
Abstract
Introduction:
Pretreatment inflammatory markers were applied to predict the prognosis of colorectal cancer. However, the role of these markers in predicting survival in patients with synchronous colorectal liver metastasis (CLM) is rarely reported. Notably, lymphocyte-to-monocyte ratio (LMR) was mainly reported in hematologic malignancies and is worth to be further explored to predict the survival of synchronous CLM.
Methods:
Totally, 196 patients who were diagnosed with synchronous CLM were enrolled. Their clinical and laboratory data before treatment were collected, retrospectively. Univariate and multivariate analyses were performed to analyze the inflammatory biomarkers.
Results:
LMR (P = .002) and lactate dehydrogenase (LDH) (P = .017) were significantly related to the progression-free survival (PFS). More factors such as neutrophil-to-lymphocyte ratio (NLR) (P = .011), carbohydrate antigen 19-9 (CA19-9) (P = .001), number of metastatic foci (P = .006), and adjuvant chemotherapy (P = .027) were correlated with overall survival (OS). In multivariate analysis, LMR remained statistically associated with PFS (P = .003). Regarding OS, LMR (P = .016) and LDH (P = .013) were significantly independent predictive factors.
Conclusions:
The higher LMR and lower LDH were strongly correlated with better survival in synchronous CLM patients. In addition, the result also indicated that enhanced LMR was related to better PFS. The LMR and LDH can be used to predict prognosis of the synchronous CLM.
Introduction
Colorectal cancer (CRC) is the fourth common carcinoma in China based on the statistics published in 2018. 1 About 376 300 new patients were diagnosed and 191 000 patients died because of colorectal cancer in 2015. 2 Approximately 20% newly diagnosed patients were found with metastasis and the number of these patients has not been decreased with the early diagnosis of CRC. 3 Regarding human portal circulation, the liver is the most common site of metastasis in CRC patients. About 50% of CRC patients developed live metastasis site eventually during the full course of the disease and 14% to 18% patients were diagnosed with synchronous colorectal liver metastasis (CLM). 4 Both neoadjuvant combinational chemotherapy and liver resection play an important role in prolonging survival and improving performance status, and liver resection is still the golden standard. However, only 20% of patients were suitable for surgical resection. 5 And the prognosis of the patients who received the same treatment was quite different, which is hard to be predicted.
The systemic inflammatory response in prognosis of CRC patients has been well studied.6 -9 The pretreatment inflammatory markers such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) were related to the occurrence of systemic inflammation and the survival of the CRC patients.6,10 -14 Besides above inflammatory markers, carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9),15 -17 carbohydrate antigen (CA125), and lactate dehydrogenase (LDH) level also showed significant prognostic value of CRC patients in different stages.18 -20 However, these factors were rarely mentioned in synchronous CLM patients 15 and the relationship between LMR and prognosis had not been reported individually. As mentioned above, only 20% of the primary site in patients with synchronous CRC patients can receive surgical resection; other patients would be treated with concurrent radiochemotherapy or some other regimens such as chemotherapy, radiotherapy alone, which was based on the status of the patients. In this study, we analyzed the correlations of these markers with prognosis in synchronous CLM patients.
Method
Patients
From a retrospectively collected West China Hospital (Sichuan, China) database, CRC patients were included between January 2010 and December 2015. Eligible patients met the following criteria: (1) patients with CRC were histologically confirmed; (2) patients were initially diagnosed with synchronous CLM; (3) the Eastern Cooperative Oncology Group (ECOG) status of patients was smaller than 2; and (4) clinical records, including patients’ characters, treatment strategy, follow-up information, and laboratory data before treatment, were available and complete. Patients with clinical evidence of acute or chronic systematic inflammatory, autoimmune disease, other malignant neoplasms, or hematologic diseases which may affect the inflammatory markers were excluded. In addition, patients with lack of pretreatment markers (obtained prior to anticancer treatment) were also excluded. The Ethics Administration Office of West China Hospital, Sichuan University approved our studies. Informed consents were approved waiver by the Ethics Administration Office of West China Hospital.
All participants and/or their legal guardians signed a statement confirming that informed consent was obtained. All methods were carried out in accordance with relevant guidelines and regulations.
Data extraction
Eligible patients’ clinical data, including age, sex, primary cancer site, tumor stage (T stage, N stage), pathological class, differentiation, number of liver metastasis, size of liver metastasis, primary site, lymphovascular invasion, perineural invasion, and treatment strategies, were collected via electronic medical records. The laboratory data were collected 10 days prior to the first antitumor treatment. The laboratory tests contained circulating tumor markers (CA 19-9), biochemical blood tests (LDH), and full blood count (neutrophils count, lymphocytes count, monocytes count, hemoglobin, and platelets). All the eligible patients were staged according to the American Joint Committee on Cancer tumor-node-metastasis (AJCC-TNM) stage 7th edition. 21 The NLR and PLR were calculated by dividing the absolute number of neutrophils and platelets by the absolute number of lymphocytes, respectively. The LMR is defined as the monocyte-to-lymphocyte ratio. The involved patients were followed up until December 2018 or their death. The primary endpoint of this retrospective trial was progression-free survival (PFS) and secondary endpoint was overall survival (OS). The OS measured from the date of pathological diagnosis to death. The PFS measured from the date of the synchronous CLM diagnosis to progression. We applied the response evaluation criteria in solid tumors (RESIST) to categorize the treatment response of every patient as 1 of the 4 following degrees: complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). 22
Statistics analysis
Statistical analysis was calculated by the Statistical Package of the Social Sciences (SPSS) software for windows, version 22.0. A value of P of .05 or less was set to be significant. Receiver operating characteristic (ROC) curves were applied to obtain the optimal cut-off levels for NLR, PLR, LMR, LDH, and CA19-9 based on OS, retrospectively. The χ2 test or the Fisher exact test was used in comparing the different characteristics between groups and Student t test was used for calculating the continuous variables. The impact of prognostic variables on OS and PFS was compared by the log-rank test and estimated by the Kaplan-Meier method. Hazard ratio (HR) and associated 95% confidence interval (95% CI) were obtained by the Cox proportional hazard regression models analysis. Only the significance variables at univariate analyses would be included in multivariate analysis, which could be used to test independent significance.
Results
Cut-off values for pretreatment makers
In accordance with the ROC curves, the optimal cut-off value was 2.93 for NLR, for which an area under the curve (AUC) value was 0.631 (95% CI = 0.544-0.719, P = .005). Based on the same method, the cut-off values for PLR, LMR, CA19-9, and LDH were 183.89, 3.27, 134.75, and 188.5, respectively. The AUC values were 0.526 (95% CI = 0.434-0.617, P = .582), 0.552 (95% CI = 0.465-0.639, P = .270), 0.664 (95% CI = 0.572-0.756, P = .002), and 0.618 (95% CI = 0.530-0.730, P = .012), respectively. Then, according to the cut-off values, the patients were separated into high- and low-level groups.
Baseline characteristics
Patients diagnosed with CRC in West China Hospital were enrolled and 196 patients meting the inclusion criteria were included in the studies. The median age of the eligible patients was 61.5 (27-86) years and 125 (63.7%) patients were men and 71 (36.3%) were women. Of these patients, 33.1% received neoadjuvant chemotherapy. The primary tumor site of 25.5%, 23.9%, 42.8%, and 7.8% patients was located in right colon, left colon, rectum, and colon transversum, respectively. The primary tumor of 67.8% synchronous CLM patients was well differentiated. The basic characteristics were listed in Table 1. Between the high and low groups, there were significant differences in tumor size (NLR: P = .018; PLR, P = .023; LMR P = .016).
Baseline characteristics of the study population.
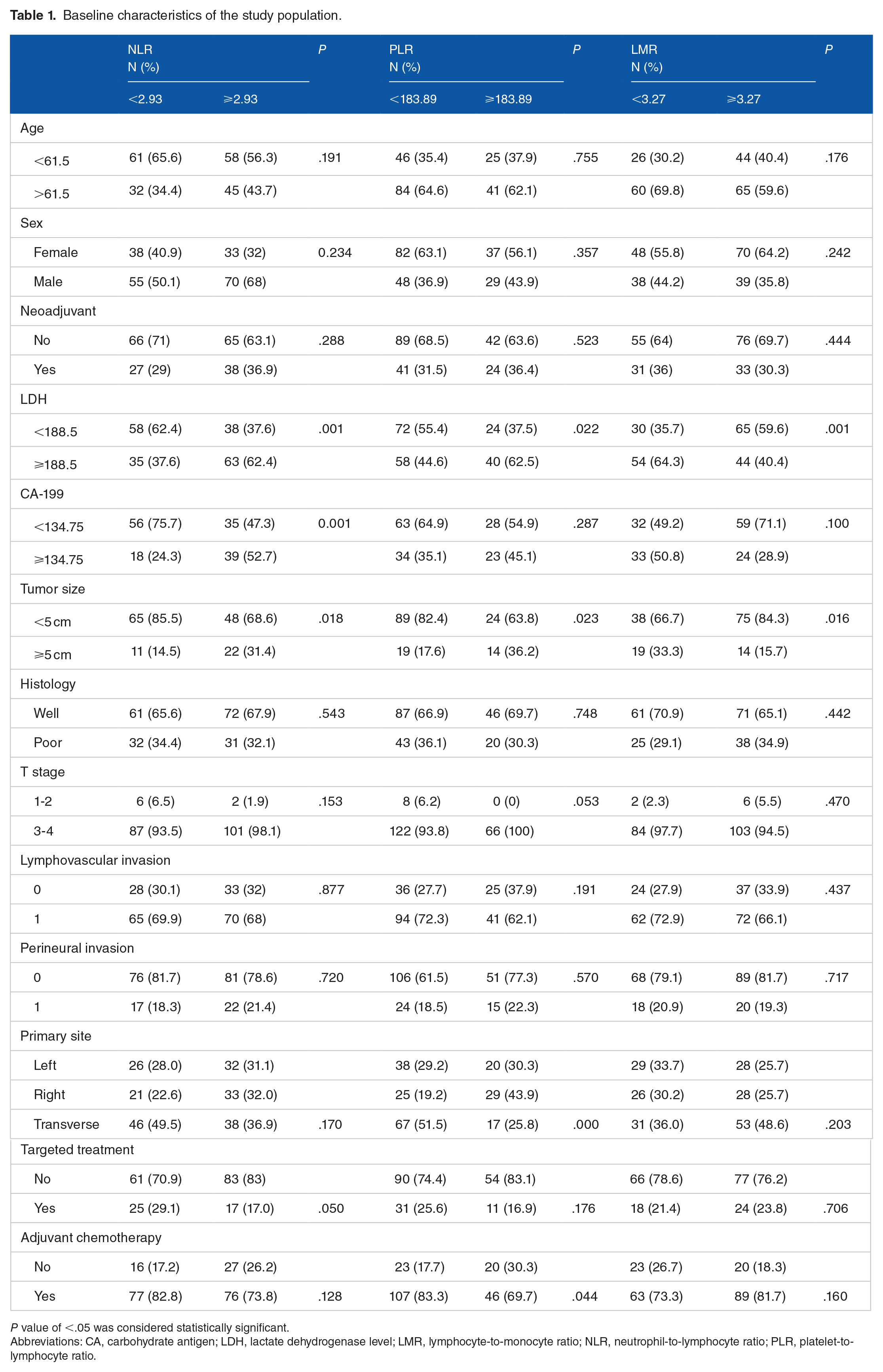
P value of <.05 was considered statistically significant.
Abbreviations: CA, carbohydrate antigen; LDH, lactate dehydrogenase level; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Univariate analysis
The median PFS was 8.00 (6.00-10.00) months and the median OS was 19 (15.5-23.00) months. According to the analysis for PFS, survival of patients with higher LMR was better than the patients with relatively lower LMR (11.00 vs 6.00, P = .002). Patients with decreased LDH (LDH < 188.5) also had favorable PFS than patients with increased LDH (11.00 vs 6.00, P = .017). Regarding OS, abdominal lymph node metastases did not influence the OS (P = .788). Elevated OS was also found in patients with decreased LDH (30.00 vs 11.00, P = .000). The NLR (25.00 vs 15.00, P = .011), number of metastatic foci (62.00 vs 19.00, P = .006), adjuvant treatment (23.00 vs 9.00, P = .027), and CA19-9 (25.00 vs 13.00, P = .001) were also significantly associated with the OS, in which higher level index patients with single metastatic foci possessed better OS than those with relatively lower index. The details of these results were listed in Table 2. Kaplan-Meier curve demonstrated that NLR, LMR, and LDH were significantly associated with OS, and LMR and LDH were significantly associated with PFS (Figure 1).
Univariate analysis of factors associated with survival.

P value of <.05 was considered statistically significant.Abbreviations: CA19-9, carbohydrate antigen 19-9; CI, confidence interval; HR, hazard ratio; LDH, lactate dehydrogenase; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PFS, progression-free survival; PLR, platelet-to-lymphocyte ratio.

Kaplan-Meier curves of (A) PFS and (B) OS for NLR (NLR = 2.93). Elevated NLR was significantly associated with poor PFS (P = .434) and OS (P = .011). Kaplan-Meier curves of (C) PFS and (D) OS for PLR (PLR = 183.89). Elevated PLR was significantly associated with poor PFS (P = .196) and OS (P = .059). Kaplan-Meier curves of (E) PFS and (F) OS for LMR (LMR = 3.27). Elevated LMR was significantly associated with better PFS (P < .001) and OS (P < .001). Kaplan-Meier curves of (G) PFS and (H) OS for LDH (LDH = 188.5). Elevated LDH was significantly associated with poor PFS (P = .003) and OS (P < .001). LDH indicates lactate dehydrogenase level; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PFS, progression-free survival.
Multivariate analysis
The multivariate analysis for PFS and OS was adjusted for significant markers in univariate analysis, which was shown in Table 3. In multivariate analysis, a variable that remained statistically associated with PFS was LMR (HR = 0.629, 95% CI = 0.463-0.854, P = .003), in which LMR might be an independent factor in predicting the PFS of synchronous CLM. The other pretreatment factors showed no correlation with the PFS. Regarding OS, LMR (HR = 0.555, 95% CI = 0.345-0.895, P = .015) and LDH (HR = 1.806, 95% CI = 1.130-2.885, P = .013) were significantly independent factors. The results indicated that high-level LMR was associated with better survival. In contrast, high-level LDH suggested patients had poor survival.
Multivariate analysis of factors associated with survival.
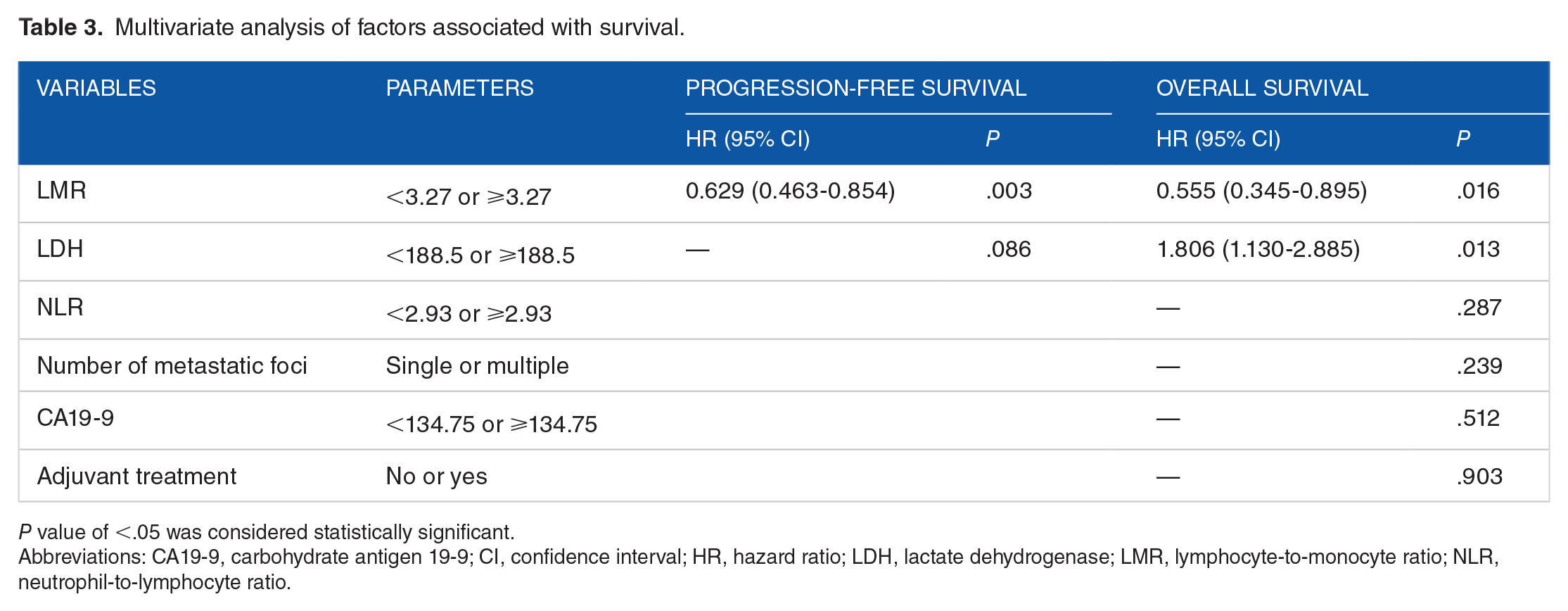
P value of <.05 was considered statistically significant.
Abbreviations: CA19-9, carbohydrate antigen 19-9; CI, confidence interval; HR, hazard ratio; LDH, lactate dehydrogenase; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio.
NLR, PLR, and LMR regarding chemotherapy response
No patients showed CR. A total of 47 patients showed PR, 38 patients had still SD, and 42 patients showed PD. Furthermore, the relationship between the response and NLR, PLR, and LMR was analyzed. The number of PR, SD, and PD was significantly higher in other groups compared with lower pretreatment NLR (P = 0.027). According to LMR and PLR, there was no significance (Table 4).
NLR, PLR, and LMR with regard to chemotherapy response.

P value of <.05 was considered statistically significant.
Abbreviations: LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Discussion
In this study, we investigated the prognostic impact of pretreatment markers in predicting chemotherapeutic response, progress, and survival in colorectal cancer patients with synchronous liver metastasis. The present results demonstrated that LMR was found to be a potentially powerful factor in predicting PFS and OS in colorectal cancer patients with synchronous liver metastasis. In addition, LDH was also related to the OS based on the results. Furthermore, it seemed that NLR was a significant factor related to the chemotherapeutic response.
Studies have shown that inflammation plays an important character in pathogenesis and progression of colorectal cancer by regulating and releasing chemokines, cytokines, growth factors, transcription factors, oncogenes, and tumor suppressor genes.23,24 Lymphocytes were quite vital cells in mediating the immunity of the host, such as cytotoxic cell death, inhibition proliferation, and migration of neoplasm cells.9,25 -27 The absolute number of lymphocytes can reflect the degree of the immune system.28,29 In addition, the decrease of peripheral blood lymphocytes was associated with cancer progression.30,31 In the tumor microenvironment, the tumor-associated macrophages can be differentiated from monocytes, which can suppress adaptive immunity and promote invasion, migration, and tumor growth. The peripheral level of absolute monocytes reflects the presence of macrophages.22,31 -38 Taking these into consideration, the LMR was a systemic inflammation factor. The relationship between prognosis and LMR has been widely reported.
The LMR was correlated to the prognosis of gastric cancer, pancreatic cancer, lung cancer, esophageal squamous cell carcinoma, lymphoma, and so on.22,39 -42 PLR and LMR were applied on predicting prognosis of patients who were undergoing resection for colorectal cancer. 14 And some studies reported that in CLM, NLR is superior to PLR in predicting survival. 43 Compared with NLR, LMR was widely discussed in hematologic malignancies such as diffuse large B-cell lymphoma, follicular lymphoma, and Hodgkin lymphoma.44 -46 The relationship between LMR and metastatic colorectal cancer was first reported in 2015. 47 LMR was also reported in previously untreated metastatic colorectal cancer patients who received FOLFOX chemotherapy. 48 And the correlation between LMR and synchronous CLM was rarely mentioned. The LMR reflects both the immune environment status of the host and the stage of the tumor progression. Lower lymphocyte count and higher monocyte count may results in lower LMR that reflected the patients’ poor antitumor immunity and enormous tumor burden. The treatment strategies stimulating the tumor immune response were considered to be used in low LMR patients. Besides pretreatment LMR, posttreatment LMR could reflect the responsiveness of chemotherapy reported in the previous studies. 49 The LMR is a marker worth to be persistently monitored.
The LDH is a cytoplasmic enzyme which is widely distributed in different tissues and is correlated with the anaerobic glycolysis.50 -53 Previous studies have reported that the accumulation of LDH might play a different role in the development of carcinoma such as breast cancer, nasopharyngeal carcinoma, malignant melanoma, and pancreatic cancer. Elevated LDH has been widely considered to be related to the recurrence and survival.19,54 In patients with unresectable colorectal liver metastases, elevated LDH negatively affected survival. 55 LDH was also an independent factor relating to poor OS and PFS in metastasis colorectal cancer. 46 However, some studies showed that pretreatment LDH was not an independent factor in resected colorectal cancer patients. 56 The level of LDH in serum can also reflect the tumor hypoxia and neo-angiogenesis. Consistent with this method, increased LDH levels seem to be related to benefit from vascular endothelial growth factor A (VEGF-A) inhibition by bevacizumab in first-line. 53 In contrast to these consequences, Cremolini reported that the continuation of angiogenesis inhibition by bevacizumab contrary to the findings of tumor invasion seems more credible in patients with decreased LDH levels.18,46 The role of angiogenesis treatment needs to be further explored.
In conclusion, the results suggested that LMR and LDH were independent markers in predicting OS, and LDH was an independent marker in predicting PFS. To the synchronous CLM patients, elevated LDH negatively influenced the PFS and OS. The baseline factors such as age, sex, tumor size, neoadjuvant chemotherapy, perineural invasion, histology, T stage, primary site, size of metastatic foci, and number of metastatic foci did not affect the survival independently.
In fact, our study was restricted because of retrospective design and single-center research which may cause selected bias. Prospective studies are required to verify the results. Besides, factors that may influence the inflammatory cell count were not taken into consideration, such as infection, ischemia, and taking drugs. In addition, the data were collected about 10 days or shorter before the first treatment and the inflammatory indexes may change all the time. Finally, cut-off values applied in the dichotomous categorization were common in clinical research, leading to an inevitable decrease in statistical power and incomplete correction in confounding factors. 57 Grouping the data was considered as importing an excessive kind of rounding with an inevitable reduce of information, which may result in effectively equivalent to losing a third of the data. The use of dichotomization may cause some extent of false positive results. 58
Conclusions
In this study, pretreatment LMR was an independent prognostic factor of OS and PFS in synchronous CLM patients. High-level LMR and low-level LDH were strongly correlated with better prognosis in synchronous CLM patients. The LMR and LDH can be used to predict prognosis of the synchronous CLM. The LMR shows excellent prediction value, which is really worth to be explored.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
QL and XM mainly generated the idea. QL collected the data. QL, LC, and HJ wrote the manuscript. ZH, YZ, and YL helped correct the grammar and did some statistical work.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The Ethics Administration Office of West China Hospital, Sichuan University approved our studies. All participants and/or their legal guardians signed a statement confirming that informed consent was obtained. All methods were carried out in accordance with relevant guidelines and regulations.