
Abstract
Background:
Bone metastases (BMs) are a common complication in patients with cancer, often leading to significant pain that adversely affects quality of life, necessitating effective pain management strategies. This study aims to evaluate the effectiveness of pain management in patients with BMs undergoing palliative radiotherapy and to identify determinants of pain management adequacy.
Methods:
We conducted an observational analysis of 560 patients from the Palliative Radiotherapy and Inflammation Study (PRAIS) trial across several European centers, focusing on the Pain Management Index (PMI) for assessing pain management adequacy. Key predictors examined included Karnofsky Performance Status (KPS), treatment setting, primary tumor type, and site of BMs.
Results:
Our findings indicate that 19.0% of patients experienced inadequate pain management (PMI < 0). Specifically, patients with KPS ⩾ 90 had a notably lower rate of adequate analgesic therapy (59.3%) compared with those with a KPS < 90 (85.0%). Among outpatients, 23.7% reported inadequate pain management, contrasted with a significantly lower inadequacy rate (3.8%) in palliative care or hospice settings. In addition, in outpatients, pain management adequacy varied with the primary tumor type, showing improved outcomes for patients with lung cancer (89.2%) versus other primary tumors (79.1%). Moreover, in non-outpatients, pain management was less effective for patients receiving radiotherapy on pelvic BMs (89.5%) compared with other sites (95.7%).
Conclusion:
Although overall rates of inadequate pain management were lower than seen in previous studies, significant variability exists based on patient health status, care setting, primary tumor type, and site of BMs. These results underscore the need for personalized pain management approaches and highlight specific areas for improvement in outpatient settings and among patients with generally good health but significant pain from BMs.
Keywords
Introduction
Pain, depression, and fatigue are frequently encountered symptoms among patients with cancer, recognized by the National Cancer Institute as critical symptoms that require thorough evaluation. 1 Pain stands out as a prevalent issue for individuals with cancer, arising from the cancer itself, its spread, or the side effects of treatments. It is reported that up to 90% of patients may experience pain of nociceptive or neuropathic nature throughout their cancer journey.2,3
Pain in patients with cancer is a complex condition that significantly deteriorates the quality of life (QoL) due to its physical and psychological repercussions.4-7 Indeed, insufficient pain management is strongly associated with a decline in QoL, as it adversely affects daily functioning, mood, and autonomy.8,9
As such, the management of pain is a high priority within the field of oncology, with guidelines recommending the assessment of pain both before and throughout treatment to ensure effective management.3,10 Despite the existence of these guidelines and various effective pain-relief methods, the treatment of pain remains suboptimal in many cases.11-15
Consequently, numerous studies have been conducted to assess pain management across various cancer care settings.16-29 Nonetheless, there is a scarcity of such research in patients undergoing radiotherapy (RT). 16 -18,20 Our previous work includes 2 analyses from a multicenter observational study aimed at assessing the adequacy of analgesic therapy in RT patients.
In the initial analysis (ARISE 1), 28 we enrolled 2104 outpatients with cancer, all 18 years or older, across 13 RT departments. The intent of RT was either curative (62.4%) or palliative (37.6%), with 57.3% of patients having nonmetastatic and 42.7% having metastatic stages of cancer, respectively. Pain was present in 1417 patients, with 45.0% of them receiving inadequate pain management. Factors such as the intent of RT being curative, an Eastern Cooperative Oncology Group (ECOG) performance status of 1 (vs ECOG 3-4), diagnosis of breast cancer, noncancer-related pain, and the geographic location of the RT center significantly influenced the adequacy of pain management.
In our subsequent analysis (ARISE 2), 29 we focused on the adequacy of pharmacologic pain management in patients assessed prior to RT within the same cohort. This analysis included 1042 cancer outpatients, revealing that 42.9% of those with pain had not been adequately managed. Among those with pain or those using analgesics and undergoing either palliative or curative RT, 72% and 75%, respectively, had inadequate or ineffective analgesic treatments. Odds of receiving adequate pain management were higher among patients slated for palliative RT (odds ratio [OR] = 2.52; P < .001), with an Eastern Cooperative Oncology Group Performance Status (ECOG-PS) 30 scores of 2, 3, and 4 compared with score 1 (OR = 1.63, 2.23, 5.31, respectively; P = .017, .002, .009, respectively), with cancer-related pain (OR = 0.38; P < .001), and for those treated in the northern part of Italy as opposed to the central or southern regions (OR = 0.25, 0.42, respectively; P < .001).
However, these analyses were limited by their focus on Italian patients and by including a diverse patient group referred for both curative and palliative RTs, which hindered a detailed examination of the factors affecting pain management in these distinct settings.
Therefore, we have designed a subanalysis within an international multicenter study (PRAIS) aimed at evaluating the adequacy of pain management among a uniform group of patients undergoing palliative RT specifically for BMs.
Materials and Methods
This investigation is a detailed analysis derived from the PRAIS trial, which is a longitudinal, observational study spread across various European locations (Trondheim, Ålesund, Oslo in Norway; Milan and Meldola in Italy; Lleida in Spain; Hull in the United Kingdom) aiming to gather data on patients undergoing palliative RT for cancer-related bone pain. 31 The study included patients from multiple European centers: St. Olavs Hospital, Trondheim University Hospital in Trondheim, Norway; Oslo University Hospital in Oslo, Norway; Ålesund Hospital, Møre and Romsdal Hospital Trust in Ålesund, Norway; Fondazione Institute of care with a scientific character (IRCCS) Istituto Nazionale dei Tumori in Milan, Italy; Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS in Meldola, Italy; Arnau de Vilanova University Hospital, IRB in Lleida, Spain; and Hull York Medical School, University of Hull in Hull, United Kingdom. The study was conducted over a 4-year period, from December 2013 to December 2017. From the PRAIS trial database, only patients reporting pain or taking analgesics (560) were selected for our analysis. The main goal was to determine the effectiveness of pain management in patients receiving RT. Another objective was to identify any potential relationships between the success of pain management and certain predictors, including demographic and clinical characteristics such as sex, age, KPS, timing of the visit, aim of RT, type and stage of primary cancer, nature of pain, and the geographic location of the RT facility.
Regarding endpoints, the primary focus was on evaluating the success of pain management for BMs in RT departments. The secondary aim was to explore any associations between pain management success and the identified predictors.
In eligibility, all participants of the PRAIS study were considered for our analysis. This encompassed patients with a confirmed cancer diagnosis and radiologically confirmed BMs, who were scheduled for palliative RT targeting painful BMs.
Data for this subanalysis were extracted focusing solely on pretreatment assessments. Information was collected using a standardized form during the initial visit, capturing details on sex, age, KPS, RT objectives, primary cancer type, tumor stage, pain intensity using the Numeric Rating Scale (NRS),32,33 analgesic usage, and the type of pain experienced (classified as cancer pain [CP], noncancer pain [NCP], and mixed pain [MP]). Pain intensity was categorized on a scale from 0 (no pain) to 3 (severe pain), and analgesic usage was scored from 0 (no medication) to 3 (strong opioids), with the Pain Management Index (PMI) 34 calculated by subtracting the pain score from the analgesic score. A negative PMI value indicated inadequate pain management. The administration of adjuvant drugs did not change the pain score classification and, therefore, the PMI calculation.
The study inclusion criteria allowed patients with solid tumors being referred for palliative RT. The consideration for inclusion extended to patients who had received, were receiving, or would receive RT, chemotherapy, hormone therapy, targeted therapies, and immunotherapy, as well as supportive palliative care medications.
For statistical analysis, descriptive statistics summarized continuous variables, whereas categorical variables were reported as counts and percentages. Factors such as sex, age, KPS, timing of the visit, RT intention, primary cancer, disease stage, pain type, analgesic score, and RT center location were examined for their potential association with PMI. The chi-squared test was used to ascertain statistical significance, with a P value of <.05 denoted as significant. These analyses were conducted using the XLSTAT software package.
Variable selection and the development of a predictive model employed the Least Absolute Shrinkage and Selection Operator (LASSO) method and machine learning techniques to identify significant prognostic variables and refine the model for training and validation. The classification and regression tree (CART) analysis, a type of machine learning model, was then applied to distinguish between patients adequately and inadequately treated for pain, based on the significant variables identified. The performance of these models was evaluated through the use of receiver operator characteristic (ROC) curves and the area under the curve (AUC), with a rigorous cross-validation process.
From an ethical standpoint, the study was approved by the Area Vasta Romagna Ethics Committee and adhered to the principles of the 1964 Helsinki Declaration and its subsequent amendments, along with Good Clinical Practice guidelines. Written informed consent was secured from all participants, ensuring that no identifiable human data were included in the manuscript.
Results
Patients and Treatment Characteristics
The study encompassed 560 participants, with an average age of 66 years (SD: ±10.7 years), and a predominance of male participants (61.6%). The majority identified as White, with the leading sites of primary tumors being the prostate (25.6%), breast (19.6%), and lung (18.2%). A significant portion of the cohort, 84.5%, had a KPS score of 80 or above, and 70% were treated on an outpatient basis. Bone metastases were predominantly found in the spine (46%) and pelvis (33%). Treatment regimens varied, with about 37% of patients receiving RT in a single fraction. Opioid analgesics were used by 81% of patients, and 33% received steroids as part of their treatment protocol (Table 1). In addition, anticonvulsants and antidepressants were also used for pain treatment in 12% and 1% of patients, respectively.
Patient characteristics and univariate analysis (560).

The PMI analysis showed that 19.0% of the patients experienced inadequate pain management. Using the LASSO analysis, we were able to identify the factors that contributed to a PMI score below zero, indicating insufficient pain management. In fact, the predictive model included KPS, patient care setting (outpatient vs other), anatomical location of treated BMs, and primary tumor (Figure 1).

Predictive model for adequate pain management: the percentages represent the proportion of patients with adequate pain management (PMI ≥ 0), while the numbers in brackets represent the total number of patients within each group.
Specifically, our findings showed that patients with a KPS ⩾ 90 were significantly less likely to receive adequate analgesic therapy compared to those with a KPS < 90 (59.3% vs 85.0%). Among patients with KPS < 90, those treated as outpatients had a reduced likelihood of receiving adequate pain management when compared to those in alternative care settings (81.1% vs 93.4%). In addition, within the outpatient group, individuals with primary lung cancer were more likely to have adequate analgesic therapy than those with other types of primary tumors (89.2% vs 79.1%). Finally, for nonambulatory patients, those receiving treatment for pelvic sites experienced less adequate pharmacologic pain management compared with patients treated for other sites (89.5% vs 95.7%). These data are visually represented in Figure 1.
The performance of the CART model for the evaluation of pain management is shown in Figure 2. In the training and validations sets, the AUC values were 0.74 (95% confidence interval [CI] = 0.69-0.79) and 0.73 (95% CI = 0.68-0.77), respectively.

Receiver operating characteristic curves and area under the curve for the training and validation sets.
Discussion
In our study, we focused on understanding how well pain is managed in patients with cancer with BMs. This symptom is very important because it greatly affects patients’ QoL. Our research was part of the PRAIS study, which involved patients from several European countries receiving palliative RT for pain caused by BMs. We looked at 560 patients to see how effective pain management was and to find out what factors might affect it. This included looking at patient details like age, sex, KPS, and type of cancer. Our results showed that 19% of these patients did not get adequate pain management. Using the LASSO method, we identified key factors that contributed to whether patients received good pain management or not.
Our main finding indicates a relatively low rate of inadequate pain management (19.0%) when compared to other analyses using the PMI,17,21,23-29 which reported significantly higher rates of inadequacy (26.6%-82.6%). This discrepancy might stem from our study focus on patients with BMs, where similar rates of adequate pain management (25.1%-33.3%) have been observed.16,17,20 This could be due to health care providers paying more attention to patients with metastatic diseases, especially those exhibiting significant symptoms. Supporting this hypothesis, previous studies have highlighted those patients receiving palliative treatments, whether chemotherapy 23 or RT,28,29 often experience better pain management compared with those undergoing curative treatments (Table 2). Interestingly, no significant correlation was recorded between age and PMI, similarly to what was observed in previous studies.16-18,28,29
Comparison with other studies on Pain Management Index evaluated in patients with cancer.
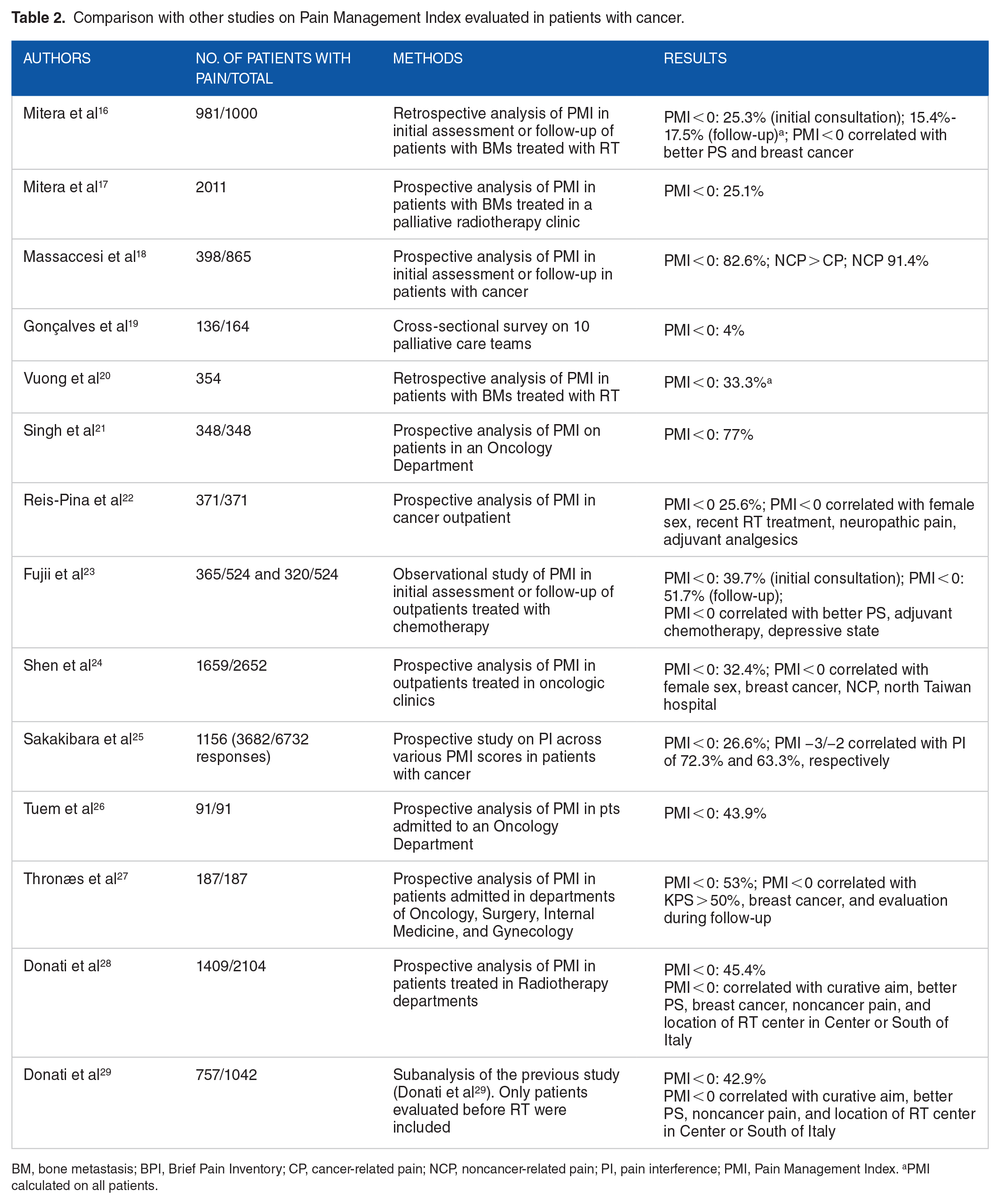
BM, bone metastasis; BPI, Brief Pain Inventory; CP, cancer-related pain; NCP, noncancer-related pain; PI, pain interference; PMI, Pain Management Index. aPMI calculated on all patients.
Our results also underscore the negative impact of a higher KPS on pain management, aligning with earlier findings.23,27- 29 This suggests that patients in better overall health may receive less focus on pain management. Similarly, the observation of suboptimal pain management in outpatient settings corroborates earlier reports, 22 - 24 confirming a trend where patients in relatively good conditions might be overlooked in pain control. On the contrary, we found that pain management was more effective in palliative care or hospice settings (PMI < 0: 3.8%), likely due to both the more severe condition of these patients and the specialized pain management skills of health care providers in these settings. This observation is consistent with a previous study reporting very similar rates of PMI < 0 (4%) among patients under palliative care. 19
Our analysis also revisited the topic of pain management adequacy across different primary cancers, considering historically poorer outcomes in patients with breast cancer,16,24,27,28 while in contrast, our study showed improved outcomes for patients with lung cancer. This might reflect a heightened awareness among doctors toward patients with lung cancer, possibly due to their generally poor prognosis and the presence of additional QoL-compromising symptoms (eg, dyspnea, cough, bleeding, weight loss, and fatigue). Furthermore, although the data available to us do not definitively confirm this, patients with advanced lung cancer may, in some instances, have been treated with opioids to manage symptoms beyond pain, notably dyspnea and cough. This could potentially reduce the number of subjects with a PMI less than 0.
The observation that pain management was less effective for outpatients with pelvic irradiation compared with other sites (PMI ⩾ 0: 89.5% vs 95.7%) is more challenging to explain. It might be that other skeletal areas (eg, spine, limbs, and cranial theca) present more complex symptoms or higher risks of complications, prompting more attentive care from health care providers.
In summary, our analysis highlights the intricate web of factors influencing the effectiveness of pharmacologic pain management in patients with BMs. It underscores the variability in factors affecting PMI across different care settings and emphasizes the need for targeted improvements in pain management, especially for outpatient settings and among patients who, despite experiencing pain, are in otherwise good health.
This study, while offering insights into pain management for patients with cancer undergoing palliative RT, has its limitations. One limitation is that it primarily includes data from a select number of European countries, which might not fully represent the global cancer patient population. In addition, the observational nature of the study means we can identify associations but cannot prove cause-and-effect relationships. However, a major strength of our research is the comprehensive analysis of a large, diverse data set from the PRAIS trial, which allowed us to explore a variety of factors that influence pain management. Another strength is the use of advanced statistical methods to identify these factors accurately. Together, these elements contribute to a deeper understanding of pain management in palliative care, although future studies with broader geographic representation and different study designs are needed to build on these findings.
Therefore, further research in the area of pain management for patients with cancer with BMs is needed to better understand the factors impacting on pain management within this specific population. Prospective studies could focus on longitudinal assessments to track pain management outcomes over time, providing insights into the long-term effectiveness of different therapeutic approaches. Given the complexity of pain in patients with BMs, there is also a significant opportunity to explore personalized pain management plans that incorporate patient-specific factors such as genetic markers, psychological state, and response to previous treatments.
Interdisciplinary studies involving collaboration between oncologists, pain specialists, palliative care teams, and patient advocates are also needed to develop comprehensive care models that address the complex nature of pain in this patient group. In addition, the application of innovative technologies and machine learning to predict pain management needs and outcomes could refine and customize treatment strategies. Research focusing on the efficacy of novel analgesic drugs, nonpharmacologic interventions, patient’s education on pain, and the integration of digital health tools to monitor and manage pain could further enhance care for this specific patient population, ultimately improving their QoL.
Conclusions
Our study highlights the complexity of pain management in patients with cancer with BMs undergoing palliative RT. Despite a relatively low rate of inadequate pain management, significant variability persists based on patient health status, care setting, primary tumor type, and treatment site. These findings underscore the need for targeted improvements, particularly in outpatient settings and for patients with good general health but severe pain. Future research should focus on personalized pain management strategies and explore interdisciplinary approaches to enhance care for this patient population.
Footnotes
Acknowledgements
The authors would like to express their gratitude to all those who helped them during the writing of this manuscript and the European Union horizon 2020 research and innovation program.
Author Contributions
SC, RR, CMD, FM, RH, PK, AGM, and MM involved in conception and design.RH, PK, MDA, VV, and SK involved in research and data collection. RR, CMD, FM, SC, VV, AGM, and MM involved in analysis and interpretation of data. CMD, FM, AGM, and MM wrote the manuscript. All authors involved in approval of final article. AGM and MM contributed equally to this work.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work reported in this publication was funded by the Italian Ministry of Health, RC-2024-2790151 Project.
Consent to Participate
Written informed consent was obtained from the patients for their participation in the study.
Consent for Publication
Informed consent was obtained from those participating to allow scientific publication.
Data Availability
Data supporting reported results can be found at Radiotherapy Unit—A.G. Morganti of the IRCCS Azienda Ospedaliero-Universitaria di Bologna. Prof. Alessio Giuseppe Morganti
Ethical Considerations
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Area Vasta Romagna Ethics Committee (code: L2P1517; May 17, 2017).