
Abstract
Background/aim:
Low dose rate brachytherapy has been used as salvage therapy for locally recurrent prostate cancer (PC) after primary external beam radiation therapy (EBRT), along with surgery and cryotherapy. All these techniques, in particular, when applied to the whole gland, involve a relatively high risk of toxicity and may worsen the patient’s quality of life. Our aim is to evaluate the results of whole-gland salvage brachytherapy (SBT) after primary EBRT in terms of toxicity, functional outcomes, and efficacy.
Materials and methods:
We retrospectively reviewed clinical data on 19 patients consecutively treated with SBT at our institution between June 2012 and November 2015. Local recurrences were identified with 11C-choline positron emission tomography/computed tomography and pelvic magnetic resonance imaging after biochemical recurrence according to Phoenix criteria (prostate-specific antigen nadir + 2). Low dose rate brachytherapy was performed by 125I permanent seeds implantation to the whole prostate gland, with a prescription dose of 130 Gy. At the time of SBT, only 2 patients were receiving androgen deprivation therapy. Acute and late toxicities were recorded using the CTCAE 4.0 scoring system. Quality of life was assessed using IPSS (International Prostate Symptoms Score) and IIEF (International Index of Erectile Function) questionnaires at baseline and 6, 12, and 24 months after SBT, and the respective mean values were compared using Student t test. Biochemical relapse-free survival (BRFS) was also calculated.
Results:
Median follow-up after SBT was 24 months. Of 19 patients, 2 patients experienced a G3 cystitis (10.2%) and 1 patient experienced a G4 proctitis (5.3%), respectively. Mean pre-SBT IPSS scores and 6, 12, and 24 months after SBT were 5.84, 10.22, 15.72, and 8.10, respectively. Mean pre-SBT IIEF scores and 6, 12, and 24 months after SBT were 8.42, 3.55, 7.89, and 6.40, respectively. At the time of analysis, only 2 patients showed a biochemical relapse (3-year BRFS 85.2%). The Student t test demonstrated a worsening of functional outcome 6 months and 1 year after treatment but a subsequent improvement 2 years after SBT.
Conclusions:
Salvage brachytherapy for recurrent PC after primary EBRT seems to be a feasible treatment for selected patients. Our series revealed a severe toxicity peak 6 months and 1 year after local re-treatment and then they decrease. Early BRFS rates are good. However, these are very preliminary results so further patient accrual, long-term follow-up, and prospective trials are needed in the future.
Introduction
External beam radiation therapy (EBRT), with or without androgen deprivation therapy (ADT), is considered the standard of care for patients with localized prostate cancer (PC). Modern EBRT techniques, that is, intensity modulated radiation therapy and image-guided radiation therapy have improved both biochemical control and the late toxicity profile.1–3 Despite this, a variable rate of biochemical failure (22%-69%) is reported in literature.2,4,5 Local recurrences were usually treated with salvage ADT. To date, local treatment modalities such as brachytherapy, surgery, cryotherapy, and high-intensity–focused ultrasound (HIFU) have been increasingly proposed to patients harboring a gland-confined disease recurrence, to prevent hormonal therapy severe side effects. 6 Moreover, despite the initial response to salvage ADT, nearly all patients develop a castrate-resistant disease. A recent review by Zumsteg et al 7 confirmed that the most common initial site of PC clinical recurrence after EBRT is in the prostate itself for all the NCCN (National Comprehensive Cancer Network)–risk groups. Therefore, local re-treatments are proposed to obtain a long-term disease control and possibly cure it. Unfortunately, local treatments are not without complications, in particular when applied to the whole prostate gland. Salvage brachytherapy (SBT) appears safe and feasible in carefully selected patients.8–10 However, data on its acute and late toxicity rates and functional outcomes are still lacking. Since 2005, more than 600 patients underwent primary brachytherapy for PC at our institution, whereas an SBT program has been recently started. We present our SBT experience in terms of toxicity, functional outcomes, and early biochemical diseases control.
Materials and Methods
From June 2012 to November 2015, 19 patients with radiologically confirmed local recurrence of PC after primary EBRT, undergoing 125I low dose rate (LDR)-SBT were retrospectively reviewed. The biochemical failure was documented according to Phoenix criteria (nadir prostate-specific antigen [PSA] + 2 ng/mL) 11 and the local recurrence by both 11C-choline positron emission tomography/computed tomography (PET/CT) and endorectal coil magnetic resonance imaging (MRI). Eligibility criteria included negative systemic staging, good urinary, and bowel function (IPSS [International Prostate Symptoms Score] <7 and no proctitis) and prostate volume <50 cm3.
Low dose rate brachytherapy was performed by a permanent implant of 125I seeds with an initial air-kerma strength of 0.520 U and an initial dose rate of 7 cGy/h. The physical delivered dose to the planning target volume (PTV) was 130 Gy, corresponding to an EQD2 = 79.4 Gy, 12 considering the radiobiological values of α/β = 3 Gy and repair half-time T1/2 = 0.27 hours 13
The whole prostate gland plus a 3-mm margin to include all microscopic disease and physical uncertainties was considered for the PTV.
Target volume and critical organs, such as urethra and rectum, were outlined on transverse images taken every 5 mm from base to apex. The volume study was performed by a BK Medical Pro-Focus transrectal ultrasound. Magnetic resonance imaging sequences were used only for disease restaging.
To reduce prostate movement during the procedure, 2 stabilizing needles were inserted.
An intraoperative planning was performed using the Treatment Planning System (TPS) VariSeed Software (versions 8.0 and 8.0.2 by Varian Medical System Inc.). Combining automatic and manual positioning of preloaded needles and optimizing the results, the aim was to respect the dose-volume parameters summarized in Table 1, according to the GEC-ESTRO indications. 14
Dose-volume parameters for PTV and organs at risk in intraoperative low dose rate brachytherapy treatment.

Abbreviation: PTV, planning target volume.
During the procedure, fluoroscopic images were taken to check the implant, the coverage of the prostate, and the number of seeds.
Data on clinical presentation, primary EBRT treatment, SBT, and toxicity were collected. Acute and late toxicities were recorded using the CTCAE v4.0 scoring system. Quality of life (QoL) was assessed using IPSS and IIEF (International Index of Erectile Function) questionnaires compiled before SBT and after 6, 12, and 24 months, and the resulting scores were analyzed. Higher IPSS and lower IIEF scores indicate deterioration. Cancer control outcomes were calculated using the Kaplan-Meier method. Functional outcome was evaluated by comparing IPSS and IIEF mean values at baseline with 6, 12, and 24 months after SBT using the Student t test. A χ2 test was used to identify and compare potential risk factors for toxicity score ≥G2 (eg, time after primary treatment, age, total EBRT dose). All variables were dichotomized using median values as cutoff. P value of <.05 was considered statistically significant.
Results
Patients’ baseline characteristics are summarized in Table 2.
Population characteristics (19 patients).
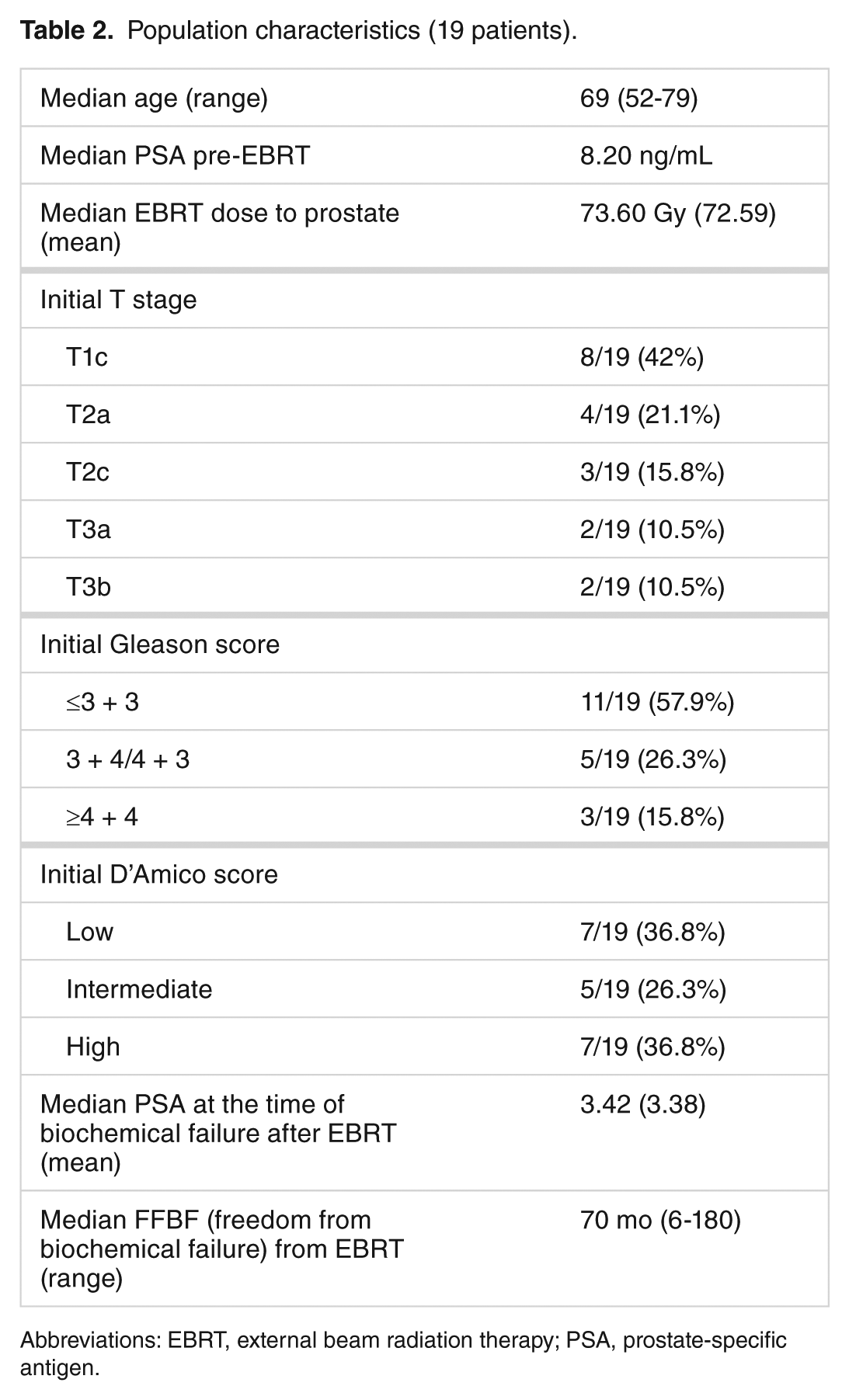
Abbreviations: EBRT, external beam radiation therapy; PSA, prostate-specific antigen.
At the time of SBT, only 2 patients were receiving ADT with luteinizing hormone-releasing hormone analogues (intraprostatic castration-resistant PC): their follow-up was 6 and 8 months, respectively. With a median follow-up after SBT of 24 months (range: 6-45), the 3-year biochemical relapse-free survival (RFS) was 85.2% (Figure 1). At the time of the present analysis, all the patients were alive except 1 who died 2 years after treatment for acute intracerebral hemorrhage without radiological evidence of brain metastases.

Kaplan-Meier curve showing the whole population’s BRFS after SBT. BRFS indicates biochemical relapse-free survival; SBT, salvage brachytherapy.
Median age at the time of SBT was 69 years (range: 52-79). Median prostate dose was 73.6 Gy (range: 70-78 Gy). Salvage brachytherapy was delivered after a median time interval of 84 months (range: 12-187) from primary EBRT. Median PSA values before SBT and after 6 months were 3.4 ng/mL (range: 2.07-6.8) and 0.45 ng/mL (0.09-2.09), respectively. Median PSA value percentage reduction between pre-salvage PSA and the first biochemical assessment after 6 months was 80%.
Two patients experienced disease progression 6 and 20 months after SBT, respectively: the first one had low-risk PC at the time of diagnosis and relapsed 70 months after EBRT with bone metastasis; the second one had high-risk disease at the time of diagnosis and relapsed 25 months after EBRT. Both patients experienced PSA increasing from the pre-SBT value to the first assessment after treatment.
Acute urinary symptoms such as frequency and transitory hematuria were common during the first 3 months after treatment.
Two patients (2/19, 10.5%) had grade 3 late genitourinary (GU) toxicity with gross hematuria, requiring blood transfusion, 7 and 13 months after SBT. Of 19 patients, 4 patients experienced G1 and 8 patients experienced G2 late GU toxicity (21% and 42%, respectively), whereas 5 patients (26.5%) did not complain any GU toxicity.
Transient G1 and G2 gastrointestinal (GI) toxicity was recorded in 4 of 19 (21.1%) and 1 of 19 (5.3%) patients, respectively. Only 1 patient had a grade 4 rectal toxicity 16 months after SBT (rectourethral fistula requiring temporary bilateral ureterostomy and colostomy).
Mean IPSS scores before SBT and 6, 12, and 24 months after the procedure were 5.84, 10.22, 15.72, and 8.10, respectively: mean IPSS score increased from pre-SBT 5.84 to 6 months post-SBT 10.22 (P = .017), reaching a peak 12 months after seeds implantation (15.72) and then lowering 24 months after SBT (8.10, P = .015). The difference between median pre-SBT IPSS score and at 12 months post-SBT was not significant, thus suggesting a nearly complete recovery of such transient toxicity.
Mean pre-SBT IIEF scores and 6, 12, and 24 months after the procedure were 8.42, 3.55, 7.89, and 6.40, respectively: mean IIEF score decreased from 8.42 before SBT to 3.55 after 6 months of the treatment (P = .019) and then raised again; 12 months after SBT, up to values very close to the pre-SBT one (7.89, P = .016) were substantially maintained 24 months post-SBT (6.40, P = .18).
Table 3 shows complete results of the comparison of IPSS and IIEF scores with the Student t test.
The t test comparing mean IPSS and IIEF before SBT and 6, 12, and 24 months after the procedure: mean values are compared with the previous measurements.

Abbreviations: IIEF, International Index of Erectile Function; IPSS, International Prostatic Symptoms Score; NS, nonsignificant; SBT, salvage brachytherapy.
One-to-one comparisons (t test) are reported in each row along with the relative P value.
A possible relationship between age at SBT, pretreatment IPSS status, T category at the time of diagnosis, hormonal treatment at the time of relapse, and GU/GI toxicity was explored. However, none of these factors appeared to be significantly linked to a toxicity grade more than G2.
Discussion
Despite the promising results in terms of biochemical and clinical disease control as well as remarkable advances in planning and delivery techniques, biochemical failure after EBRT for PC remains an issue. Prostate-specific antigen rising after EBRT is often due to local relapse. This means that treating an intraprostatic recurrence may decrease the risk of distant metastases. 15
Therefore, when a biochemical relapse occurs, disease restaging is clinically appropriate to select patients with localized disease. 11C-choline PET/CT increases restaging sensitivity over CT, MRI, and technetium scintigraphy.16–18 However, multiparametric MRI is considered a sophisticated imaging technique, able to detect and localize PC recurrence in patients with biochemical progression after definitive EBRT. 19
To date, there is no large consensus regarding management of locally recurrent PC after EBRT. Androgen deprivation therapy alone cannot be considered as a curative treatment; indeed, it may cause several, well-documented side effects. 20 Performing an effective local treatment may postpone the use of systemic therapies and possibly avoid the related toxicity and QoL deterioration. 21 As Aoun and coworkers pointed out, primary tumor, the patient, and metastatic spread to lymph nodes and distant sites are “communicating ecosystems” and this could be the biological background of the abscopal effect. 22 A growing biological rationale supports the hypothesis that local treatments may also interrupt the metastatic process or hamper the growth of occult metastatic deposits. The “seed and soil” theory postulates that local tumor control may eliminate the source of dissemination of metastatic cells. 23 In addition, the possibility of a “self seeding” process has been also postulated. According to this theory, local control of cancer relapse may also prevent “reseeding” of the primary tumor. 24 Finally, local relapse control may interfere with the development of castrate-resistant cancer cell clones. 25 Finally, yet importantly, it has been hypothesized that local failure may originate to a second wave of distant metastases.26,27 In fact, similar biological mechanisms have been clinically exploited for treatment of oligometastatic and oligoprogressive patients with PC.26,27 Actually, there are several therapeutic options for intraprostatic failures after EBRT: HIFU, cryotherapy, and brachytherapy, but, as previously mentioned, all these treatments may involve a relatively high risk of toxicity. 21
Compared with other similar experiences in the available literature, despite the relatively short follow-up period, our series can still fully consider functional issues (IPSS and IIEF questionnaires). The severe toxicity rates described in the literature vary depending on treatment and baseline patient characteristics.
In a series of 37 men treated with SBT (5-year freedom from biochemical failure [FFBF] of 65%), Burri et al 10 reported a crude rate of toxicity ≥G3 of 11% (1 prostatorectal fistula, 2 obstructive uropathies requiring transurethral resection of the prostate [TURP] and 1 gross hematuria) after a median follow-up of 86 months.
Another retrospective series of 49 patients by Grado et al 28 reported 5-year biochemical disease-free survival rate of 34% and a cumulative incidence of adverse events (grade ≥3) of 16% (7/49 patients underwent posttreatment TURP and 1/49 had to apply colostomy for rectal bleeding).
To our knowledge, a Spanish multi-institutional study including 56 patients treated between 1993 and 2007 with LDR-SBT (37/56) and low dose rate (HDR)-SBT (19/56) is the largest ever published SBT series 8 : after a median follow-up of 48 months and the reported 5-year FFBF was 77%. The incidence of grade 3 GU toxicity for LDR and HDR patients was 24% and 21%, respectively; 1 LDR-SBT patient developed a prostatorectal fistula that requiring a colostomy.
A prospective phase 2 study by Nguyen et al 29 enrolled 25 patients with intraprostatic PC failure at least 2 years after EBRT with favorable clinical features (Gleason score ≤7 and PSA ≤10 with negative restaging) for MRI-guided SBT to a minimum peripheral dose of 137 Gy. After a median follow-up of 47 months, the actuarial estimate GI and GU toxicity (grade ≥3) was 30%. In particular, 3 of 25 patients developed prostatorectal fistula 11, 12, and 29 months after SBT. The estimated PSA failure-free survival rate was 70% after 48 months of the procedure.
The use of rectal spacers might decrease the likelihood of grade 3 or higher toxicity, especially fistulization for all the cases of whole-gland SBT. 30
Unfortunately, no sufficient data are available to establish the optimal total target dose to the whole prostate, combining an acceptable toxicity profile with high therapeutic efficacy. Our LDR-SBT total dose of 130 Gy seems to be relatively low if compared with the other LDR-SBT experiences; however, our results in terms of biochemical control and toxicity outcome are similar to those reported in literature. This confirms that target volume reduction using an MRI technology that allows a “more focal” intraprostatic treatment is more important than a dose escalation on the whole gland. It is true that some studies investigate feasibility of a “focal” salvage approach to minimize severe late effects. 31 Data on 15 patients undergoing SBT with an MRI spectroscopy–based planning with median follow-up 23.3 months showed 3-year Phoenix-PFS 71.4% with no late severe side effects. 32
Another retrospective study on 20 patients treated with focal SBT revealed 3-year FFBF rate 60%, whereas only 1 patient had a G3 urethral stricture with a median follow-up of 36 months. 33 Table 4 summarizes the reviewed literature.
Results from the literature.

Abbreviations: CTV, clinical target volume; FFBF, freedom from biochemical failure; FU, follow-up; LDR, low dose rate; MRI, magnetic resonance imaging.
A novel proposed way of optimizing intraprostatic local re-treatment is reduced-dose SBT in combination with ADT: Baumann et al 36 have recently reported their experience of 25 patients treated with median 100-Gy 103Pd LDR-SBT plus 4 to 6 months of neoadjuvant and adjuvant ADT, showing favorable RFS and low toxicity profile.
Of note, we also found in our series that a longer disease-free interval from primary treatment was associated with better FFBF: this result has already been reported in literature 35 and may be related to a more efficient selection of patients with a real local recurrences rather than also harboring occult distant metastases.
Moreover, patients with pre- and post-SBT PSA reduction rate <80% had a significantly worse outcome: we hypothesized that an incomplete PSA response gives rise to distant metastases too much small to be detected by with 11C-choline PET/CT and therefore more likely to fail.
All this considered, our series are in line with the available literature, but the small number of treated patients compared with other series and the relatively short median follow-up period allow to draw quite limited conclusions about FFBF, local disease control, and survival. In addition, our study is also limited by its retrospective nature. However, toxicity rate has been acceptable, despite 3 cases with complications. Functional outcome analysis showed that urinary and erectile functional deterioration occurred 6 months after SBT, but a nearly complete recovery could be observed 12 to 24 months after implantation of seeds (Table 3).
Conclusions
With the limits of a small retrospective analysis, the present series seems to confirm that LDR-SBT is an effective treatment in carefully selected patients with local PC relapse after primary EBRT. Toxicity resulted to be acceptable, and specific functional parameters (IPSS, IIEF) worsened between 6 and 12 months after treatment but subsequently improved again almost to pretreatment levels. Very early FFBF rates also seem to be acceptable. In this regard, longer disease-free interval from primary EBRT suggests better FFBF, whereas the modest PSA reduction rate after local salvage treatment could be referred to the presence of occult widespread disease rather than to an organ-confined recurrence. Further patient accrual, long-term follow-up, larger series, and prospective studies are needed to better understand the role of brachytherapy as curative, local salvage therapy in the actual scenario of rapidly evolving techniques and advances in biology and genomics about PC, into which SBT seems to emerge as the most promising therapeutic option.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
LT and PG were responsible for data collection and statistical analysis, DG reviewed the available literature, LB reviewed the literature and draft the article, BG revised technical and physical details of brachytherapy procedure as performed at our Institute, MB, PB, BC and PV revised the paper, MM and NP revised and edited the English manuscript, FB and BLF revised the report critically for important intellectual content, SMM supervised the work and provided general. All authors read and finally approved the version to be submitted.