
Abstract
We present a 20-year-old male patient with localized osteosarcoma arising in osteogenesis imperfecta who underwent high-dose chemotherapy together with autologous peripheral blood stem cell transplantation followed-by a successful extremity sparing surgery.
Introduction
Osteosarcoma may arise secondary to osteogenesis imperfecta (OI) and both conditions may be concomitant in some cases. Limb sparing surgery is rarely applicable in these cases. Currently, high-dose chemotherapy (HDC) and autologous peripheral blood stem cell transplantation (APBSCT) is not used yet as a treatment alternative in such cases. We present a 20-year-old male patient with localized osteosarcoma arising in OI who underwent HDC and APBSCT followed-by a successful extremity sparing surgery.
Case Report
A-20-year male patient was diagnosed as type II OI in his childhood by the presentation features of dentinogenesis imperfecta, blue sclera, frequent fractures during infancy, less frequency fractures after puberty, easy bruising, and mild short stature due to the frequent fractures. He was admitted to orthopedics clinic with complaints of bone pain, edema and swelling of the right proximal tibia. The evaluation studies by incisional bone biopsy, direct X-ray and computed tomography of the extremity, chest, abdomen and pelvis and whole body bone scintigraphy revealed a diagnosis of conventional osteosarcoma stage IIB (Figs. 1, 2 and 3). After evaluation by magnetic resonance imaging and multi-slice computed tomography preoperatively, a decision to perform HDC and APBSCT along with limb sparing surgery was made. Two cycles of neoadjuvant induction chemotherapy consisting of cisplatin 30 mg/m2, adriamycin 20 mg/m2, and ifosfamide 2.5 g/m2 were administered in three consecutive days, every three weeks, according to our institutional treatment protocol for non-metastatic osteosarcoma.(Arpaci et al. 2005). Fifteen days later, stem cells were mobilized using filgrastim (10 μg/kg/day given in two doses) and collected with a COBE spectra cell separator (Cobe BCT Inc., Lakewood, CO). The amount of collected CD34+ cells was 6.69 × 10 6 /kg. High dose chemotherapy (A total dose of ifosfamide 12 g/m2, carboplatin 1.2 g/m2, and etoposide, 1.2 g/m2 was divided in six equal doses and was given on six consecutive days) and APBSCT was performed thereafter. Eighteen days after the transplant, after the achievement of neutrophil and platelet engraftment limb sparing surgery was performed. The longitudinal size of the tumor was 6 cm and the lateral cortex of the proximal tibia was destructed. Therefore, the proximal of tibia and fibula were resected en-bloc with 2 cm of tumor-free bone beyond the distal margin of the tumor under femoral tourniquet by the experienced orthopedic oncology surgical team. The total resection length was 8 cm. The adjacent knee joint together with joint capsule were resected compartmentally with 2 cm of distal femoral bone. The frozen section of the neurovascular bundle as well as the bone marrow from distal and proximal surgical margins were reported as free of tumor at margins intraoperatively; therefore, a modular endoprosthesis was placed (Morris et al. 1994) (Image 1 and Figs. 4 and 5). No complications were encountered postoperatively. Continuous passive motion exercises were started on day 7 and full weight-bearing on the affected limb was restricted for two months after the operation. Postoperative tumor necrosis rate was reported at as 99% after pathologic examination of the resected bone. Because of the high necrosis rate in the tumor, based on our treatment protocol, the same chemotherapy regimen that was used as induction chemotherapy was given for three additional cycles as consolidation chemotherapy. The patient is currently disease-free and has a good functional score. No additional fractures have occurred in 28 months of follow-up after the transplant (Fig. 6).
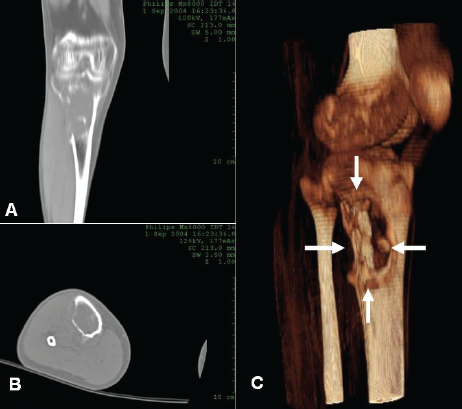
Preoperative CT images of tumor.


Preoperative anteroposterior graphy; arrows showing the tumor area and cortical destruction.

Preoperative MR images; T1 coronal section before neoadjuvant chemotherapy.

Direct graphies after the second course of neoadjuvant chemotherapy.

Postoperative direct graphies and endoprosthesis.

Postoperative functionality of the patient.
Discussion
Osteogenesis imperfecta is a genetic disorder characterized by increased bone fragility and loss in bone mass due to defective type 1 collagen (Rauch et al. 2004). Patients with OI have multiple bone fractures resulting in progressive skeletal deformities and retardation in bone growth.
Among therapeutic options in osteosarcoma cases arising in OI, amputation procedures were the most commonly used treatment approaches until today (Jewell et al. 1940; Klenerman et al. 1967; Lasson et al. 1978; Reid et al. 1979; Rutkowski et al. 1979; Gagliardi et al. 1995; Bedi et al. 1999; Maiya et al. 2002 and Takahashi et al. 2004) (Table 1). It is well-known that neoadjuvant chemotherapy combined with complete surgical excision followed-by adjuvant chemotherapy is the gold-standard treatment modality in patients with extremity osteosarcomas (Bacci et al. 2000 and Provisor et al. 1997). Histopathologic response rate to preoperative chemotherapy (namely, the tumor necrosis rate) has been shown to be the most important predictor of long-term survival for osteosarcoma patients. This was based on the assumption that an increase in the tumor necrosis rate would result in improved survival rates (Raymond et al. 1987). We demonstrated recently in a phase-II study, the effectiveness of HDC which yielded tumor necrosis rates over 90% in 82% of cases (Arpaci et al. 2005). We also used this treatment modality in this patient with osteosarcoma arising in OI. To our knowledge, no data have been presented yet about the feasibility of HDC and APBSCT in patients with osteosarcoma arising in OI. We have observed in this patient, that the placement of an endoprosthesis did not increase the rate of fracture in the operation area. This treatment procedure is shown to have many advantages such as high tumor necrosis rate, minor surgical complications and good functional results (Arpaci et al. 2005). This treatment modality appears to be feasible and effective even in patients with osteosarcoma arising in OI and should therefore be further investigated in other large studies.
Reported cases in English literature with osteosarcoma arising in osteogenesis imperfecta.
