
Abstract
Introduction:
Although signet ring cell carcinoma (SRC) is a subtype of poorly cohesive carcinoma (PC), the differences in the biological behavior between the 2 morphologically similar carcinomas have not been fully studied. Therefore, we performed transcriptome analysis to evaluate the differences of genetic expressions between SRC and PC.
Methods:
The study group consisted of patients with SRC or PC pathology from patients with early gastric cancer (EGC) whose depth of invasion was localized in the mucosal layer. A total of 18 patients were enrolled. The patients were divided into 3 groups based on their histologic type and lymph node (LN) status. Group 1 consisted of patients with PC and positive LN metastasis, Group 2 consisted of patients with PC without LN metastasis, and Group 3 consisted of patients with SRC without LN metastasis. Transcriptome analysis was performed using the nCounter PanCancer Progression Panel Kit.
Results:
The expression of 77 genes in Group 1 was altered compared to that in normal tissues. The expression of 49 and 13 genes in Groups 2 and 3, respectively, was altered when compared to that in normal tissues. Groups 1 and 2 showed similar genetic expressions. However, Group 3 showed numerous differences in gene expression including Roundabout4 (Robo4) compared to the other groups, especially Group 1.
Conclusion:
Our data suggest that gene expression patterns were different between SRC and PC and expression of ROBO4 may play an important role in the prognosis of SRC and PC type of EGC.
Introduction
Poorly cohesive carcinoma (PC) is a subtype of gastric cancer composed of isolated or small groups of tumor cells. In 2010, the world health organization (WHO) classified a series of carcinomas with decreased cell-to-cell adhesion as PC (including signet ring cell carcinoma [SRC]). 1 Signet ring cell carcinoma consists of tumor cells with prominent cytoplasmic mucin and a crescent-shaped eccentrically located nucleus. 2 Poorly cohesive non-SRCs morphologically resemble histiocytes, lymphocytes, and plasma cells. 3 Signet ring cell carcinomas and poorly cohesive non-SRCs were grouped together in the PC category as they share the property of decreased cell-to-cell adhesion (Figure 1). However, the biological behavior and clinical prognosis of PC and SRC are quite different. Lymph node (LN) metastasis is more common in PC, and the histologic purity of SRC is a good prognostic factor for LN metastasis.4,5 In addition, the depth of the invasion is more marked in PC than in SRC.4,6 Owing to these differences, efforts have been made to distinguish between SRC and PC. A recently published consensus guideline proposed a criterion for differentiating SRC and PC. 7 However, very few studies have investigated why these 2 morphologically similar carcinomas exhibit different biological behaviors. One conceivable study approach is to investigate the differences in gene expression between them. Analysis of the genetic differences that contribute to the differences in the biological behaviors of the 2 carcinomas will help identify genes that can be used as biomarkers to aid treatment decisions for early gastric cancer (EGC).
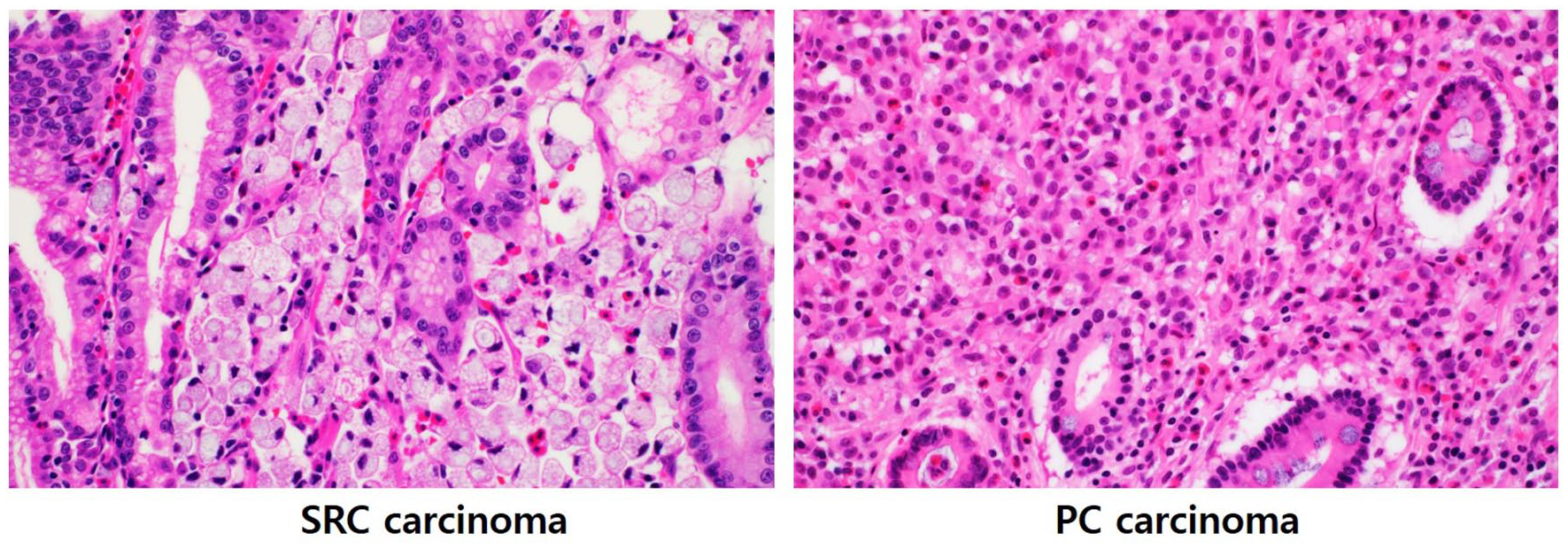
Signet ring cell (SRC) carcinoma and poorly cohesive (PC) carcinoma. Although there are morphological similarities between the 2 carcinomas, their biological characteristics are different (×400, hematoxylin and eosin stain).
The main treatment options for EGC include endoscopic or surgical resection depending on LN metastasis, depth of invasion, and degree of differentiation. Several recent studies on endoscopic submucosal dissection (ESD) in undifferentiated EGCs, including SRC and PC, have reported favorable treatment results.8 -11 We sought to study the differences in the biological behaviors of SRC and PC to identify a biomarker that may help to determine the optimal treatment strategy between surgical and endoscopic resection for undifferentiated cancers. Therefore, we limited the target patients in the study to those with mucosal cancer and performed transcriptome analysis to evaluate the differences of genetic expressions between SRC and PC in EGC.
Materials and Methods
Study population
We selected patients with SRC or PC pathology among patients with EGC whose depth of invasion was localized to the mucosal layer. The study recruitment was conducted on patients who underwent surgery at a university hospital located in Daejeon, Republic of Korea from 2013 to 2018. Differentiation between SRC and PC was based on a recently published guideline. 7 Eighteen patients with EGC who had undergone surgical resection were enrolled in the study. Six patients were assigned to each group. The patients were divided into 3 groups based on their histologic type and LN status as follows: Group 1, patients with PC and positive LN metastasis; Group 2, PC without LN metastasis; and Group 3, patients with SRC without LN metastasis. Normal tissues adjacent to the cancer tissues were also sampled and used as controls.
Transcriptome analysis
Transcriptome analysis was performed using the nCounter Pancancer Progression Panel Kit (NanoString Technology Inc., Seattle, WA, USA), which includes 770 genes involved in angiogenesis, epithelial-mesenchymal transformation, metastasis, tumor growth, and tumor invasion. The nCounter Analysis System (NanoString Technology Inc.) is based on a novel digital color-coded barcode technology that allows for direct multiplexed measurement of gene expression with a small amount of mRNA (25-300 ng) without the need for amplification. 12 RNA was isolated from cancer tissues that were stored as formalin-fixed paraffin-embedded samples in our institution using the Qiagen RNeasy Kit (Qiagen), according to the manufacturer’s instructions. Hybridization was performed by attaching reporter and capture probes to specific genes in the extracted mRNA. The hybridized RNAs were transferred to the nCounter Prep Station (NanoString Technology Inc.) and fixed on a cartridge. This cartridge was then analyzed using the nCounter Digital Analyzer, NCT-DIGT-120 (NanoString Technology Inc.). Following counting, quality control was performed on the reporter code count data using the nSolver program (NanoString Technology Inc.). The raw data were then normalized and changes in gene expression were expressed as fold change. Normalization (standardization) is an essential step that aligns the data to be analyzed to a level that can be compared with each other and is a preprocessing step performed prior to analysis. Normalization is performed to avoid introduction of bias from excessive signal from a specific gene. Normalization was performed using the positive control and housekeeping gene, and the resulting normalized data were used to express the change in gene expression as fold change. All procedures were performed according to the manufacturer’s instructions. Paired comparison between normal and cancer tissues was performed for each patient. Comparative analysis of RNA expression in cancer tissues between groups was also performed.
Statistical analysis
The fold change in the expression of each gene following normalization was compared. A paired t-test was used to compare the differences in gene expression. Differences in the level of gene expression were compared between normal and cancer tissues in each group and also between groups. nSolver performs a 2-tailed t-test on log-transformed normalized data that assumes unequal variance. The distribution of the t-statistic was calculated using the Welch-Satterthwaite equation for the degrees of freedom with an estimation of 95% confidence limits for observed differential expression between groups.
Ethics statement
All procedures complied with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and its later versions. The study protocol was approved by the Institutional Review Board of Chungnam National University Hospital (2020-05-007).
Results
The study consisted of 18 patients with EGC. Six patients were assigned to each group. Eight patients were male and 10 patients were female. Mean age was 50.6 years old, and mean size of the EGC lesions were 3.0 cm (Table 1). Most common site of the lesions were body (10/18, 55.6%). Transcriptome analysis of 770 genes from 18 patients was performed using the nCounter Pancancer Progression Panel Kit (NanoString Technology Inc., Seattle, WA, USA) (Figure 2). In Group 1, 77 genes were differently expressed in cancer tissues compared to that in normal tissues. Seventy-four genetic expressions were increased, and 3 genetic expressions were decreased (Table 2). The expression of 49 and 13 genes in Groups 2 and 3, respectively, was different in cancer tissues compared to that in normal tissues (Tables 3 and 4). In Groups 2 and 3, the expression of 48 and 13 genes, respectively, was increased in cancer compared to normal tissue. The expression of VAV3 gene was decreased in Group 2 cancer tissue compared to the normal control. As a result of comparing changes in gene expression in between normal and cancer tissues by group, it was found that the changes were similar in Groups 1 and 2 but different in Group 3 (Figure 1). There was no significant difference in gene expression between normal tissues of each group, and only a few genes were expressed differently (Table 5).
Demographics of patients.
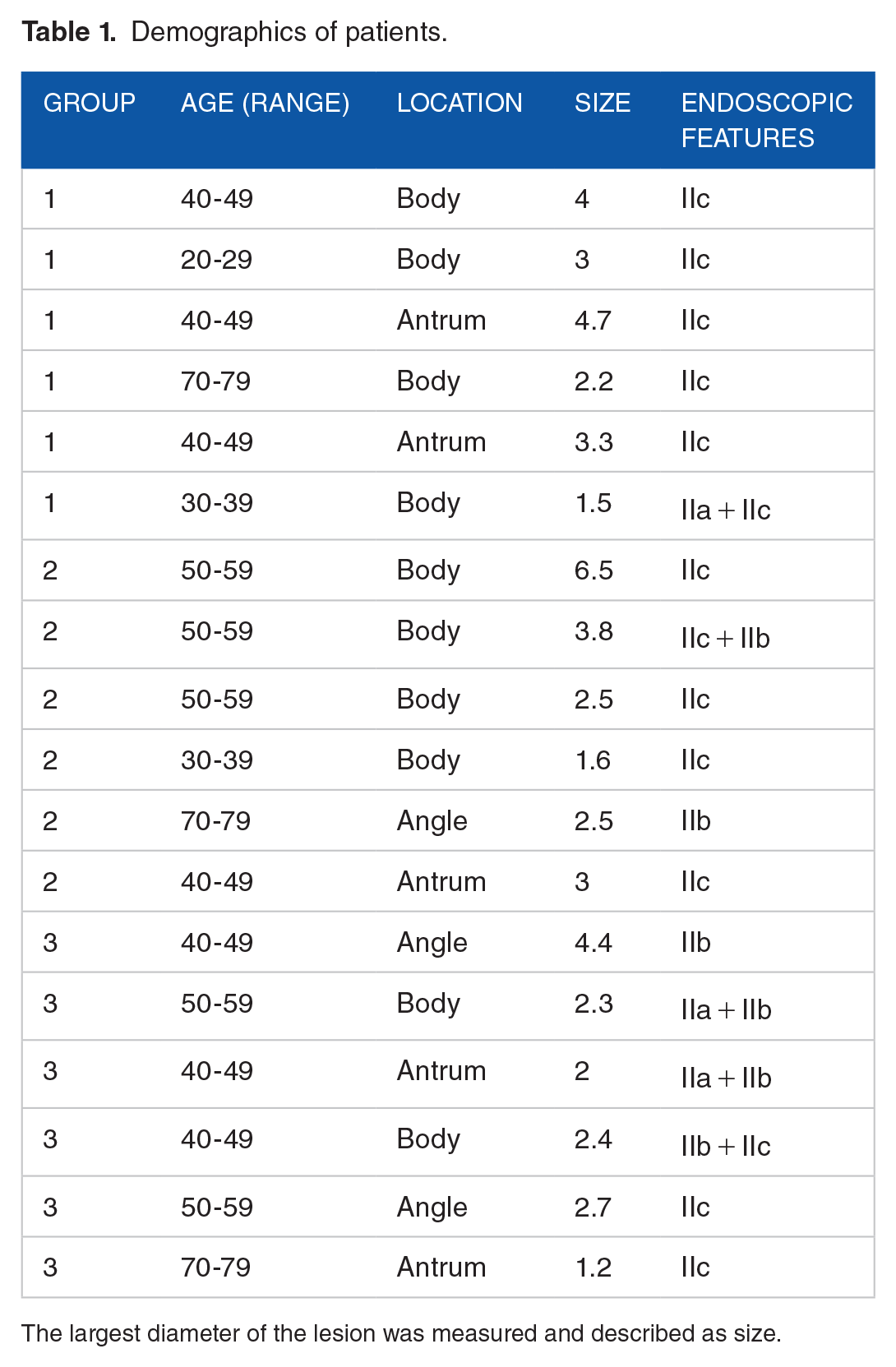
The largest diameter of the lesion was measured and described as size.
Genetic profile of group 1 comparing cancer tissues and normal controls. Gene expression levels indicated by fold changes after normalization were compared.

A 2-tailed t-test.
Genetic profile of Group 2 comparing cancer tissues and normal controls. Gene expression levels indicated by fold changes after normalization were compared.

A 2-tailed t-test.
Genetic profile of Group 3 comparing cancer tissues and normal controls. Gene expression levels indicated by fold changes after normalization were compared.

A 2-tailed t-test.
Comparison of gene expression in normal tissues of each group.
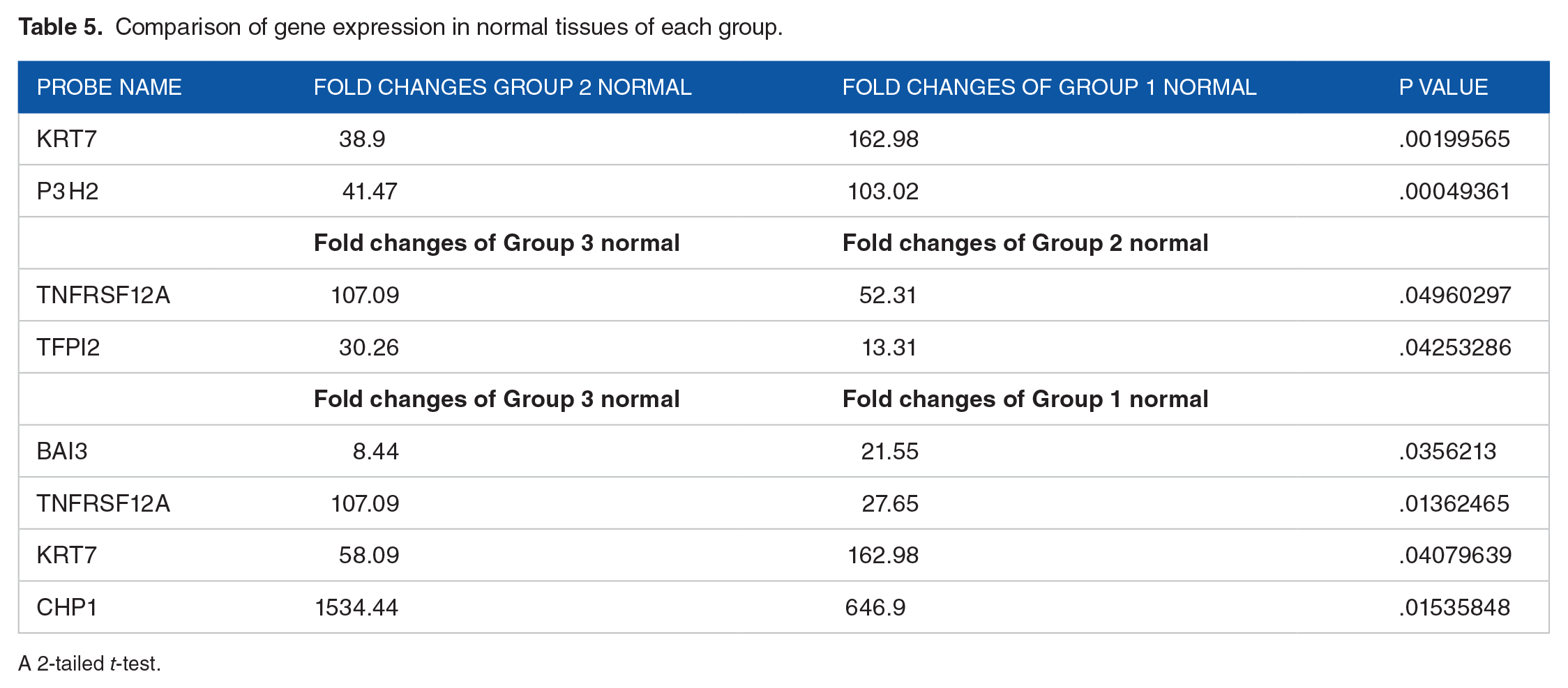
A 2-tailed t-test.

Gene expression through transcriptomic analysis of 770 genes from 18 patients with early gastric cancer. The heatmap and hierarchical clustering of all 18 samples was based on the genes with the most differential expression. (A) gray color: signet ring cell carcinoma (SRC), orange color: poor cohesive carcinoma (PCC) with positive lymph node (LN) metastasis. (B) gray color: SRC, orange color: PCC with negative LN metastasis. (C) gray color: PCC with negative LN metastasis, orange color: PCC with positive LN metastasis.
The fold change in gene expression was also compared between the groups. Groups 1 and 2 showed similar mRNA expression levels. PDK1 expression was increased in Group 1 compared to that in Group 2 (fold change value: 443.6 vs 218.74, P = .048), whereas there was no significant difference in the expression of other genes between the groups. However, there were significant differences in gene expression between Groups 1 and 3 and between Groups 2 and 3. The fold changes of 7 genes were significantly different between Groups 2 and 3, and that of 33 genes were different between Groups 1 and 3 (Tables 6 and 7). The 7 differentially expressed genes between Groups 2 and 3 included CLO7A1, EGFL7, BAI3, APOD, ROBO4, CXCL12, and SCNN1A. All genes, except SCNN1A, were more highly expressed in Group 2 than in Group 3 (Table 6). The 33 differentially expressed genes between Groups 1 and 3 included COL7A1, COL1A1, SFRP2, PTPRM, BNC2, TAL1, BAI3, NRXN3, MMP2, FLT4, SPARC, MEOX2, EGFL7, THY1, FAP, COL1A2, TIE1, OGN, ROBO4, IGF1, SNAI2, COL6A3, RUNX1T1, PDGFRB, ITGA11, THBS2, B3GNT3, BCAS1, SLC44A4, CHRNA7, CHP1, SCG2, and PROK2. B3GNT3, BCAS1, SLC44A4, CHRNA7, CHP1, SCG2, and PROK2 were more highly expressed in Group 3 than Group 1, and the other genes were expressed more highly in Group 1 than Group 3 (Table 7).
Comparison of gene expression in Group 2 and Group 3. Gene expression in cancer tissues of each group was compared. Gene expression levels expressed as fold change after the normalization step were used for comparison.

A 2-tailed t-test.
Comparison of gene expression in Group 1 and Group 3. Gene expression in cancer tissues of each group was compared. Gene expression levels expressed as fold change after the normalization step were used for comparison.
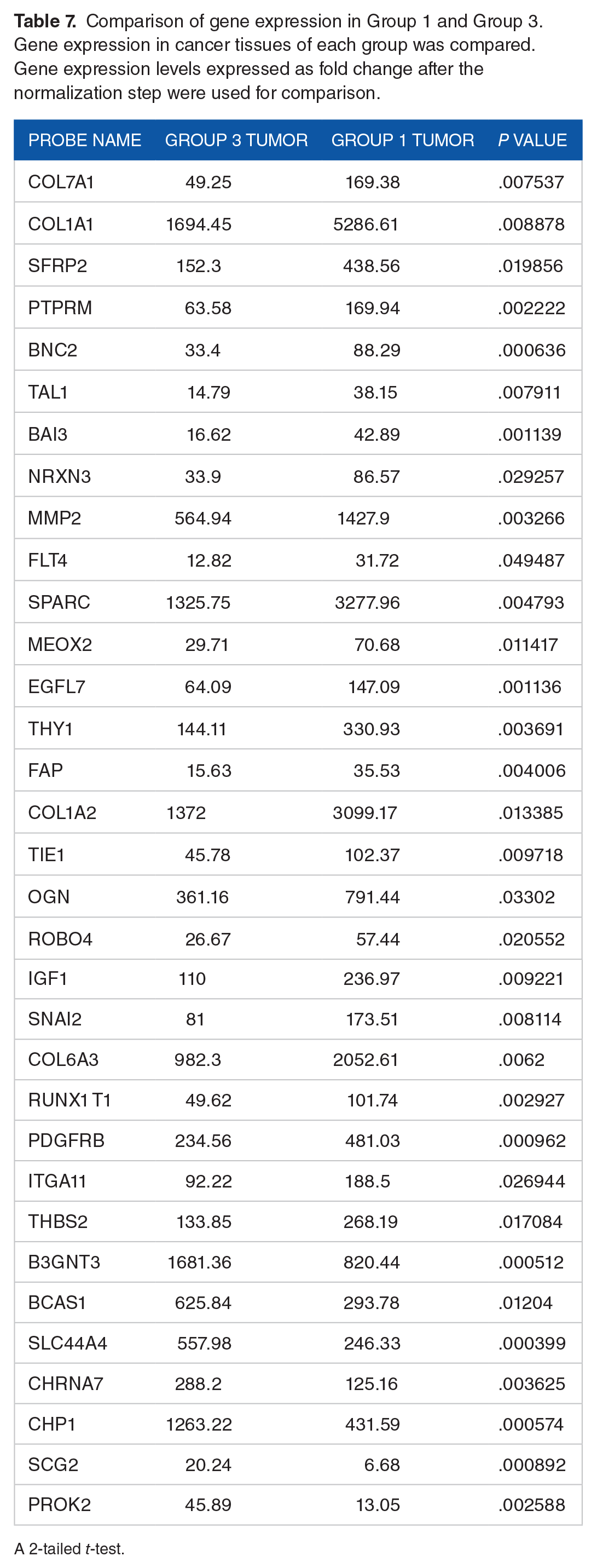
A 2-tailed t-test.
Discussion
Owing to their morphological similarities, both SRC and PC are classified as diffuse gastric cancer according to the Lauren classification. 13 However, SRC and PC are quite different in their biological behaviors.4 -6,14 Although the WHO recently proposed a new classification of gastric cancer that separates SRC and PC, 15 there are limited data on why these 2 morphologically similar carcinomas exhibit different biological behaviors. Similar to our study, a Korean study evaluated the genetic differences between SRC and PC in gastric cancer 16 and showed that PC was associated with greater depth of invasion, LN metastasis, and poorer prognosis compared to SRC. The study also identified mutations in TP53, BRAF, PI3CA, SMAD4 and RHOA that were associated with PC. 16 However, they performed targeted sequencing using multiplexed polymerase chain reaction (PCR) (Ion AmpliSeq) custom panels, whereas we performed transcriptome analysis to assess the differences of genetic expressions from different perspectives. Given that there is very little genetic information on PC and SRC, we believe that transcriptome analysis offers significant advantages over DNA sequencing as it generates a comprehensive genome-wide picture of gene expression.
In this study, PC showed more altered genetic expressions compared to SRC. The nCounter Pancancer Progression Panel is comprised of 770 genes from the various steps of the cancer progression including angiogenesis, epithelial-mesenchymal transformation, metastasis, tumor growth, and tumor invasion. An increase in the number of genetic alterations in cancer tissues may be associated with increased aggressiveness. We found that the PC group with LN metastases (Group 1) showed more gene expression changes than the PC group without LN metastases (Group 2). Furthermore, compared to SRC, PC showed greater changes in gene expression in our study.
As SRC and PC are classified together as diffuse-type cancers in the Lauren classification, we expected to find some commonalities in gene expression. However, we found that only 7 genes, including MMP3, were commonly affected in all 3 groups. The expression levels of the other genes were significantly different (Figure 3). Based on the results of this study, it is possible to consider the possibility that SRC and PC are carcinomas with different genetic backgrounds. However, it is unclear whether SRC and PC originate from similar cells and diverge later in the process or originate from completely different cell types.
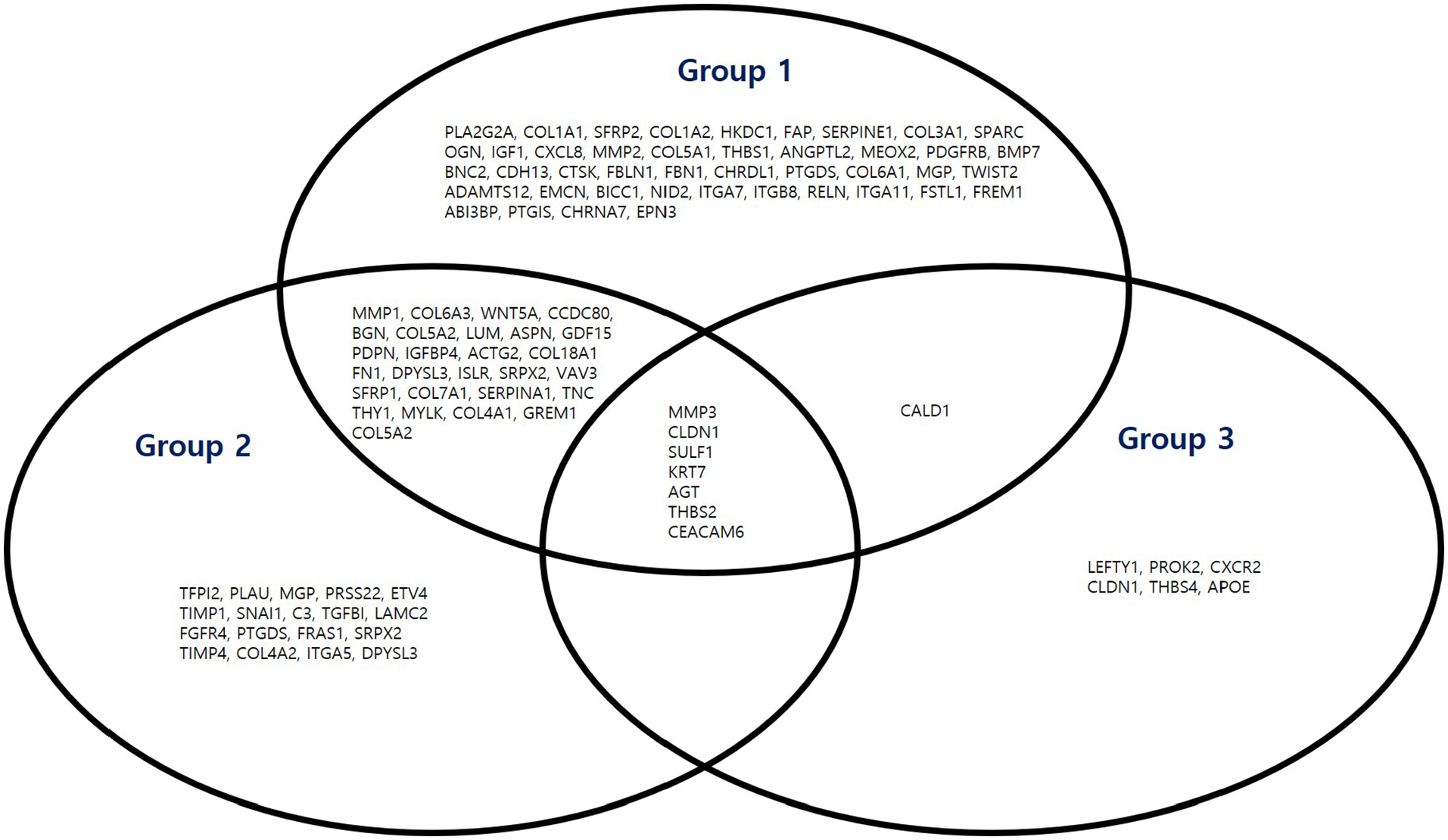
Gene expressions of cancer tissues compared to normal tissues by group. These are the results of comparing the cancer tissues of each group and each normal control group. Using the Venn diagram, the uniquely and the commonly altered genes for each group were indicated.
Comparison of the gene expression changes between the groups revealed that only PDK1 expression was different and increased in Group 1 compared to that in Group 2 (443.6 vs 218.74, P = .048). The PDK1 gene has been shown to be associated with epithelial-mesenchymal transformation, which affects the metastatic potential of gastric cancer. 17 PDK1 gene may play an important role in LN metastasis of PCs at the EGC stage. However, the statistical significance is close to .05, so more research is needed to draw this conclusion.
More genes showed an increase in PC (Groups 1 and 2) compared to that in SRC (Group 3). Genes including SCNN1A, B3GNT3, BCAS1, SLC44A4, CHRNA7, CHP1, SCG2, and PROK2, were highly expressed in SRC. SCNN1A, B3GNT3, BCAS1, SCG2, and PROK2, like the other genes, are oncogenes associated with poor prognosis or cancer progression.18 -23 However, CHP1, CHRNA7, and SCL44A4 are not associated with cancer progression. CHP1 has been shown to inhibit cancer cell growth and angiognenesis. 24 CHRNA7 acts as a tumor suppressor in pancreatic cancer, and SLC44A4 is associated with better survival in renal cell carcinoma.25,26 Interestingly, CHRNA7 expression was decreased in cancer tissues compared to normal tissues in Group 1. The expression of 3 genes, including CHRNA7, VAV3, and EPN3, was decreased in cancer tissues compared to that in the control in Group 1, and VAV3 expression was decreased in cancer tissues compared to that in the control in Group 2 (Tables 2 and 3). Downregulation of EPN3 causes apoptotic resistance in gastric cancer. 27 However, overexpression of VAV3 was shown to be related to poor prognosis in gastric cancer. 28 It is unclear whether the reduced expression of VAV3 in Group 1 cancer tissues is a bias unique to this study, or whether PC exhibits different gene expression compared to the other histologic types. A comparative analysis between groups performed in this study clarified the differences of genetic expressions between SRC and PC, and confirmed that SRC harbors less-aggressive expressions of genes than PC.
To confirm the mRNA expression and the prognosis of gastric cancer, additional evaluation using a public database was performed. According to The Human Protein Atlas (https://www.proteinatlas.org/humanproteome/pathology), roundabout guidance receptor 4 (ROBO4) and apolipoprotein D (APOD), which were more highly expressed in Group 2 than in Group 3, were prognostic factors for gastric cancer. High expression of these 2 factors suggests a poor prognosis. ROBO4 was also more highly expressed in Group 1 than in Group 3, suggesting that ROBO4 may be a major factor in determining different prognoses in SRC and PC types of EGC. According to The Human Protein Atlas, other genes that showed differences in expression between groups were not prognostic factors for gastric cancer. Robo 4 is an endothelial-specific receptor which is related to many types of cancers including bladder cancer, colorectal cancer, pancreatic cancer, and hepatocellular carcinoma. Its aberrant hypermethylation influence on endothelial cell migration, proliferation, and angiogenesis and the maintenance of vasculature homeostasis. 29
This study has several limitations. This was a small, single-center study. Owing to limited research funding, a large number of patients could not be enrolled. Second, we were unable to enroll patients with SRC with LN metastasis. A review of the 10-year pathology data from our institution did not reveal any case of LN metastasis in patients with SRC confined to the mucosal layer. Although we estimated that PDK1 might be a factor that could affect LN metastasis in EGC of PC histology in this study, we could not research how it was in SRC due to this limitation. Finally, contrary to our expectation, several genes showed differential expression between SRC and PC, thus making it difficult to identify a definitive gene that maybe used as a biomarker.
Conclusion
In conclusion, gene expression patterns were different between SRC and PC, suggesting the possibility that the 2 carcinomas may have different biological origins. Also, the expression of ROBO4 may play an important role in the prognosis of SRC and PC type of EGC. Further research is needed to support and solidify these findings.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work(research) was supported by Chungnam National University Hospital Research Fund, 2019 and the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (grant no. 2019M3E5D1A02068558).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SHKa, MKY, and HYJ contributed to conception and design of the study. KBJ, HSL, HJJ, SHKa, and MKY organized the database. SHKa, MKY, HSE, and HSM performed the statistical analysis. ESL wrote the first draft of the manuscript. SHKi, JKS, BSL, and HYJ wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.