
Abstract
Background:
The International Diabetes Federation-Diabetes and Ramadan (IDF-DAR) Practical Guidelines 2021 provide a risk stratification tool to guide the assessment of people with diabetes before they observe Ramadan. Here we conducted a survey study to explore the predictability of the IDF-DAR 2021 guidelines, and the factors associated with breaking fast, in people with type 1 diabetes (PwT1D) during Ramadan.
Methods:
This cross-sectional study included adult PwT1D living in Saudi Arabia, aged 18 years and above, who observed Ramadan 2022. Between May and August 2022, a standardized online questionnaire was used to collect data regarding socio-demographics, medical history (including the modality of T1D management and other components of the IDF-DAR risk calculator), and Ramadan fasting experience.
Results:
The study included 963 PwT1D (257 males and 706 females, mean age 26.5 ± 8.4 years). Applying the IDF-DAR risk calculator revealed that the study respondents included 66% high-risk PwT1D, 34% moderate-risk PwT1D (34%), and no low-risk PwT1D. Compared to the moderate-risk group, the high-risk group had significantly more days during which fasting was broken, a higher prevalence of diabetes complications, and more frequent diabetes-related ER visits (P < .01). Attending a pre-Ramadan education session was associated with 47% lower odds of visiting the ER during Ramadan (odds ratio 0.53; 95% confidence interval 0.34-0.82; P = .005).
Conclusion:
The IDF-DAR 2021 risk calculator predicts the risk of acute diabetes complications and ER visits during Ramadan fasting. Pre-Ramadan education sessions are important and may reduce acute complications among PwT1D during Ramadan fasting.
Plain Language Summary
Introduction
Ramadan is the ninth month of the Islamic lunar calendar. One of the fundamental pillars of Islam is obligatory fasting during Ramadan for physically capable and mentally healthy adult Muslims. 1 Throughout Ramadan, Muslims abstain from eating and drinking from dawn to dusk for 29 to 30 consecutive days. 2
Fasting during Ramadan necessitates abrupt changes to the eating times, sleeping patterns and duration, and overall lifestyle of those who observe the practice. 3 These alterations can have substantial negative impacts on individuals with chronic illnesses, particularly type 1 diabetes. People with type 1 diabetes (PwT1D) exhibit disrupted regulatory and counterregulatory mechanisms of glucose metabolism, which pose significantly increased risks during periods of fasting. Reduced oral intake of food, when inadequately countered by glucagon and epinephrine responses, may lead to hypoglycemia. Conversely, the absence of exogenous insulin during fasting can elevate glycogen breakdown, gluconeogenesis, and ketogenesis, resulting in hyperglycemia and ketoacidosis.3,4 During Ramadan fasting, PwT1D may also experience diabetic ketoacidosis (DKA), dehydration leading to secondary thrombosis, and renal impairment. 4 Although Islamic regulations exempt PwT1D and other individuals with chronic conditions from fasting, a significant number express a firm intention to fast. 5 Notably, in Saudi Arabia, the majority of PwT1D observe the fast, constituting a significantly higher proportion compared to in other Muslim countries. 6
To increase the safety of those who want to observe Ramadan, PwT1D wishing to fast should be strictly monitored in collaboration with healthcare providers (HCPs) who can provide optimal care and minimize risk. With the aim of addressing this challenge on a global scale, the International Diabetes Federation (IDF) and the Diabetes and Ramadan (DAR) International Alliance collaborated to draft an enhanced guide for the classification and management of people with diabetes during Ramadan. 7
Prior to publication of the IDF-DAR risk score of 2021, numerous guidelines were developed, including by the American Diabetes Association (ADA), and PwT1D have been consistently classified as very high risk or high risk.3,8 -14 Only a few studies have examined direct correlations between patient outcomes and calculated IDF-DAR risk scores, and most have been epidemiologic and none are specific for people with T1D.15,16 Critics of the IDF-DAR guidelines have highlighted their potential underestimation of the role of technology, as the risk scores do not directly account for patients using advanced technologies, like continuous glucose monitoring (CGM) and automated continuous subcutaneous insulin infusion (CSII). However, the authors’ rationale is that the guidelines account for the outcome of technology, rather than the mere use of the tool, as not all advanced technology users were at lower risk, and those having better glycemic control with less hypoglycemic episodes will have lower scores. The remaining evidentiary gaps highlight the need for practical validation studies to strengthen the evidence regarding the IDF-DAR guidelines, and to ensure that its algorithm promotes optimal management of PwT1D observing Ramadan.
In the present cross-sectional study, we evaluated the consistency of the IDF-DAR classification system in a real-world setting, by surveying PwT1D in Saudi Arabia who fasted during Ramadan.
Materials and Methods
Study Design and Questionnaire
This cross-sectional study was conducted in Saudi Arabia. The study protocol and procedures conformed to international ethical guidelines, and the study was approved by the Institutional Review Board of the College of Medicine, King Saud University, Riyadh, Saudi Arabia (approval no: E-21-5928, May 27, 2021).
PwT1D were invited to participate in an online survey that was launched 2 weeks after the end Ramadan in 2022, and ran from May 17, 2022 to August 31, 2022. Briefly, the questionnaire comprised 3 parts: demographic and medical data, information required to calculate the IDF-DAR score for risk stratification, and information related to Ramadan and diabetes (eg, fasting interruptions due to glucose disturbances, ER visits for diabetes-related reasons, receiving Ramadan counseling, and discussing fasting with healthcare providers). To ensure content relevance, the survey questions were based on the established IDF-DAR 2021 Practical Guidelines. Additional information was also collected, such as demographics. To enhance clarity and applicability, the questionnaire was internally reviewed by experts familiar with diabetes management and Ramadan practices. The questions were determined to be straightforward and easy to understand, considering the cultural and religious context of the target population.
The questionnaire was hosted on SurveyMonkey, and the link was shared in social media groups focused on PwT1D and advocacy for T1DM in Saudi Arabia. To encourage wider dissemination among PwT1D, it was also distributed through activists within the T1DM community, and diabetes educators and dietitians were asked to share the link with their PwT1DM circle and to post it within their professional and community groups. With this approach, we aimed to create a snowball effect to reach a larger and more diverse sample.
Participants
Inclusion criteria were as follows: Saudi PwT1D, aged of at least 18 years, intent to fast during Ramadan in the study period, and consenting to participate in the study. Exclusion criteria were diabetes other than type 1 (eg, type 2). Participants were recruited through purposive sampling, and an online informed consent was obtained from each participant. Eligible participants were stratified according to risk scores calculated based on the IDF-DAR guidelines. 6 The scores ranged from 0 (the best possible score) to 50.5 (the worst possible scores), with a score of <3.5 classified as low-risk, 3.5 to 6 as moderate-risk, and above 6.0 as high-risk. 6
Data Collection
Information was collected using standardized questionnaires in simple Arabic, which comprised 3 parts: demographic details and medical history (patient reported), questions related to specific aspects of diabetes management during Ramadan fasting, and questions related to select risk factors mentioned in the IDF-DAR classification system. 6 These questionnaires were distributed using various online social media platforms, and PwT1D were targeted through known private groups on telegram, WhatsApp, and X. The questionnaire was also shared with diabetes educators and physicians, who forwarded it to PwT1D, allowing for snowball sampling. The main variables of interest included risk factors related to breaking fasting, adherence to diabetes management practices during Ramadan, and diabetes-related emergency room (ER) visits.
Statistical Analysis
Sample size calculation was performed, using G*Power version 3.1.9.4 to estimate the prevalence of individuals at high risk when fasting, according to the IDF-DAR risk stratification. Based on a previously reported high-risk prevalence of 56.9%, 17 it was determined that we required a sample size of n = 385 to achieve a 95% confidence interval (CI) with a 5% margin of error.
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 26.0 (IBM, Chicago, IL, USA). Descriptive statistics—including medians, interquartile ranges (IQR), frequencies, and percentages (%)—were used to present categorical and continuous data. Comparative analyses between groups were conducted using appropriate statistical tests, including the Mann-Whitney U test for non-normal continuous variables, and the chi-square or Fisher’s exact tests for categorical variables. Multinomial linear regression models and risk estimates were used to identify significant risk factors associated with breaking fasting and ER visits secondary to glycemic disturbances. A P < .05 was considered significant.
Results
Table 1 presents the demographic characteristics of all 963 respondents (73.3% females), and differences between the age- and body mass index (BMI)-matched moderate-risk (N = 325, 73.8% females) and high-risk (N = 638, 73% females) groups. Table S1 presents a breakdown of the respondents according to region, showing that the greatest proportion of respondents were from the Riyadh region (n = 380, 39.5%). Notably, 66% of respondents were categorized as high-risk, and none were categorized as low-risk. As expected, the median score of the high-risk group was significantly higher than that of the moderate-risk group (P < .001). Furthermore, the prevalence of having a T1D duration of >10 years was significantly higher among high-risk PwT1D than among moderate-risk PwT1D (57.4% vs 49.8%; P = .0003). Consequently, the high-risk group also exhibited a significantly higher prevalence of complications, including retinopathy (P = .03) and neuropathy (P = .02), compared to the moderate-risk group. The risk groups did not differ in terms of education, other complications, or presence of autoimmune comorbidities (Table 1).
Demographic and Clinical Characteristics of the Study Participants.
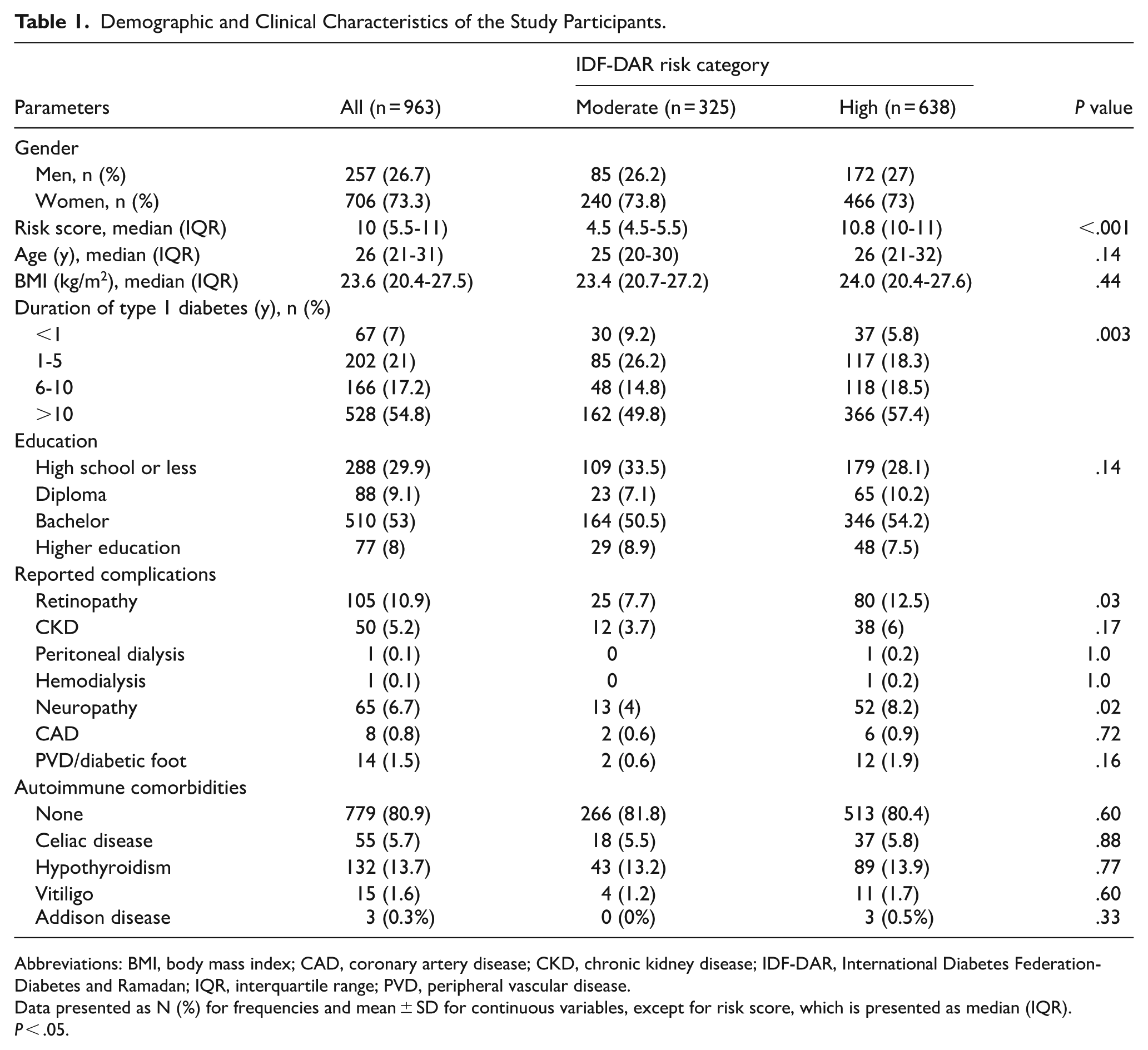
Abbreviations: BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; IDF-DAR, International Diabetes Federation-Diabetes and Ramadan; IQR, interquartile range; PVD, peripheral vascular disease.
Data presented as N (%) for frequencies and mean ± SD for continuous variables, except for risk score, which is presented as median (IQR).
P < .05.
Table 2 presents between-group differences in outcomes related to Ramadan fasting. Compared to the moderate-risk group, the high-risk group exhibited a significantly higher prevalence of choosing not to fast (24% vs 16.3%; P = .02). Breaking the fast was also significantly more common in the high-risk group compared to the moderate-risk group (P < .001; Figure 1), while the moderate-risk group was more likely to successfully fast for more days (P = .002). Compared to moderate-risk respondents, high-risk respondents were significantly more likely to be absent from school/work due to diabetes-related issues (P = .008), to be diagnosed with DKA (P < .001), and to visit the ER during Ramadan (P < .001; Table 2).
Outcomes Related to Ramadan Fasting Management in Respondents With Type 1 Diabetes.

Abbreviations: DKA, diabetic ketoacidosis; ER, emergency room.
Data presented as N (%) for frequencies and superscript (a) as median (range).
P < .05.

Distribution (%) of the number of days of breaking fasting (0, 1-2, 2-4, or >4 days) in the moderate-risk and high-risk groups.
Figure 2 presents the differences in T1D management among groups, showing that participants in the high-risk group were more commonly advised not to fast, compared to those in the moderate-risk group (P < .001). However, the majority of the high-risk group (61.1%) reported that their HCP did not advise them to abstain from fasting. Compared to those in the high-risk group, PwT1D in the moderate-risk category reported significantly greater frequencies of participating in an educational session within the last 12 months (P < .009), visiting a dietician (P < .001), and being contacted by their HCP regarding insulin changes (P < .001). Additionally, participants in the moderate-risk group were more likely to practice carbohydrate counting (56.9% vs 46.6%; P = .003; Figure 3). With regards to treatment modality, insulin pumps were used by more respondents in the moderate risk group (27.4% vs 19.1%; P = .004). The risk groups did not differ with respect to sensor-based monitoring use, changes in insulin dose, or fasting during Shawwal (Figure 3).

Differences in T1D management between the moderate-risk and high-risk groups.

Differences in Ramadan practices between the moderate-risk and high-risk groups.
Multinomial logistic regression analysis revealed that breaking the fast was significantly associated with several risk factors, including longer duration of T1D, use of intermittent-scan continuous glucose monitoring (IS-CGM), having T1D complications, and first time fasting during Ramadan (P < .01; Table 3). In parallel, breaking the fast showed significant inverse associations with older age, male gender, use of insulin injections, previous glycated hemoglobin (HbA1c) levels of >9% or being unaware of their previous levels, and being contacted by the HCP team (P < .01). In other words, PwT1D with these factors were significantly less likely to break fasting days.
Risk Factors Associated With Breaking Fast.

Abbreviations: CI, confidence interval; HbA1c, glycated hemoglobin; HCP, healthcare practitioner; IS-CGM, intermittent-scan continuous glucose monitoring; SE, standard error; T1D, type 1 diabetes.
P < .05.
Unadjusted risk estimates revealed that participants were significantly more likely to visit the ER due to glucose imbalance if their last HbA1c level was >9% (P = .04) or was unknown (P = .003). On the other hand, attending a pre-Ramadan education session was associated with 47% lower odds of visiting the ER during Ramadan (odds ratio 0.53; 95% confidence interval 0.34-0.82; P = .005; Table 4). The other analyzed risk factors were not associated with ER visits (Table 4).
Risk Factors Associated With Visiting the Emergency Room Due to Glucose Imbalance.

Abbreviations: CI, confidence interval; HCP, healthcare practitioner.
P < .05.
Discussion
In the present study, we aimed to assess the latest IDF-DAR 2021 guidelines for risk stratification in a real-life setting, among PwT1D planning to fast for Ramadan in Saudi Arabia. This cohort included a high prevalence of high-risk patients, who were more likely to suffer from complications and frequent ER visits while fasting. Interestingly, the moderate-risk group was more likely to be counseled by the HCP team for insulin dose changes. This finding may suggest that the moderate-risk group was more pro-active in terms of compliance, as evidenced by their higher attendance to education sessions and overall better outcomes during Ramadan fasting, and/or may reflect that the increased education and communication between PWT1D and HCP resulted in these patients being in the moderate-risk group. To our knowledge, this study is the largest of its kind to implement and validate the latest IDF-DAR 2021 guidelines among PwT1D.
The IDF-DAR guidelines classify people with diabetes into low-risk, moderate-risk, and high-risk categories based on multiple risk factors, including diabetes type and duration, presence of hypoglycemia, level of glycemic control (HbA1c level), type of treatment, self-monitoring of blood glucose (SMBG), presence of acute complications, and other detailed risk elements. 7 Our study only included PwT1D, and all participants were categorized as either moderate-risk or high-risk patients according to IDF-DAR classification. High-risk PwT1D were significantly more likely to break their fasting due to hypoglycemia, which supports their risk level assignment. Notably, several studies have reported that most high-risk people with diabetes opt to fast, despite the recommendations not to, emphasizing the need for this issue to be better addressed through such guidelines combined with pre-Ramadan education programs.17,18
In our study, the moderate-risk PwT1D were more likely to visit education clinics and to practice carbohydrate counting, and these habits may contribute to them being at a moderate risk level. Unfortunately, a lower percentage of high-risk PwT1D had access to the education programs. The IDF-DAR guidelines strongly emphasize the fundamental role of pre-Ramadan education programs for PwT1D, and this is further supported by several studies in the medical literature, which have reported less complications after proper education programs.19 -21 A recent systematic review probed the safety of Ramadan fasting among high-risk people with diabetes, and reported that notable benefits are associated with the implementation of existing guidelines, particularly a significant reduction of the risk of hospitalization during the Ramadan period. 22 However, must be noted that the guidelines lack robust support from strong evidence, as they have been primarily derived from observational studies. As efforts to evaluate these guidelines in real-life settings, several studies have been conducted among people with type 2 diabetes (T2D), and have reported that the guidelines were deemed reliable.
Our present results revealed an inverse relationship between glycemic control and the ability to fast, with PwT1D exhibiting higher HbA1c levels being able to complete more fasting days. One explanation could be that patients with poor glycemic control pay less attention to their disease, and thus may fast regardless of the contraindications and safety considerations. A recent study reported slightly different results, showing that PwT1D (n = 50) with HbA1c levels of ⩽8.5% were able to perform fasting for a greater number of days and suffered significantly fewer episodes of hypoglycemia. 22 A proper comparison is limited by the use of different cut-off levels, and their previous findings can only be considered suggestive due to the small sample size. Further investigations in different settings are needed to better understand this topic.
The National Institute of Clinical Excellence (NICE), ADA, and the European Association for the Study of Diabetes (EASD) recommend that CSII regimens are generally a favorable way to treat PwT1D.23,24 A recent systematic review and meta-analysis also concluded that CSII regimens are associated with lower rates of severe hypoglycemia, hyperglycemia, and ketosis during fasting. 25 Similarly, we found that the use of insulin pumps was associated with a significantly decreased number of breaks from fasting. Thus, we suggest that high-risk PwT1D should probably have greater access to this technology, to increase their likelihood of more successful fasting days. However, a recent meta-analysis reported contradictory results of using insulin pumps during Ramadan, with no significant difference in glycemic control. 26
Regarding gender-related differences, a systematic review published in 2021 investigated the impact of Ramadan fasting on hypoglycemic events, and reported that females were significantly more prone to hypoglycemia than males. Our present findings support this conclusion, as the females were more likely to break their fasting due to glycemic disturbances. However, a newly published study included 1045 people with diabetes, and reported that males are more likely to develop major hypoglycemia. These contradictory findings warrant additional larger studies to investigate this aspect.27,28
We hypothesized that the type of glucose monitoring used might play an important role in achieving optimal glucose control, among PwT1D observing Ramadan. It seemed likely that the use of CGM could facilitate fasting by empowering patients to better manage their glucose levels and complete the fast. Surprisingly, our analysis revealed that IS-CGM use was associated with a significant increase in the number of fast-breaking days. In contrast, another recent study demonstrated positive outcomes with the use of IS-CGM, reporting significantly reduced HbA1c levels without concurrent hypoglycemia episodes in patients using FreeStyle Libre. 29 Similarly, a local study highlighted the usefulness of IS-CGM for assisting PwT1D in fasting safely without encountering severe hypoglycemia. 30
Our present study had several limitations. The reliance on self-reported data could introduce recall bias, and subjective interpretation is intrinsic to survey-based studies. Additionally, the use of purposive sampling via online platforms can introduce potential selection bias, leading to overrepresentation of participants with better access to technology. Another limitation is that our findings were based only on inputs from PwT1D; therefore, the gaps identified in patient management must be confirmed by investigating HCPs’ awareness and knowledge of the existing IDF-DAR guidelines. Our cohort exhibited a high prevalence of high-risk PwT1D, but this risk was calculated without using all 14 risk factors identified in the guidelines; thus, the actual scores may be higher in the high-risk group. However, we intentionally omitted some risk factors for practical reasons. Since the presence of T1D alone is assigned 1.0 point, none of the respondents could have a score of 0. Furthermore, any PwT1D treated with multiple daily injection (MDI) or insulin pump (2.5 points) is automatically categorized in the moderate-risk group independent of glycemic control. The architects of the IDF-DAR guidelines could consider these issues in forthcoming updates. A final limitation is the lack of formal validation beyond expert committee review; however, the simplicity of the questions and the alignment with existing guidelines 7 are considered strengths that mitigate potential biases.
Despite these limitations, the present study is the first to assess the validity and outcomes of the IDF-DAR 2021 guidelines among PwT1D in the Middle-Eastern region. Other strengths of this study are the large sample size and kingdom-wide scope, which make the findings generalizable. This study contributes to the field by validating a globally recommended risk tool in a specific population, consequently providing novel data about risk distribution and providing real-world evidence regarding fasting experience, with actionable insights into how educational interventions impact health outcomes during religious fasting.
Conclusion
In conclusion, our results support the reliability of the IDF-DAR 2021 guidelines, offering valuable assistance to physicians in their clinical decision-making for PwT1D who fast during Ramadan. Notably, patients classified as high-risk according to the IDF-DAR stratification should be targeted to receive increased Ramadan-specific education and diet consultation, since the findings suggest a gap in counseling this vulnerable group. Future prospective cohort studies should be designed to include HCP knowledge and adherence to IDF-DAR guidelines, to identify barriers to implementation and better evaluate the impact of education and technology on fasting outcomes. Finally, the IDF-DAR guidelines could be improved by updates that include advancements in diabetes technology, such as insulin pumps and CGM.
Supplemental Material
sj-docx-1-end-10.1177_11795514251376888 – Supplemental material for Assessment of the IDF-DAR Fasting Risk Assessment Tool to Predict Type 1 Diabetes-Related Complications During Ramadan in a Real-World Setting
Supplemental material, sj-docx-1-end-10.1177_11795514251376888 for Assessment of the IDF-DAR Fasting Risk Assessment Tool to Predict Type 1 Diabetes-Related Complications During Ramadan in a Real-World Setting by Abdullah M. Alguwaihes, Mohamed Hassanein, Naweed Alzaman, Mohammed E. Al-Sofiani and Metib Alotaibi in Clinical Medicine Insights: Endocrinology and Diabetes
Supplemental Material
sj-docx-3-end-10.1177_11795514251376888 – Supplemental material for Assessment of the IDF-DAR Fasting Risk Assessment Tool to Predict Type 1 Diabetes-Related Complications During Ramadan in a Real-World Setting
Supplemental material, sj-docx-3-end-10.1177_11795514251376888 for Assessment of the IDF-DAR Fasting Risk Assessment Tool to Predict Type 1 Diabetes-Related Complications During Ramadan in a Real-World Setting by Abdullah M. Alguwaihes, Mohamed Hassanein, Naweed Alzaman, Mohammed E. Al-Sofiani and Metib Alotaibi in Clinical Medicine Insights: Endocrinology and Diabetes
Supplemental Material
sj-jpg-2-end-10.1177_11795514251376888 – Supplemental material for Assessment of the IDF-DAR Fasting Risk Assessment Tool to Predict Type 1 Diabetes-Related Complications During Ramadan in a Real-World Setting
Supplemental material, sj-jpg-2-end-10.1177_11795514251376888 for Assessment of the IDF-DAR Fasting Risk Assessment Tool to Predict Type 1 Diabetes-Related Complications During Ramadan in a Real-World Setting by Abdullah M. Alguwaihes, Mohamed Hassanein, Naweed Alzaman, Mohammed E. Al-Sofiani and Metib Alotaibi in Clinical Medicine Insights: Endocrinology and Diabetes
Footnotes
Acknowledgements
The authors are thankful to all the respondents who participated in the survey. A portion of the results was presented as an oral abstract presentation during the AACE 2024 MENA Meeting held in Dubai on November 22 to 24, 2024.
Ethical Considerations
The study protocol and procedures conformed to international ethical guidelines, and the study was approved by the Institutional Review Board of the College of Medicine, King Saud University, Riyadh, Saudi Arabia (Approval no: E-21-5928, May 27, 2021).
Consent to Participate
All participants provided written informed consent prior to participating.
Consent for Publication
All participants provided written informed consent prior for publication.
Author Contributions
A.M.A. conceptualization; data curation; formal analysis; investigation; methodology; project administration; resources; supervision; visualization; writing—original draft; writing—review and editing. M.H. investigation; validation; writing—review and editing. N.A. conceptualization; data curation; investigation; writing—review and editing. M.E.A. data curation; methodology; writing—review and editing. M.A. data curation; investigation; project administration; writing—original draft; writing—review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.M.A. has served on advisory panels for Medtronic, Novo Nordisk, Eli Lilly, Vital Air, and Sanofi; has received honoraria for speaking from AstraZeneca, Eli Lilly, Medtronic, Novo Nordisk, and Sanofi; and received research support from AstraZeneca and Novo Nordisk. M.A. has served on advisory panels for Eli Lilly and Algorithm; has received honoraria for speaking from Eli Lilly, Novo Nordisk, Boehringer Ingelheim, and Sanofi; and received research support from Novo Nordisk. M.E.A. has served on advisory panels for Medtronic, Insulet, Abbott, VitalAire, and Sanofi; and has received honoraria for speaking from Abbott, Eli Lilly, Medtronic, Novo Nordisk, Sanofi, and VitalAire. The other authors declare no conflict of interest.
Data Availability Statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.