
Abstract
Introduction:
The accuracy of response assessment positron emission tomography (PET)-computed tomography (CT) following radiotherapy with or without chemotherapy for laryngeal/hypopharyngeal squamous cell carcinoma is uncertain.
Methods:
In all, 35 patients with laryngeal or hypopharyngeal squamous cell carcinoma who were treated between 2009 and 2014 with (chemo)radiotherapy were identified. The accuracy of response assessment PET-CT was made by correlation with clinical follow-up and pathological findings.
Results:
Of the 35 patients, 20 (57%) had an overall complete metabolic response. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for response assessment [18Fluorine]-fluoro-2-deoxy-
Conclusions:
Response assessment FDG PET-CT following (chemo)radiotherapy for laryngeal and hypopharyngeal carcinomas has a high NPV for both primary site and lymph nodes and can be used to guide treatment decisions. The PPV of residual FDG uptake at the primary tumour site is limited and requires examination and biopsy confirmation.
Introduction
Non-surgical treatment with (chemo)radiotherapy is an established standard of care for organ preservation for head and neck squamous cell carcinoma (HNSCC).1,2 The management of the node-positive neck has long been a source of controversy,3,4 with alternative approaches, including upfront or planned neck dissection regardless of response or a policy of a neck dissection only in the event of residual nodal disease. In the event of persistent primary disease following completion of treatment, salvage surgery has curative potential. Surgery to the primary site and/or neck is associated with the potential for significant morbidity.3,5,6
Multiple studies have evaluated the potential for [18Fluorine]-fluoro-2-deoxy-
In our centre, we have adopted a policy of response assessment FDG PET-CT following (chemo)radiotherapy for locally advanced HNSCC. 7 The aim of this report is to analyse the accuracy of PET-CT response assessment following (chemo)radiotherapy for locally advanced laryngeal and hypopharyngeal carcinomas.
Methods
Inclusion criteria
Consecutive patients with laryngeal/hypopharyngeal carcinoma who underwent FDG PET-CT for response assessment following curative-intent (chemo)radiotherapy between January 2009 and December 2014 were retrospectively identified from an institutional database. Electronic case notes were used to confirm patients who fulfilled the eligibility criteria for this retrospective study. Formal institutional review board approval was waived.
Eligible patients for inclusion in the analysis fulfilled all of the following criteria: (1) squamous cell carcinoma of the larynx or hypopharynx, (2) (chemo)radiotherapy with curative intent, (3) FDG PET-CT as a baseline prior to treatment, and (4) FDG PET-CT as response assessment following completion of treatment. Figure 1 shows a summary of the study schema. Patients were excluded with a history of prior therapeutic resection of primary and/or lymph node disease. Patients in whom the FDG PET-CT was performed only following response assessment after CT and/or magnetic resonance imaging (MRI) were also excluded.

Study schema. Response assessment imaging performed in routine practice at approximately 4 months following completion of (chemo)radiotherapy according to local institutional protocols. CT indicates computed tomography; FDG, [
18
Fluorine]-fluoro-2-deoxy-
Data collection
Demographic, clinical, and imaging data, including PET-CT findings, maximum standardised uptake value (SUV) at primary site and lymph nodes at presentation, and maximum SUV at primary site and lymph nodes at response assessment, were obtained from review of institutional electronic case-note records and imaging review.
Staging
Conventional staging was routinely performed by physical examination, fibre-optic endoscopy, examination under anaesthetic with biopsy where indicated, MRI or contrast-enhanced CT of head and neck region, and CT of the thorax. The FDG PET-CT was performed primarily to provide a baseline for future response assessment for patients with either bulky stage II or stage III/IV disease. Results were routinely reviewed in a specialist Head & Neck Multidisciplinary meeting, and a TNM classification, based on all available clinical and radiological data, according to the American Joint Committee on Cancer (AJCC) TNM staging 7th edition 17 was assigned.
Radiotherapy
During the early part of the study period, patients were treated with a conformal technique as previously described. 18 Intensity-modulated radiotherapy (IMRT) was subsequently implemented into routine clinical practice. During this period, a compartmental approach to target delineation was adopted. 19 Delineation of gross tumour volumes (GTVs) and clinical target volumes (CTVs) were performed manually by one of a team of radiation oncologists experienced in the management of head and neck cancer, as part of routine care (during the period of this analysis there were no formal peer review of contours in place). A primary tumour CTV was created to include at least GTV +10 mm and the anatomical compartment, modified to anatomical boundaries to include the whole larynx/hypopharynx. The high-dose nodal CTV was constructed to include the whole involved nodal level. The elective lymph node CTV routinely included levels 1b to V in the node-positive neck; nodal levels in a node-negative neck were selectively irradiated depending on tumour site and disease extent according to published recommendations. 20 The planning target volume was created by auto-expansion of the CTV by 4 mm. 18 Institutional protocols were followed with a radical treatment dose of 70 Gy in 35 fractions over 7 weeks, with lower doses to prophylactic dose regions (54-63 Gy in 35 fractions over 7 weeks). During this period, several patients entered a UK dose escalation study 21 comparing a dose of 65 Gy in 30 fractions versus 67.2 Gy in 28 fractions; other dose-fractionation regimens were occasionally used at the treating clinician’s discretion. Intensity-modulated radiotherapy was delivered with a 5- to 7-angle step and shoot IMRT technique or in the latter period of the study with a volumetric arc therapy technique.
Chemotherapy
Induction chemotherapy was used based on clinician preference, patient, and tumour factors; in general, induction chemotherapy was considered for patients with bulky disease. Standard induction chemotherapy consisted of either TPF (docetaxel 75 mg/m2 day 1, cisplatin 75 mg/m2 day 1, and 5-fluorouracil [5FU] 750 mg/m2 days 2-5, thrice weekly) for selected fit patients 22 or PF (cisplatin 80 mg/m2 day 1 and 5FU 800 mg/m2 days 2-5, thrice weekly). 18 Patients <70 years old were considered for concurrent chemotherapy. Standard concurrent chemotherapy was cisplatin 100 mg/m2 days 1 and 29. Carboplatin at area under the curve 4 was substituted for cisplatin if creatinine clearance was <55 mL/min.
Response assessment and follow-up
Response assessment and follow-up was performed according to standard institutional protocols. Tumour response was routinely assessed 4 months after the completion of treatment by clinical examination, naso-endoscopy, and FDG PET-CT; examination under anaesthetic and biopsies were performed on clinical discretion following response assessment. Patients with less than a complete response were evaluated for salvage surgery. Subsequently, patients were followed up with physical examination and flexible endoscopy every 6 to 8 weeks in the first year after treatment, every 3 months for an additional 2 years, and 6 monthly until discharge at 5 years. Patients with biopsy-proven local and/or regional disease were considered for salvage surgery.
FDG PET-CT protocol
The FDG PET-CT examinations prior to June 2010 were performed on a 16-slice Discovery STE PET/CT scanner (GE Healthcare, Amersham, UK) and from June 2010 on a 64-slice Philips Gemini TF64 scanner (Philips Healthcare, Best, The Netherlands). The PET acquisition from skull vertex to upper thighs was performed 60 minutes after administration of intravenous 18F-FDG (dose varied according to patient body weight). A silence (no talking) protocol was employed in the uptake period following tracer injection to minimise physiological tracer activity within the head and neck regions. The CT component was performed according to a standardised protocol (without the use of iodinated contrast medium) with the following settings: 140 kV; 80 mA; tube rotation time, 0.5 seconds per rotation; pitch, 6; and section thickness, 3.75 mm (to match the PET section thickness). Patients maintained normal shallow respiration during the CT acquisition. Images were reconstructed using a standard ordered subset expectation maximisation (OSEM) algorithm with CT for attenuation correction. Both non-attenuation–corrected and attenuation-corrected data sets were reconstructed.
Categorisation of FDG PET-CT response assessment
To evaluate the application of FDG PET-CT to clinical decision making, the categorisation of FDG PET-CT response for the purposes of this analysis was based on formal radiology reports. All FDG PET-CT scans were reported by a team of 3 highly experienced clinicians dual certified in Radiology and Nuclear Medicine (range of PET-CT experience, 6-10 years). To ensure consistency of reporting, all PET-CT scans were reported using specialised software (XD Version 3; Mirada Medical, Oxford, UK) using a fixed display (0-7) scaled to the SUV. Background physiological uptake within the liver and normal tissues in the neck was calculated semiquantitatively using a volume of interest placed over the relevant structure by one of the 3 experienced readers. The FDG PET-CT images were assessed qualitatively (by comparison of tumour or nodal tracer activity with background physiological uptake). Semiquantitative assessment (maximum SUV [SUVmax]) of residual tumour or nodal uptake was also documented, but this was not fundamental to the qualitative interpretation of response. Primary tumour and nodal SUVmax values were documented. Results of posttreatment FDG PET-CT were categorised into ‘positive’, ‘equivocal’ or ‘negative’ for the primary site and nodal sites separately, as previously described. 7 Areas of FDG uptake were classified as positive if uptake was focal, corresponding to a structural abnormality and of greater intensity than background liver activity. Scans were classed as equivocal if focal FDG uptake was reduced from baseline – was below liver background but above that of surrounding normal tissues. Scans were classed as negative in the absence of any abnormal focal FDG uptake or diffuse FDG uptake in the absence of corresponding anatomical abnormality on the CT which was considered to be radiotherapy related. The presence or absence of residual tissue on the CT component of the posttreatment FDG PET-CT was recorded.
Analysis and statistics
Follow-up duration was defined as from last day of radiotherapy treatment. Survival and recurrence outcomes were calculated from the last date of radiotherapy treatment. Progression-free survival (PFS) and overall survival (OS) were analysed using Kaplan-Meier product limit curves, and groups were compared with the log-rank test. Pathology from either a biopsy or surgical procedure was defined as the criterion standard for determining the presence of persistent or recurrent loco-regional disease. In patients who did not receive a biopsy, serial negative physical examinations over the follow-up period and any relevant imaging investigations were used as confirmation of disease-free status. Sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) were calculated using 2 × 2 tables constructed using clinicopathological outcomes (sensitivity = true positives × 100%/(true positives + false negatives), specificity = true negatives × 100%/(true negatives + false positives), PPV = true positives × 100%/(true positives + false positives), NPV = true negatives × 100%/(true negatives + false negatives)). Positive and equivocal responses were grouped together for this analysis.
Results
In total, 35 patients were identified for inclusion in this retrospective case-note review, 18 (51%) with hypopharynx cancer and 17 (49%) with laryngeal cancer. Median age at diagnosis was 63 years (range, 43-76 years). Of the 35 patients, 24 (69%) were men and 11 (31%) were women. All patients were World Health Organization performance status 0 or 1. Table 1 describes tumour site, subsite, TNM staging, AJCC staging, tumour histology, and treatment details. Of the 35 patients, 24 (69%) received chemoradiotherapy. Median follow-up of all patients was 27 months (range, 7-80). Median living follow-up was 38 months (range, 13-60 months).
Disease site, TNM stage, AJCC stage, histology, and treatment.

Abbreviations: 3D, three-dimensional; AJCC, American Joint Committee on Cancer; SCC, squamous cell carcinoma.
On pre-treatment PET-CT, 32 patients had an FDG-avid primary lesion and the median primary tumour maximum SUV was 11.2 (range, 3.8-53). Twenty-six patients had FDG-avid lymph node disease on baseline PET-CT and the median lymph node maximum SUV was 9.4 (range, 2.3-34). Median time to response assessment FDG PET-CT following (chemo)radiotherapy was 18 weeks (range, 9-42 weeks; interquartile range, 16.7-18.7 weeks). One patient had his or her FDG PET-CT response assessment at 42 weeks from completion of chemoradiotherapy because of a prolonged hospital admission with a chest infection. Overall, 20 (57%) of 35 patients had a complete metabolic response. A complete metabolic response was demonstrated in 19 (59%) of 32 patients with an FDG-avid primary site at baseline assessment. With regard to lymph node disease, a complete metabolic response was demonstrated in 20 (77%) of 26 patients with FDG-avid nodal disease at baseline. Table 2 demonstrates the sensitivity, specificity, PPV, and NPV for the response assessment FDG PET-CT outcomes for primary tumour alone and lymph node involvement alone (positive and equivocal responses are grouped together for the purposes of this analysis). Where primary tumour or lymph nodes were not assessable on the baseline FDG PET-CT, these were omitted from the analysis of the respective response assessments. In the overall cohort, 2-year PFS and OS were 63% and 67%, respectively. Figure 2 demonstrates PFS and OS outcomes comparing groups with a complete metabolic response, equivocal FDG uptake, or persistent FDG uptake suggestive of residual disease. A complete metabolic response was associated with superior PFS (log-rank test P = .01), although the association with OS was non-significant (log-rank test P = .11).
Diagnostic performance of response assessment FDG PET-CT in patients with locally advanced head and neck cancer after (chemo)radiotherapy.

Abbreviations: CT indicates computed tomography; FDG, [
18
Fluorine]-fluoro-2-deoxy-

(A) Progression-free survival (PFS) and (B) overall survival (OS) curves. Kaplan-Meier curves were generated between the positron emission tomography (PET)-computed tomography (CT) complete metabolic response (CMR), equivocal, and residual disease (RD) groups, and log-rank survival analysis was performed. This demonstrated a significant impact of PET-CT response assessment on PFS (P = .01) but not OS (P = .11).
Assessment of primary tumour response by FDG PET-CT and correlation with clinical outcome
Of the 35 patients, 32 had an assessable FDG-avid primary tumour at baseline. The 3 patients in whom the primary lesion was not FDG-avid on the baseline PET-CT all had low-volume biopsy-proven primary lesions (T1N1 supraglottis, T1N2b supraglottis, T1N3 pyriform fossa). Of the 32 patients, 13 (40.6%) had persistent FDG uptake at the primary site; persistent uptake was interpreted as positive and equivocal in 6 and 7 patients, respectively. An example of persistent uptake and equivocal uptake at the primary site is shown in Figures 3 and 4, respectively. Median SUV in the positive FDG PET-CT group for primary site was 4.2 (range, 2.7-9.1). Table 3 summarises the outcomes of equivocal and positive FDG PET-CT reassessments. Following clinicopathological correlation, 7 (53.8%) of 13 were classified as false positives, with a median SUV of 4.0 (range, 2.7-5.1). Four of 6 positive FDG PET-CT response assessments and 2 of 7 equivocal assessments were true positives (PPV 67% and 29%, respectively). None of the 19 patients with negative response assessments developed local recurrence at the primary site (NPV 100%).
Persistent uptake at primary site on FDG PET-CT for a patient with T3N0 left piriform sinus poorly differentiated squamous cell carcinoma treated with 70 Gy in 35 fractions of radiotherapy. (A) Baseline axial-fused FDG PET-CT image showing the metabolically active primary tumour (SUV 14.4). (B) Axial-fused FDG PET-CT image showing a partial metabolic and morphological response in the primary tumour with persistent abnormal tracer uptake (SUV 8.0) post treatment. Biopsies confirmed residual/recurrent disease at the primary site, and salvage total laryngectomy and partial pharyngectomy were performed. CT indicates computed tomography; FDG, [18Fluorine]-fluoro-2-deoxy-

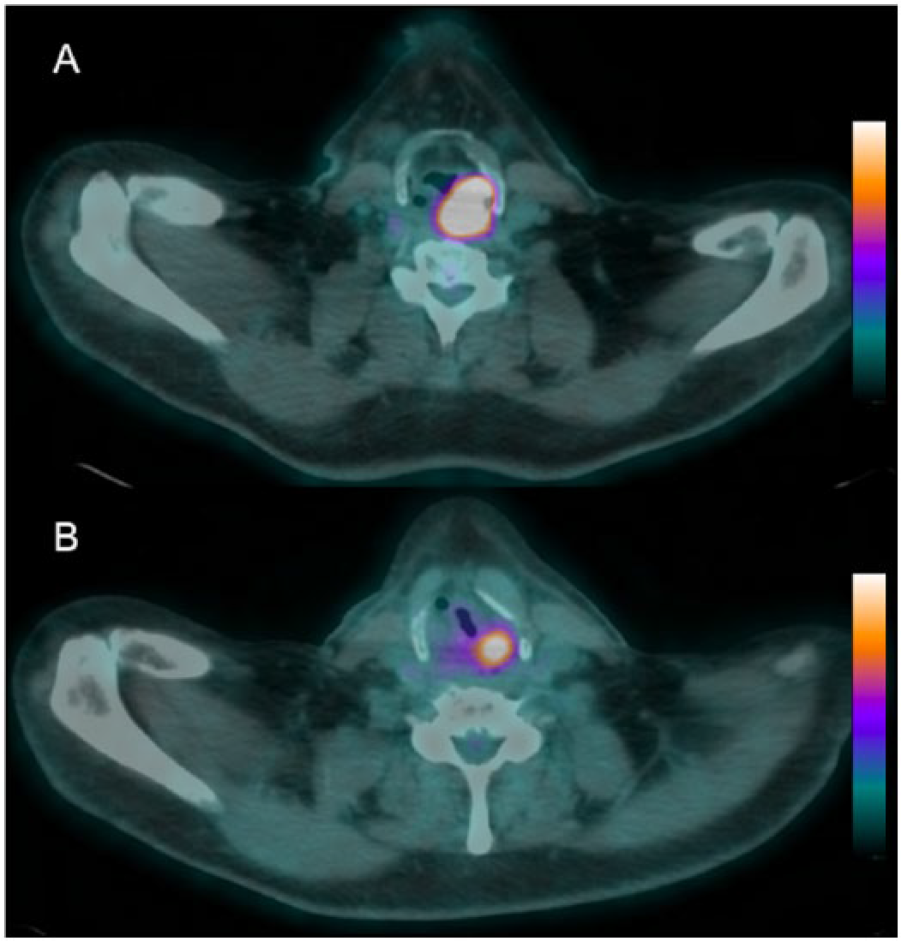
Equivocal primary and nodal site response at FDG PET-CT for a T3N2c supraglottic squamous cell carcinoma at baseline and response assessment 19 weeks post 70 Gy in 35 fractions of chemoradiotherapy with 2 concurrent cycles of cisplatin chemotherapy 100 mg/m2. (A) Baseline axial-fused FDG PET-CT image demonstrating the metabolically active primary laryngeal tumour. (B) Baseline axial-fused FDG PET-CT image demonstrating an involved left level II lymph node. (C) Response assessment axial-fused FDG PET-CT image showing equivocal (minor) residual uptake at the primary site (red arrow). Pronounced physiological FDG uptake is also present within the tonsils. (D) Response assessment axial-fused FDG PET-CT image showing equivocal (minor) residual nodal uptake (red arrow). Pronounced physiological FDG uptake is also present within the tongue and tonsils. Initially, the patient was monitored by repeated clinical assessment. After 12 months of completion of chemoradiotherapy, the patient was found on FDG PET-CT to have recurrent disease at the primary site and distant metastatic disease with mediastinal and hilar lymphadenopathy. There was no evidence of recurrent disease in the neck. CT indicates computed tomography; FDG, [
18
Fluorine]-fluoro-2-deoxy-
Summary of positive/equivocal PET-CT response assessment in primary tumour site.

Abbreviations: CT, computed tomography; FDG, [18Fluorine]-fluoro-2-deoxy-
Assessment of lymph node response by FDG PET-CT and correlation with clinical outcome
Twenty-six patients had FDG-avid lymph node involvement at baseline PET-CT; a complete metabolic response in lymph nodes was achieved in 20 (77%) patients. Of the 26 patients, 6 (23%) had persistent FDG uptake at the primary site; persistent uptake was interpreted as positive and equivocal in 5 and 1 patients, respectively. Median SUV in the positive FDG PET-CT group for nodal site was 5 (range, 2.9-11.5). Table 4 shows outcomes of equivocal and positive FDG PET-CT reassessments. All 5 of the patients with a positive scan were classified as true positives (PPV 100%), whereas the equivocal response scan was a false positive. One (5%) of the 20 patients with a negative response assessment FDG PET-CT developed nodal recurrence, with an NPV of 95%. This patient was treated with chemoradiotherapy for a T4N2c laryngeal squamous cell carcinoma.
Summary of positive or equivocal PET-CT response assessment in lymph nodes.
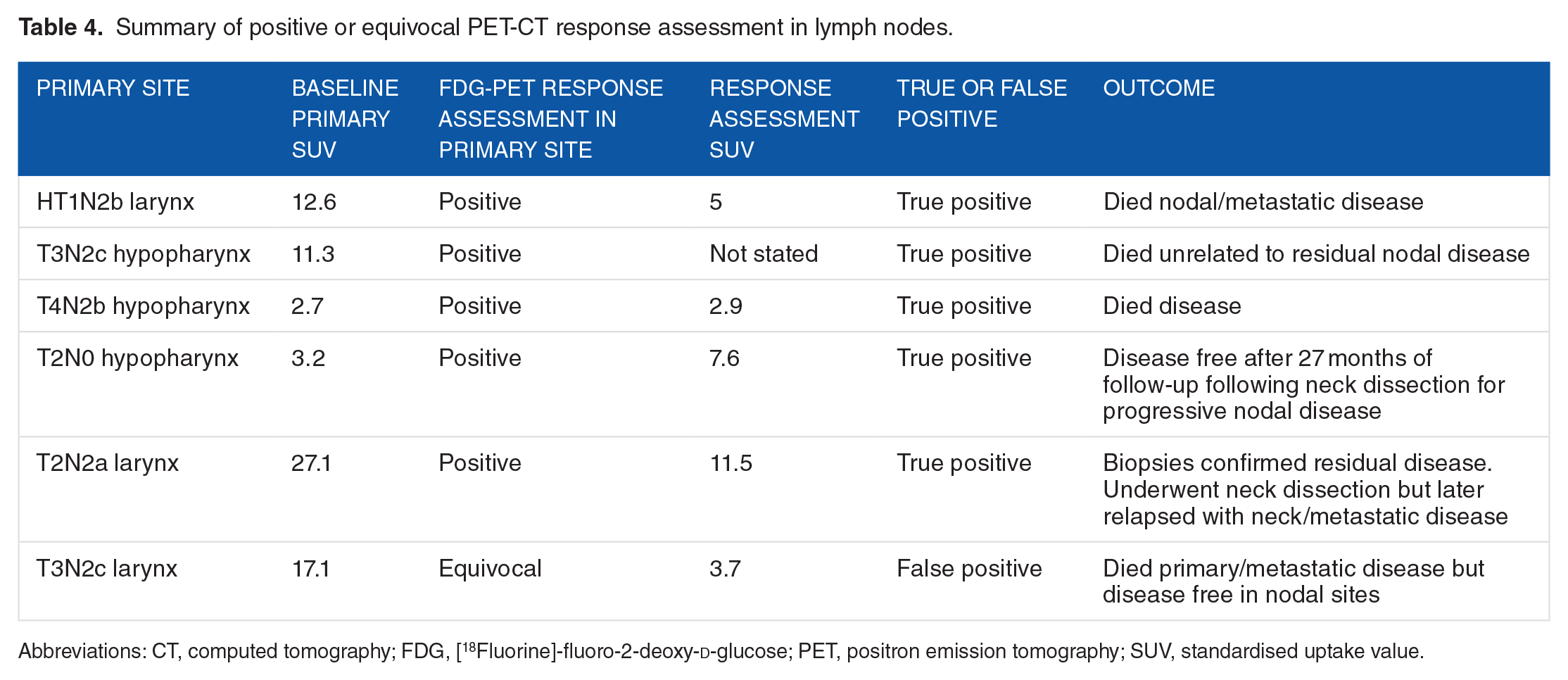
Abbreviations: CT, computed tomography; FDG, [18Fluorine]-fluoro-2-deoxy-
Detection of distant metastases by FDG PET-CT
Three of 35 patients had distant metastatic disease detected on response assessment FDG PET-CT. In all 3 cases, the patients had developed pulmonary metastases. In each of these patients, the finding of distant metastatic disease was not biopsy proven but was confirmed on subsequent imaging or clinical assessment. One of 35 patients had an indeterminate lung nodule which was found to be benign on biopsy.
Outcomes for patients with FDG-negative residual nodal tissue
Three patients were found to have residual nodal masses greater than 1 cm in size on response assessment FDG PET-CT, which were FDG negative. The maximum diameter of the residual nodes was 10, 18, and 26 mm. In each case, these patients were managed with clinical observation with no evidence of subsequent nodal disease progression. Median follow-up for these 3 patients was 41 months (range, 40-57 months).
Discussion
The high NPV of FDG PET-CT following (chemo)radiotherapy in locally advanced HNSCC has led to acceptance of this imaging technique to assess treatment response and guide the need for surgical intervention. The recent PET-NECK study has provided high-level evidence that PET-CT–guided surveillance for patients with N2/3 disease is non-inferior to a routine planned neck dissection. 15 The strategy of PET-CT-guided surveillance has been shown to be cost-effective.15,23
The characteristics of a test depend on the nature of the population to which it is applied; the accuracy of PET-CT will depend on the prognosis of the HNSCC site to which it is applied. Human papillomavirus (HPV)-positive oropharyngeal carcinoma carries a particularly favourable prognosis, 2 and a complete response in both the primary lesion and lymph nodes on PET-CT has been shown to have a very high NPV.10,12,14 Series reporting the accuracy of PET-CT response and including patients with multiple head and neck tumour sites are all heavily dominated by patients with oropharyngeal carcinoma.7-9,11,13,15 Although used as a response assessment tool following non-surgical treatment of locally advanced laryngeal and hypopharyngeal carcinomas, the accuracy of PET-CT in this context is unclear. To use PET-CT to guide a surveillance strategy, it is essential to establish whether the NPV is high with regard to both primary and nodal disease.
In this series of 35 patients with locally advanced laryngeal and hypopharyngeal carcinomas managed non-surgically, sensitivity was high for both primary and lymph node residual disease. Specificity was limited for primary disease (73%), although it remained high for lymph node disease (95%). In terms of clinical application, the NPV is critical to whether PET-CT can be used to determine which patients do not need further investigation of the primary site or a neck dissection for lymph node disease. The NPV of PET-CT was high for both the primary (100%) and nodal disease (95%). These data suggest that a negative response assessment may be used to select patients who do not require surgical intervention for either the primary or nodal disease. Based on these data, it appears that, despite the different causes of laryngeal and hypopharyngeal carcinomas, the high NPV of a complete metabolic response on PET-CT is similar to that in other studies comprising predominantly or exclusively patients with oropharyngeal cancer.7,9–15 The PET surveillance study 15 and prior prospective studies 16 have shown in a predominantly oropharyngeal cancer population that the high NPV can be used to guide a PET-CT–directed management strategy. With regard to nodal neck disease, these data show that a similar approach can be employed for patients with laryngeal/hypopharyngeal carcinoma, with avoidance of a neck dissection appropriate in the context of a complete metabolic response at sites of pre-existing lymph node disease. The high NPV of PET-CT at the site of primary disease suggests that when a complete metabolic response at the primary tumour site is achieved in combination with a complete response on clinical examination, patient can be followed up clinically without the need for further investigations (such as examination under anaesthetic and biopsies).
The PPV of PET-CT response assessment has been found to be limited in several previous series, ranging from 0% to 78%.7,8,11,13,14 Within this series of laryngeal and hypopharyngeal carcinomas, the PPV of residual metabolic activity within lymph nodes (grouping positive and equivocal scan results together) was high (83%). These data suggest that it is appropriate to proceed with a neck dissection if a complete metabolic response is not achieved at sites of nodal disease. Only a single patient had an equivocal nodal response, so it is not possible to draw useful conclusions for this sub-group. By contrast, the PPV for primary tumour assessment was limited (46%). These data suggest that the PPV of PET-CT is broadly similar for laryngeal and hypopharyngeal carcinomas compared with studies of predominantly oropharyngeal carcinoma.7,8,11,13,14 These data emphasise that residual FDG uptake at the site of the primary disease is not sufficient to proceed with salvage surgery, and the presence of persistent disease needs to be confirmed by an examination under anaesthetic and biopsy of the primary site to determine the need for surgical salvage for the primary tumour.
The optimal timing of PET-CT response assessment following (chemo)radiotherapy is unclear. It is necessary to delay response assessment long enough to allow a complete response to occur. The timing of imaging is also important in differentiating treatment-related inflammatory changes from residual disease activity. A meta-analysis has previously shown that PET-CT performed ⩾12 weeks post treatment improves diagnostic accuracy. 24 Along with others, 8 we have previously adopted a policy of performing response assessment at 4 months post treatment. There are insufficient data to compare the accuracy of response assessment PET-CT at 12 weeks post treatment, compared with later time points (as in this study). These data need to be interpreted in this context, with the accuracy of PET-CT response assessment likely to be different if performed at a different time point after treatment. Based on currently available evidence, it is appropriate to wait at least 12 weeks following completion of treatment to perform response assessment PET-CT.
One important clinical question following response assessment PET-CT is the optimal management of patients with a residual lymph node mass which is metabolically inactive. Within the PET-NECK trial, patients with any residual enlarged lymph nodes underwent a neck dissection, even if the residuum was metabolically inactive. 15 However, it has been reported that residual lymph nodes with no metabolic activity have a very high NPV, 16 especially in patients with HPV-positive oropharyngeal carcinoma. 25 In addition, it has been recognised that lymph nodes in HPV-positive disease may continue to regress longer than in HPV-negative disease. On this basis, it has been recommended that residual metabolically inactive lymph nodes in HPV-positive patients may be closely observed. 15 However, the need for surgery for metabolically inactive residual lymphadenopathy in non-HPV–positive oropharyngeal cancer remains unclear. 26 In this series, residual lymph node masses were uncommon, with only 3 patients having residual lymph node masses measuring ⩾1 cm; the largest residual lymph node measured 2.8 cm but had developed calcification. A neck dissection was not performed in any of these patients, and none have experienced lymph node disease failure. Further data are required in this context to determine the NPV of a complete metabolic response in the context of a residual lymph node mass.
In this study, treatment response was determined by qualitative interpretation by experienced readers dual trained in Radiology and Nuclear Medicine. Importantly, all patients had undergone a baseline PET-CT; this may be of value if assisting interpretation of response assessment. 27 Standardised metabolic qualitative visual interpretation criteria have recently been proposed, 9 with inter-reader interpretation reliability similar to that of the widely adopted Deauville 5-point scale for lymphoma response. 28 There is controversy over the interpretation of ‘equivocal’ levels of FDG uptake when implementing these types of qualitative scales. 29 Quantitative methods of interpretation are promising; for example, parameters such as metabolic tumour volume have been shown to be prognostic after treatment. 30 These quantitative methods currently remain within the research field.
The main limitation of this study is the retrospective nature with only 35 patients being involved. Although the retrospective nature may allow some selection bias, each of these patients had a baseline PET-CT at outset with the intention of proceeding with a response assessment post treatment; therefore, the decision on whether to use PET-CT to assess response was made at the outset prior to any clinical assessment of response. To the best of our knowledge, no other series have specifically reported on the accuracy of FDG PET-CT response imaging in laryngeal/hypopharyngeal carcinoma. It is important not to make an unwarranted assumption that the experience of using PET-CT for response assessment based largely on experiences of treating HPV-positive oropharyngeal carcinomas will be transferable to other head and neck cancer sites. Despite the limited size of our study, these data are encouraging in suggesting that PET-CT response assessment has a high NPV which is critical to guide clinical management.
Conclusions
In summary, PET-CT response assessment following (chemo)radiotherapy for locally advanced laryngeal/hypopharyngeal carcinoma has a high NPV for both primary site and lymph nodes and can be used to guide treatment decisions to avoid the need for further investigation and neck dissection, respectively. The PPV of residual PET uptake at the primary site is limited and requires examination and biopsy confirmation.
Footnotes
Peer Review:
Five peer reviewers contributed to the peer review report. Reviewers’ reports totalled 1126 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
FS, SV, MS, AFS, and RJDP conceived and designed the experiments. FS, EE, and RJDP analysed the data. RJDP wrote the first draft of the manuscript. FS, EE, and RJDP contributed to the writing of the manuscript. FS, EE, SV, MS, AFS, and RJDP agree with manuscript results and conclusions. FS, MS, AFS, and RJDP jointly developed the structure and arguments for the paper. EE and SV made critical revisions and approved the final version. All authors reviewed and approved the final manuscript.