mothers with Saudi nationality, babies born via cesarean deliveries, and babies born with low birth weights, but exclusive breastfeeding was found to be positively associated with the mother’s awareness of the recommended duration of exclusive breastfeeding. These high-risk groups should therefore be targeted by programs promoting 6 months of exclusive breastfeeding in line with WHO’s 10 Steps campaign, which needs to be far more widely applied across hospitals in Saudi Arabia than it is at present (only 28 hospitals out of 400 nationwide follow it). The study also found that 2 of the factors identified are modifiable: mothers in employment and mothers’ awareness of the recommended duration of exclusive breastfeeding. Improved workplace breastfeeding facilities are therefore clearly needed (such as providing breast pumps and rooms for feeding), and increased maternal awareness of the recommended duration for exclusive breastfeeding should be strongly targeted in the formulation of new strategies to improve exclusive breastfeeding rates. Furthermore, research on a wider scale is also required to examine the different factors influencing breastfeeding practices.
Footnotes
Peer Review:
Six peer reviewers contributed to the peer review report. Reviewers’ reports totaled 2472 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by research grant from Deanship of Scientific Research (DSR) at the University of Tabuk, Saudi Arabia.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
RAA designed the study, set the study protocol, and carried out the fieldwork. He also performed the data analyses and drafted the manuscript.