
Abstract
Background:
Distant metastasis is the leading cause of death in patients with rectal cancer. This study aims to comprehensively analyze the risk factors of distant metastasis in T3 T4 rectal cancer using magnetic resonance imaging (MRI), pathological features, and serum indicators.
Methods:
The clinicopathological data of 146 cases of T3 T4 rectal cancer after radical resection from January 2015 to March 2023 were retrospectively analyzed. Pre- and postoperative follow-up data of all cases were collected to screen for distant metastatic lesions. Univariate and multivariate Logistic regression methods were used to analyze the relationship between MRI features, pathological results, serum test indexes, and distant metastasis.
Results:
Of the 146 included patients, synchronous or metachronous distance metastasis was confirmed in 43 (29.4%) cases. The patients’ baseline data and univariate analysis showed that mrEMVI, maximum tumor diameter, mr T Stage, pathological N stage, number of lymph node metastasis, cancer nodules, preoperative serum CEA, (Carcinoembryonic antigen) and CA199 were associated with distant metastasis. In the multiple logistic regression model, mrEMVI, pathological N stage, number of lymph node metastasis, maximum tumor diameter, and preoperative serum CEA were identified as independent risk factors for distant metastasis: mrEMVI [odds ratio (OR) = 3.06], pathological N stage (OR = 6.52 for N1 vs N0; OR = 63.47 for N2 vs N0), preoperative serum CEA (OR = 0.27), tumor maximum diameter (OR = 1.03), number of lymph nodes metastasis (OR = 0.62). And, the receiver operating characteristic (ROC) curve was plotted and the area under the curve was calculated (area under the curve [AUC) = 0.817, 95% CI = 0.744-0.890, P < .001].
Conclusions:
mrEMVI, pathological N stage, number of lymph node metastasis, maximum tumor diameter and preoperative serum CEA are the independent risk factors for distant metastasis in T3 T4 rectal cancer. A comprehensive analysis of the risk factors for distant metastasis in rectal cancer can provide a reliable basis for formulating individualized treatment strategies, follow-up plans, and evaluating prognosis.
Introduction
Rectal cancer is one of the most common human malignant tumors. The main treatment for rectal cancer is surgery, supplemented by radiotherapy, chemotherapy, interventional and targeted therapy. In recent years, with the popularization of colonoscopy screening and the optimization of treatment methods, the survival rate of rectal cancer has improved. However, distant metastasis remains a significant problem and is the leading cause of death in rectal cancer patients.
Studies reported that 25% of rectal cancer patients were detected liver metastasis at the time of confirmed diagnosis, and the number increased by 25% during disease progression, totaling about two-thirds of rectal cancer patients who died of liver metastasis. 1 What’s more, compared with total mesorectal excision (TME) alone, preoperative radiochemotherapy does not seem to have improved the survival rate, mainly due to distance metastasis. 2 The survival rate of rectal cancer is also closely related to the time of diagnosis, with the 5-year survival rate being significantly higher for early stage patients compared with advanced stage patients. 3 Some studies have also shown that as tumor infiltration depth increases, the probability of lymph node metastasis and distant metastasis of the tumor also increases significantly, which impacts the difficulty of complete surgical resection and affects the survival rate. 4 Consequently, controlling distant metastases is a major concern in the treatment of advanced rectal cancer. 5
Other adverse prognostic factors including tumor TN stage, high tumor grade, tumor perforation, lymphatic or vascular invasion, and perineural invasion.6-8 Recent studies have shown that EMVI (extramural venous invasion) of rectal cancer is closely related to local recurrence, distant metastasis, poor prognosis, and overall survival.9-12 EMVI is defined as venous involvement beyond the muscularis propria and primarily occurs in T3 T4 stage tumors. EMVI can be intuitively observed by preoperative magnetic resonance imaging (MRI). Therefore, this study retrospectively analyzed the data of 146 cases of T3 T4 rectal cancer, including magnetic resonance (MR) features, pathological results and serum indicators, and comprehensively analyzed the relationship between these factors and distant metastasis, to identify the related risk factors for distant metastasis in rectal cancer, and previous studies in this area have been relatively rarely reported.
Methods
Patients
Between January 2015 and March 2023, 279 rectal cancer patients who were confirmed by colonoscopy and pathology in Yangpu Hospital of Tongji University (Shanghai, China) were included in this study. 146 patients who were pathologically confirmed as having stage T3 T4 rectal cancer and had not received chemotherapy or radiotherapy before surgery were selected (Figure 1). Rectal MRI was performed 1 week before surgery for all patients. Pre- and postoperative follow-up data of the included cases were collected, including abdominal, pelvic, chest computed tomography (CT) scans, and head MRI to screen for distant metastases. All participating patients voluntarily agreed to undergo MRI examination and participated in this retrospective study. All of them provided informed consent.

Flow diagram of patients with rectal cancer.
MRI technique
A whole pelvic scan was performed using a 3T MR (MAGNETOM Skyra, Siemens health care, Erlangen, Germany) with an 18-channel phased array coil. Routine sagittal/axial T2WI and T1WI were as the following parameters:
Sagittal T2WI (TR = 1000 ms, TE = 89 ms, matrix = 320 × 200, FOV = 420 mm × 420 mm).
Axial T2WI (TR = 1600 ms, TE = 96 ms, matrix = 320 × 200, FOV = 380 × 270 mm).
T1WI (TR = 600 ms, TE = 20 ms, matrix = 360 × 270, FOV=320 × 260 mm).
In axial diffusion-weighted imaging (DWI) scan, the diffusion-sensitive factor b was set as 0, 50, and 800 s/mm2 (TR (repetition time) = 5200 ms, TE (echo time) = 67 ms, thickness = 3 mm, matrix = 112×140, FOV (field of view) = 230 × 230 mm).
Enhanced sequences, scanning in 3 directions of axial, coronal and sagittal T1WI, 3D_vibe sequence were used by injecting the contrast medium GD-DTPA (gadolinium-DTPA).
Image analysis
All MR images were retrospectively assessed by 2 blinded senior radiologists. The distance from the lower margin of the tumor to the anus is used as the criterion for determining the position of tumor: <5 cm was defined as the lower segment, 5-10 cm as the middle segment, and >10 cm as the upper segment. The relationship between tumor and peritoneal reflection (PR) was classified into 2 groups: PR involvement group and non-PR involvement group (including no involvement above PR; no involvement below PR, and no trans-PR involvement). The maximum diameter of the tumor was measured through the central level of the tumor. TNM staging was according to the UICC-TNM criteria (Figure 2A to D). Circumferential resection margin (CRM) was considered positive if the shortest distance from the tumor tissue to the adjacent mesorectal fascia was less than 1 cm on the MRI image, and vise versa. EMVI refers to the existence of cancer cell/tissue in the vein outside the muscularis of rectum wall. In the MRI image, EMVI shows that the tumor signal intensity in the extraluminal vessel of the primary tumor is medium, a mass tumor signal shadow, the angiographic morphology with a thickened, tortuous, and irregular edge (Figure 3A to D).

Male, age 50-60, rectal cancer, metastasis to the left intrailiac paravascular lymph node. An enlarged lymph node, 9 mm × 8 mm in size, adjacent to the left internal iliac vessels, A (T1WI C+): heterogeneous enhancement after enhancement. B (DWI, b = 800): the lymph node showed obvious high signal intensity. C: Enlarged lymph nodes seen during the operation. D: Pathologically confirmed lymph node metastasis.

Male, age 60-70, rectal cancer, MRI-detected EMVI: On the T2WI (A), T1WI C+ (B, C), a moderate tumor signal intensity in the extraluminal vessel of the primary tumor. Histology of extramural vascular invasion, 200× (D). MRI indicates magnetic resonance imaging; EMVI, extramural venous invasion.
Pathological judgment criteria
Rectal cancer pathological staging was according to the seventh edition of the American Joint Committee on Cancer (AJCC) TNM staging system. In addition, classic immunohistochemical tests, using a murine anti-human EGFR monoclonal antibody, (Beijing Zhongshan JinQiao Biotechnology Co., Ltd), were performed. Positive EGFR staining shows brownish-yellow or pale-yellow cell membranes and cytoplasm. Not colored as negative (−). The number of color-positive cells > 10% positive, in which weak coloring intensity is weakly positive (+) and moderate coloring intensity is positive (++).
Serum indicators
Preoperative serum indicators, including CEA, CA199, CA125, white blood cells (WBC), red blood cells (RBC), hemoglobin (Hb), platelets (PLT), neutrophils, lymphocytes, monocytes, C-reactive protein (CRP), and other indicators were obtained through the hospital’s medical record report query system.
Statistical analysis
The baseline characteristics of the patients were presented as numbers and percentages, continuous variables with normal distributions are presented as mean ± SD, and variables that were not normally distributed are presented as medians and interquartile ranges (IQRs). Continuous variables were compared using Student’s t test or the Mann-Whitney U test, and proportions of categorical variables were compared using the Pearson’s χ2 test or Fisher’s exact test. Associations between risk factors and distant metastasis in T3 T4 rectal cancer were assessed via logistic regression analyses. Variables with statistical differences in univariate analysis results were included in the binary logistic regression model and entered into the model by the “Enter” method. Univariate logistic regression was used to evaluate the crude odds ratio (OR) and 95% confidence interval (CI). Multiple logistic regression was used to adjust for potential confounders to obtain the adjusted OR and 95% CI. 13 The ROC curve was plotted and the area under the curve was calculated. All statistical analyses were performed using R software (R version 4.1.2) and SPSS (Version 20.0; IBM Statistics, Armonk, NY). All tests were 2-sided and P value < .05 was considered as significant.
Results
Patients
Of the 146 rectal cancer patients included in this study, 104 were men and 42 were women who ranged in age from 33 to 94 years with a mean of 65.7 years. 43 patients (29.4%) were confirmed as having distant metastasis, including 20 patients who were confirmed at the time of the initial diagnosis, 8 patients who were found to have recently occurring liver metastasis within 6 months after surgery, 6 patients who was found to have metastases within 12 months after surgery, and 9 patients who were found to have distal metastasis (including 1 sacral metastases) after 12 months. Liver metastasis was the most common form of metastasis, occurring in 25 cases (58.1%), followed by lung metastasis (9 cases, 20.9%), 5 cases of liver and lung metastasis, 3 cases of liver and peritoneal metastasis, 1 case of sacral metastasis. Of the 43 cases of distant metastasis, 9 cases were confirmed by postoperative pathology, and the remaining 34 cases were confirmed by radiological follow-up (Table 1).
Basic demographic information of the patients.

Abbreviations: CRP, C-reactive protein; IQR, Interquartile range; RBC, red blood cells; WBC, white blood cells; Hb, hemoglobin; PLT, platelets; ADC, Apparent diffusion coefficient; CA, Carbohydrate antigen; CEA, Carcinoembryonic antigen; EGFR, Epidermal growth factor receptor; TBIL, Total bilirubin.
Patient characteristics of the study population stratified by the distant metastasis
The patients’ baseline data and univariate analysis results showed that mrEMVI, maximum tumor diameter, mr T Stage, pathological N stage, number of lymph node metastasis, cancer nodules, preoperative serum CEA and CA199 were associated with distant metastasis (P < .05). There were no significant differences in gender, age, tumor ADC value, CRM, peritoneal reflection, tumor location, morphology, grade of differentiation, lymphovascular invasion, neural invasion, EGFR expression, and serum indicators (CA125, leukocytes, erythrocytes, Hb, PLTs, neutrophils, lymphocytes, monocytes, and CRP) between the distant metastasis group and the nondistant metastatic group (Table 2).
Univariate analysis results of the metastasis and the no metastasis.

Abbreviations: CRP, C-reactive protein; IQR, Interquartile range; RBC, red blood cells; WBC, white blood cells; Hb, hemoglobin; PLT, platelets; ADC, Apparent diffusion coefficient; CA, Carbohydrate antigen; CEA, Carcinoembryonic antigen; EGFR, Epidermal growth factor receptor; TBIL, Total bilirubin.
Multivariate analysis of risk factors for distant metastasis
Multiple logistic regression analysis showed that mr T Stage, cancer nodules and preoperative serum CA199 were not related to distant metastasis in rectal cancer (P > 0.05). mrEMVI, pathological N stage, number of lymph node metastasis, maximum tumor diameter, and preoperative serum CEA were the independent risk factors for distant metastasis (P < .05): mrEMVI (OR = 3.06), pathological N stage (OR = 6.52 for N1 vs N0; OR = 63.47 for N2 vs N0), preoperative serum CEA (OR = 0.27), tumor maximum diameter (OR = 1.03), number of lymph nodes metastasis (OR = 0.62). The risk of distant metastasis in mrEMVI-positive patients with T3 T4 rectal cancer was 3.06 times that of negative patients (P = .039, 95% CI = 1.045-8.945). Compared with pathological N0, the risk of distant metastasis in pathological N1 was 6.524 times (P = .016, 95% CI = 1.41-30.191), and the risk of distant metastasis in pathological N2 was 63.474 times (P = .005, 95% CI = 2.866-1405.6). The risk of distant metastasis in patients with elevated preoperative serum CEA was 0.27 times that of normal patients (P = .024, 95% CI = 0.082-0.865). The risk of distant metastasis increases 1.03 times with every 1 mm increase in tumor maximum diameter (P = .04, 95% CI = 1.001-1.063). The risk of distant metastasis increases 0.623 times with an increase in the number of lymph nodes metastasis (P = .027, 95% CI = 0.405-0.957) (Table 3). Forest plot of the multivariable regression analysis was displayed in Figure 4. According to the multivariable logistic regression model, the probability of predicted value for distant metastasis in 146 colorectal cancer patients was obtained. The ROC curve was plotted and the area under the curve was calculated (AUC = 0.817, 95% CI = 0.744-0.890, P < .001) (Figure 5).
Multivariate analysis of the mrEMVI between the metastasis and the no metastasis.

Abbreviations: CI, confidence interval; OR, odds ratio; EMVI, Extramural venous invasion; CA, Carbohydrate antigen; CEA, Carcinoembryonic antigen.
P < 0.05.
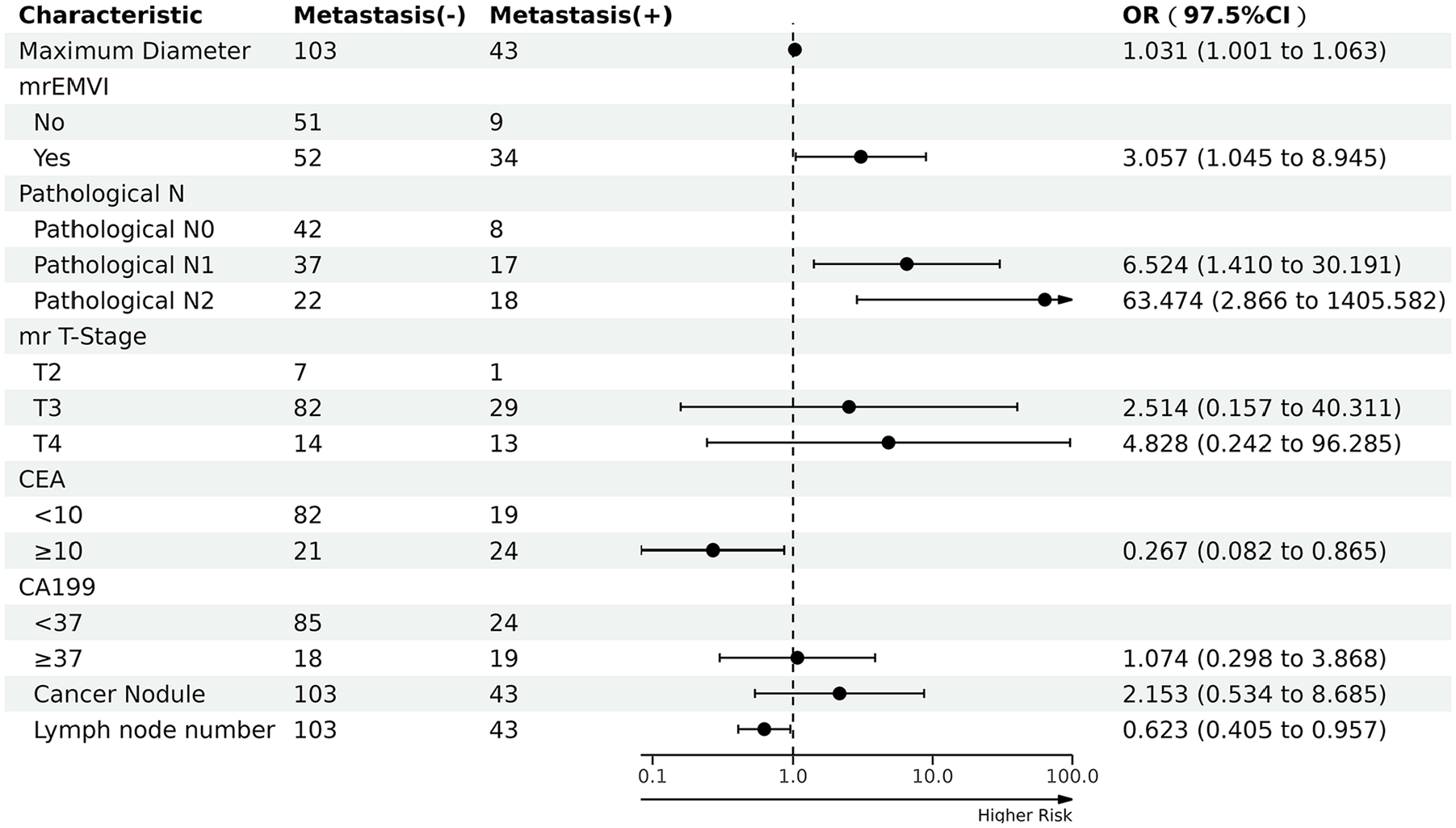
Forest plot of the multivariable regression analysis.

ROC curves of the multivariable regression analysis. ROC indicates receiver operating characteristic.
Discussion
The occurrence, development, and metastasis of rectal cancer are affected by many factors. Risk factors may include tumor diameter, gross type, grade of differentiation, depth of invasion, and lymph node status. Even if patients with rectal cancer cooperate to complete standard treatment actively, there is still a high recurrence and metastasis rate, which increases the risk of death. 14 It has been reported that nearly half of patients with liver metastases from colorectal cancer lose the opportunity for surgery. For these patients, palliative care was the only option, and the 5-year overall survival rate was less than 10%. 15 Therefore, the effective identification of high-risk patients with distant metastasis is crucial for improving the prognosis in rectal cancer.
In this study, a retrospective analysis was conducted on 146 patients with T3 T4 rectal cancer, including their clinical, imaging, pathological data and blood test indexes. Through multiple regression analysis, the study identified mrEMVI, pathological N stage, number of lymph node metastasis, maximum tumor diameter, and preoperative serum CEA were independent risk factors for distant metastasis in patients.
mrEMVI
Among various examination methods, MRI is the only imaging means that can make a non-invasive comprehensive assessment on rectal cancer. Magnetic resonance imaging can be used not only for preoperative identification of EMVI (mrEMVI), but also for the simultaneous detection of local adverse prognostic factors in rectal cancer, with the advantages of high accuracy and reproducibility.16-19 Our study showed that mrEMVI is an independent risk factor for distant metastasis of rectal cancer, which is consistent with previous findings. Sohn et al 20 found that mrEMVI was a risk factor for distant metastasis of rectal cancer, and patients with mrEMVI-positive before treatment had a significantly higher risk of distant metastasis. Tripathi et al 21 found that mrEMVI-positive was an independent risk factor for synchronous distant metastasis of rectal cancer. In a recent meta-analysis, mrEMVI-positive patients had a five-fold increased incidence of synchronous metastases and an approximately 4-fold increased risk of postoperative metachronous metastases. Bugg et al 19 found that mrEMVI-positive can be used as an independent risk factor for simultaneous liver metastasis. Moreover, studies have also shown that microvascular (MVI) and lymphovascular (LVI) are independent predictors of distant metastasis in the early stage (within 1 year after diagnosis) of T3 rectal cancer. Magnetic resonance imaging can detect EMVI preoperatively based on the identification of vasodilation or tumor signals in the venous lumen. The ability of MRI to identify EMVI is comparable with that of conventional histopathological analysis. 16 Brown et al 22 reported 85% concordance between mrEMVI and pathological EMVI. The clinical emphasized on the documentation of vascular invasion in routine pathological examination of cancer specimens and the use of EMVI as an independent predictor of poor prognosis, increased risk of liver metastases, and decreased cancer survival in colorectal cancer.23,24 It is now generally accepted that peritumoral venous invasion is the reason for hematogenous dissemination of tumor cells, which further leads to distant metastasis via portal circulation. 25 Tomisaki et al 24 believed that the occurrence of metastasis in colorectal cancer was related to tumor angiogenesis. Many blood vessels will increase the chances of tumor cells entering the rectal canceration, especially when the subserosal vessels are invaded. Therefore, metastasis is associated with the level of invasion of the intestinal wall. 26 In addition, EMVI is also one of the indications for adjuvant chemotherapy. 6 The detection of EMVI before any surgical procedure can have a decisive impact on the planning of neoadjuvant chemoradiotherapy and adjuvant chemotherapy.
Pathological N stage
Lymph node metastasis is the most common way of rectal cancer metastasis, and lymph node metastasis is related to distant metastasis. Tumor cell growth in the body increases the lymphatic pressure, and those closed lymphatic capillaries under normal conditions will open with the pressure increasing. 27 Tumor cells spread to regional lymph nodes through the lymphatic system and continue to proliferate, which causes lymph node metastasis. Moreover, tumor cells infiltrate into the lymphatic system and invade the vascular system, so lymph node involvement is more prone to hematogenous metastasis. The results of this study showed that lymph node metastasis and the number of lymph node metastasis in T3 T4 rectal cancer were risk factors for distant metastasis, which was consistent with the results of previous studies.28-30 Studies had shown that lymph node metastasis was associated with distant metastasis after colorectal cancer surgery,28,29 and N stage was associated with the presence of synchronous distant metastasis in rectal cancer.21,30 The assessment of lymph node metastasis mainly includes 2 aspects, the number and the location of lymph node metastases. It had been established that lymph node metastasis was an important independent prognostic factor for rectal cancer. 31 It had also been suggested that the number of lymph nodes retrieved during surgery was closely related to the survival and recurrence of rectal cancer. 32 Our study focused on surgical removal of both regional and lateral lymph nodes. In addition, this study also found that patients with N2 stage had more potential for distant metastasis, which may cause more attention to patients with N2 stage.
CEA
CEA is an adhesion molecule of tumor cells and has important value in the diagnosis of colorectal cancer. 33 This study found that preoperative serum CEA level was a risk factor for distant metastasis of T3 T4 rectal cancer, which was consistent with previous studies. Many studies have shown that CEA levels (CEA ⩾ 5 ng/mL) are associated with synchronous or metachronous distant metastasis in rectal cancer.21,30,34 The study of Restivo et al 35 showed that patients of advanced rectal cancer with high CEA levels had a higher risk of early distant metastasis. Wang et al 36 showed that high levels of CEA (> 10 ng/dL) may be associated with early metastases within 6 months after rectal cancer resection in patients treated with preoperative 30 Gy RT. Therefore, preoperative serum CEA level is important in monitoring the recurrence and metastasis of rectal cancer. The serum CEA test is a simple, convenient and economical monitoring method, and it is also easy for patients to accept. In clinical practice, if serum CEA level is increased, further imaging examination should be performed to determine whether distant metastasis occurs. For patients without distant metastasis, the follow-up and monitoring of CEA should also be strengthened, which is helpful for timely detection of metastases and early intervention.
Maximum tumor diameter
The results of this study also showed that tumor diameter maxima was an independent risk factor for distant metastasis. The larger the tumor diameter in rectal cancer patients, the higher the risk of metastasis, consistent with previous studies. The study of Luo 37 et al suggested that tumor size was nearly positively correlated with distant metastasis. The study of Cai et al 38 also showed that tumor size was an independent prognostic factor in patients with stage I to stage III rectal cancer. However, studies had also shown that tumor size had no prognostic effect on colorectal cancer patients. 39 It was even said that patients with stage II colorectal cancer had smaller tumors and a poor prognosis. 40 Therefore, the effect of tumor size on the prognosis of rectal cancer needs to be further studied.
In this study, 8 indicators were found to be related to distant metastasis through univariate analysis, and the differences were statistically significant. Then, the multivariate regression analysis model was further applied to exclude confounding factors, and finally 5 indicators were found to be statistically different. The research methods of previous literature, including case enrollment, 21 inclusion analysis and other indicators 20,28,30 were different from this study. Tripathi et al’s 21 study was based on postoperative patients with T3 rectal cancer that had not been confirmed by histopathology; Dhar DK’s research focused on lymph node staging 28 ; Sohn et al’s 20 study used pathological lymphovascular infiltration (LVI) as the gold standard to calculate diagnostic performance; Gaitanidis et al’ 30 study also included CEA levels. The indicators included in this study were more comprehensive, including pathologically validated T3 T4 stage patients, comprehensive clinical features and serological test indicators. Multivariate logistic regression analysis was used to further explore the independent risk factors associated with distant metastasis. Therefore, we have reason to believe that there is more confidence in the results of the findings.
Limitations
This retrospective study had some limitations. First, the study only included T3 T4 rectal cancer patients, which may limit the generalizability of the findings to patients with other stages of rectal cancer. Second, the sample size of this study was relatively small, which may introduce selection basis. In addition, the follow-up duration in this study may not long enough to capture all instances of distant metastasis.
To address these limitations, future research should consider including a larger and more diverse patient population with longer follow-up periods to improve the reliability and generalizability of the results.
Conclusions
MrEMVI, pathological N stage, number of lymph node metastasis, maximum tumor diameter, and preoperative serum CEA are independent risk factors for distant metastasis in T3 T4 rectal cancer. This comprehensive analysis of risk factors is valuable as it provides important insights for formulating individualized treatment strategies, developing appropriate follow-up plans, and evaluating the prognosis of rectal cancer patients.
Footnotes
Acknowledgements
None.
Author Contributions
Conceptualization: CT; Data curation: CT; Formal analysis: MBL; Funding acquisition: JMX Investigation: SXQ; Methodology: CT; Project administration: CT; Resources: XMZ; Software: HW; Supervision: PJW; Validation: JMX; Visualization: JMX; Writing—original draft: CT; Writing—review & editing: PJW. All authors contributed to the drafting of the article and final approval of the submitted version.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Consent for Publication
All data published here are under the consent for publication. Written informed consent was obtained from all individual participants included in the study.
Ethics Approval and Consent to Participate
The study was carried out in accordance with the Helsinki Declaration. This study was approved by the Ethics Committee of Yangpu Hospital of Tongji University (No. LL-2023-SCI-012). All participating patients voluntarily agreed to undergo MRI examination and provide informed consent.