
Abstract
Neuroleptic malignant syndrome (NMS), a potentially hazardous side effect of antipsychotic agents, usually develops within 10 days after receiving these agents. We describe a 65-year-old male who developed NMS after taking neuroleptics for alcohol dependence syndrome for several years. He was successfully treated by stopping these agents but three months later, an advanced sigmoid colon cancer was detected. He underwent surgery and the clinical course was uneventful. The present case is rare in that he developed NMS after long-term neuroleptic therapy and concurrent alimentary tract malignancy can be a risk factor for the development of NMS.
Introduction
Neuroleptic malignant syndrome (NMS) is a rare but potentially hazardous complication when using neuroleptics1,2 or antiparkinsonian drugs.3,4 NMS usually develops 4–5 days after receiving psychotic drugs or when antiparkinsonian treatment was reduced or discontinued. 5 We report a case of a colon-cancer patient who developed NMS after long-term neuroleptic treatment.
Case Report
A 65-year-old male, who had had alcohol dependence syndrome and taken nitrazepam (10 mg/day), chlorpromazine hydrochloride (25 mg/day), promethazine hydrochloride (12.5 mg/day) and phenobarbital (40 mg/day) for several years, presented with a fever (39 °C) on October 19, 2006. Under a diagnosis of the common cold, he received medications. The following day he developed marked generalized rigidity, supraventricular tachycardia (120/min), leukocytosis (18,000/mm3) and rhabdomyolysis (creatine phosphokinase{CPK} level: 7,281 IU/L). As NMS was suspected, he was transferred to the psychological department in the vicinity hospital. He was successfully treated with discontinuation of all neuroleptic agents and intense supportive care, and suffered no long-term sequelae. He then received quetiapine fumarate (100 mg/day) and was discharged from the psychological department in December. In January, 2007, he had lower abdominal pain and bloody stools, and visited our hospital. Barium enema revealed narrowing, approximately 6 cm in length, and diverticulosis in the sigmoid colon (Fig. 1). Colonoscope showed a circular ulcerative tumor in the sigmoid colon. He underwent sigmoidectomy with partial resection of bladder under general anesthesia with sevoflurane and nitrous oxide. 6 On postoperative day 5th, he had some cognitive dysfunction and there was an increase in CPK levels (342 IU/L), but the clinical course was almost uneventful. There were a circular ulcerative and infiltrative tumor and two polyps in the resected colon (Fig. 2). Microscopic findings showed that well differentiated adenocarcinoma cells in the sigmoid colon were infiltrating into the bladder. One polyp was cancer in situ and another was adenoma. There were metastases in the regional lymphnodes. He was discharged the hospital on postoperative day 14th. He has now neither NMS attack nor evidence of cancer recurrence (6 months).

Barium enema showed the stenosis and diverticulosis in the sigmoid colon.
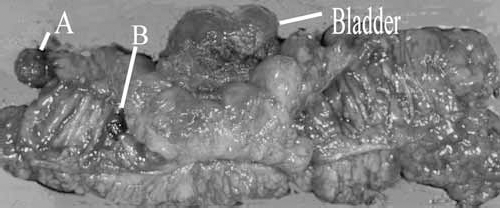
Resected specimen showed a circular ulcerogenic tumor in the sigmoid colon. There were also two polyps in its distal colon. One (A:pedunculated) is cancer in situ and another (B:protruding) adenoma.
Discussion
NMS usually develops 4–5 days after receiving neuroleptics, with 90% of cases developing within 10 days.2,7,8,9 Recent studies have shown that NMS may be induced not only by neuroleptics but also by antiparkinsonian drugs.3,4 The onset of NMS in Parkinson's disease occurred when antiparkinsonian treatment was reduced or discontinued.4,5 Both NMS due to neuroleptics and NMS due to antiparkinsonian drugs probably involve dopamine receptors, and two adverse reactions are considered to be essentially the same.3,4 Our case presented neither in the time frame of NMS due to neuroleptics nor in that due to antiparkinsonian drugs. Recently some reported patients who developed NMS after long-term uneventful treatment with neuroleptics.10,11 They did not show the reason of the late-onset. The development of NMS is reported in patients with cancer or burn.7,8,9,12 To the best of our knowledge, this is the first report of NMS associated with colon cancer. Potential risk factors for NMS are previous episodes of NMS, psychomotor agitation, dehydration and rapid increase of neuroleptic medication. 13 The blood concentrations of neuroleptics might increase in our patient, because he had the colon stenosis by cancer. Another possible mechanism is that colon cancer itself produces toxin or biochemical which causes NMS. There was also possibility that the association between colon cancer and NMS may be coincidental. Although the exact mechanism is not obvious, the chief etiology of NMS in this patient was administration of neuroleptics. As this patient had been uneventful treated with neuroleptics for several years, coexisting colon cancer could have contributed to development of the syndrome. This case indicated that concurrent alimentary tract cancer can be a risk factor for the development of NMS. NMS is a life-threatening condition and early recognition of NMS and prompt treatment can improve the potentially fatal outcome. 12 We suggested that special attention to cancer patients undergoing psychopharmacologic treatment is required in clinical oncologic practice. Some reports suggest common pathogenic mechanisms for NMS and malignant hyperthermia. 14 However in this patient there was a slight increase in CPK, the clinical course was uneventful.