
Abstract
Background:
Diabetic ketoacidosis (DKA) is a rare but serious complication that can develop during pregnancy, with up to 30% of patients presenting with euglycemia, making prompt recognition challenging. It is associated with increased perinatal mortality rates, although the exact risk of maternal mortality remains unclear. The purpose of this systematic review was to examine the available literature and provide an overview of reported cases of DKA during pregnancy.
Methods:
PubMed, Web of Science and Scopus library databases were screened from inception until January 2024. Included studies provided data on classic or euglycemic DKA during pregnancy. All study designs were considered eligible for inclusion.
Results:
We identified 66 eligible articles, which included 57 case reports and case series with individual patient data, and 9 studies without individual patient data. The mean age at diagnosis was 28.8 years, and the average gestational age at diagnosis was 29.5 weeks. The majority of women had type 1 diabetes mellitus (T1DM) (45.9%), followed by gestational diabetes (GDM) (40.5%). Most cases were classified as classic DKA (70.3%), with nearly one-third developing euglycemic DKA (29.7%). The most common trigger factors were infections (28%), followed by poor adherence to treatment (13.5%). The most frequent symptoms included nausea (32.4%), vomiting (32.4%), osmotic symptoms (21.6%), and abdominal pain (20.2%). All cases were treated with intravenous insulin and fluids. The vast majority (98.9%) of women eventually fully recovered, with only 1 reported death due to organ failure (1.3%). Intrauterine death or stillbirth occurred in one-third of cases (35.2%), including 1 instance of a twin pregnancy.
Conclusions:
DKA is a condition that clinicians may encounter during pregnancy. Although rare, increased awareness and early recognition are crucial for optimal management and improved maternal and neonatal outcomes.
Understanding Diabetic Ketoacidosis (DKA) in Pregnancy: Causes, Risks, and the Importance of Early Treatment
Diabetic ketoacidosis (DKA) is a serious health issue that can affect pregnant women with diabetes. It happens when the body cannot use sugar properly because there isn’t enough insulin. As a result, the body breaks down fat for energy, which produces harmful substances called ketones. These ketones can build up and cause dangerous complications for both the mother and her baby. While DKA isn’t common, it can be life-threatening if not treated quickly.
This study looked at 66 reports about DKA in pregnancy to better understand how often it happens, what causes it, how it is treated, and what effects it has on the mother and baby. The study found that DKA mostly occurs in women with certain types of diabetes (type 1 or gestational diabetes) and typically happens later in pregnancy, especially during the third trimester.
The main reasons for DKA during pregnancy include infections, not following diabetes treatment properly, and taking certain medications like steroids. Common signs of DKA include feeling nauseous, vomiting, feeling very thirsty, needing to urinate often, and stomach pain. Most of the women in the study recovered after receiving treatment, which usually involved giving insulin and fluids through a drip. However, DKA was associated with a high rate of stillbirth, affecting about one-third of pregnancies.
This study highlights how important it is to recognise and treat DKA early during pregnancy. It also shows the need for doctors to closely monitor pregnant women with diabetes, especially if they are sick or on certain medications. Early action can help prevent serious complications and improve the chances of a healthy outcome for both mother and baby.
Introduction
Diabetic ketoacidosis (DKA) is the most common emergency associated with diabetes. It is characterised by metabolic acidosis (bicarbonate concentration ⩽ 18.0 mmol/l and/or venous pH ⩽ 7.3), capillary or blood ketone concentration ⩾ 3.0 mmol/l or significant ketonuria (2+ or more on standard urine sticks) and in the classic presentation, a blood glucose concentration of 11.1 mmol/l or higher, versus normal plasma glucose or a milder hyperglycaemia (11-14 mmol/l) in the euglycemic DKA (EDKA).1,2 Pathophysiologically, the core of DKA is increased gluconeogenesis and glycogenolysis along with reduced glucose oxidation resulting from decreased glucose uptake by the peripheral tissues. These all lead to hyperglycaemia and subsequently osmotic diuresis and dehydration; furthermore, the increased free fatty acids are oxidised into ketone bodies in the liver resulting in a high anion gap metabolic acidosis.
The metabolic changes during pregnancy can lead to the rapid development of DKA even with relatively mild hyperglycaemia, although the exact mechanisms are not entirely understood. 3 Despite this, DKA is rare in pregnancy, with an estimated incidence of 0.5% to 3%. 4 Up to 30% of cases are euglycemic, making prompt recognition more challenging. 5 Although DKA is not commonly life threatening to the pregnant woman if it is recognised and treated promptly, the exact risk of maternal mortality secondary to complications associated with DKA is not well established. 6 Perinatal mortality rates, on the other hand, remain as high as 35% for a single episode of DKA despite substantial improvements in perinatal and neonatal care. 3 Therefore, raised awareness is required for an immediate diagnosis and management.
The purpose of this systematic review is to examine the available literature, provide an overview of the reported cases of DKA in pregnancy and elaborate on the diagnosis, management and associated outcomes.
Methods
This review was reported based on the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ (PRISMA) guidelines. 7
Literature search
Two reviewers (DS, KKT) searched the PubMed, Web of Science and Scopus library databases from inception until January 2024. The search included the following terms: (diabetic ketoacidosis OR DKA OR diabetic acidosis OR Diabetic ketosis) AND (pregnancy OR gestation). There were no restrictions regarding study design or geographic region. A manual search of references cited in the selected articles was also conducted for undetected studies. Discrepancies in the literature search process were resolved by a third investigator (KSK).
Eligibility criteria
Included studies provided data on classic or EDKA during pregnancy. All study designs were considered eligible for inclusion. Only articles with full text in English language were included. Cases on the immediate postpartum period were excluded. Review articles, abstracts submitted in conferences and non-peer reviewed sources were also considered ineligible for inclusion.
Data extraction and handling
In all articles, patient data was collected and handled by 3 authors (DS, FNL, MD) who conducted the data extraction independently. The following information was collected: article type, year, type of diabetes, age, ethnicity, parity, week of gestation, type of DKA (classic or euglycemic), medical history, regular medications, trigger factors, presenting symptoms, laboratory results, treatment, maternal outcomes, foetal outcomes including preterm delivery, growth and presence of oligohydramnios, mode of delivery (spontaneous vaginal birth, operative vaginal delivery, emergency or elective caesarean section) and type of labour (spontaneous or induced). Any disagreements were discussed and resolved by a fourth author (KSK).
Quality assessment
The risk of bias (RoB) for studies with individual patient data (case reports and series) was independently assessed by 2 authors (KSK and KKT). To evaluate the overall quality of these studies, the critical appraisal checklist provided by the Joanna Briggs Institute (JBI) was employed. The assessment was based on the reporting of 8 elements: patient demographics, medical history, health status, physical examination and diagnosis, concomitant therapies, post-intervention health status, drug administration, and reaction interface. Each element was scored as ‘Yes’, ‘No’, ‘Unclear’ or ‘Not Applicable’, depending on the availability of information. 8
For studies without individual patient data (observational studies), the risk of bias was assessed using the Methodological Index for Non-Randomised Studies (MINORS). MINORS is a validated tool designed to evaluate the methodological quality of non-randomised studies, whether comparative or non-comparative. Each domain within MINORS is scored as 0 if not reported, 1 if reported with inadequate details, and 2 if adequately reported. The global ideal score is 16 for non-comparative studies. Studies with MINORS scores < 6 were considered to have a high risk of bias, while those with scores between 6 and 9 were considered to have a moderate risk of bias. 9
Data synthesis
We used descriptive statistics to describe the demographics and clinical characteristics of the included patients. Means for continuous variables and frequencies and percentages for binary variables were used. We reported duration of symptoms in days due to inconsistent reporting of this information in the included articles.
Results
Literature search and study characteristics
The initial literature search yielded 931 publications. In the first screening 490 studies were excluded as irrelevant. After the exclusion phase, 126 full texts were screened and 66 studies were found eligible for the systematic review (Figure 1).4,10 -65 Of the studies 20 were conducted in Asia, 20 in Americas, 15 in Europe, 1 in Africa and 1 in Oceania. Regarding study design, 9 studies were case series comprising at least 3 cases each without individual patient data, and 57 were case reports and case series with individual patient data (Tables 1 and 2).
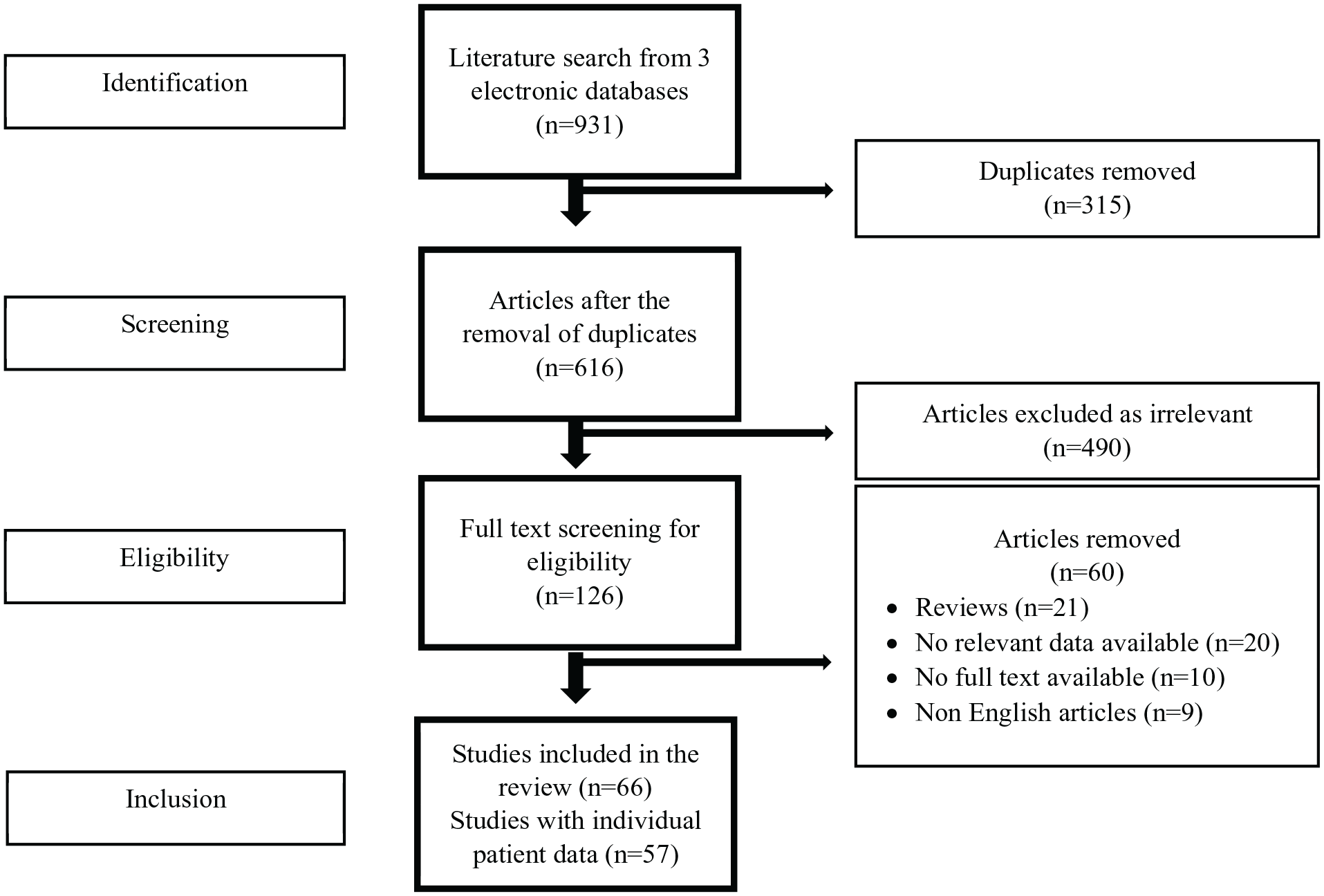
PRISMA flowchart.
Characteristics of the included studies (studies with individual patient data).

Characteristics of the included studies (studies without individual patient data).

Studies with individual patient data (case reports and case series)
In our review of case reports and case series with individual patient data, we identified a total of 74 cases of DKA during pregnancy. Among these, 1 patient experienced a recurrence of DKA during the same pregnancy, and 2 patients had recurrences during subsequent pregnancies.
Mean age at diagnosis was 28.8 years and average time of gestation at diagnosis was 29.5 weeks. The majority of women had type 1 diabetes (T1DM) (45.9%; 34/74) and a fraction had fulminant T1DM (12.1%, 9/74). The second commonest type of diabetes was GDM (40.5%, 30/74). The remaining cases were type 2 diabetes (T2DM) (9.5%, 7/74), late onset diabetes (1.4%, 1/74), while in 2 cases the type was not specified and was reported as insulin dependent diabetes (2.7%, 2/74). The majority had classic DKA (70.3%, 52/74) and almost one-third of cases developed EDKA (29.7%, 22/74). In the GDM group, 40% (12/30) had EDKA and the remaining 60% (18/30) classic DKA. Parity was reported for 53 cases ranging from first to ninth pregnancy. Ethnicity data were available in 44 cases of whom 40.9% were Asian (18/44), 29.5% Caucasian (13/44), 20.8% African (9/44), 4.6% Latin American (2/44) and 4.6% Middle Eastern (2/44).
Most common trigger factor included infection (28%, 21/74), followed by poor adherence to treatment (13.5%, 10/74), treatment with steroids (12.1%, 9/74), new diagnosis (5%, 4/74), pump failure (4%, 3/74), hyperemesis (2.7%, 2/74), reduced carb intake (2.7%, 2/74), dehydration/long haul travel (1.3%, 1/74), pre-eclampsia (1.3%, 1/74) and labour (1.3%, 1/74). In almost one-third of the cases (29%, 20/74), a trigger factor was not identified or reported.
The most reported symptoms were nausea (32.4%, 24/74) and vomiting (32.4%, 24/74), osmotic symptoms (21.6%, 16/74), abdominal pain (20.2%, 15/74), shortness of breath (18.9%, 14/74) and fatigue (9.4%, 7/74). Intravenous insulin and fluids were used in all cases.
The vast majority (98.9%, 73/74) eventually fully recovered. Two women required mechanical ventilation (2.7%, 2/74) and 1 patient was on non-invasive ventilation (1.3%, 1/74). Death following acute respiratory distress syndrome and organ failure was reported in 1 case (1.3%, 1/74). Four patients had concurrent pre-eclampsia (5.4%, 4/74). One patient had a total hysterectomy due to stitch and tubo-ovarian abscess (1.3%, 1/74). Data on mode of delivery was available in 60 cases; vaginal birth was the most common (38.4%, 28/74) followed by emergency caesarean section (17.8%, 13/74), elective caesarean section (8.2%, 6/74) and operative vaginal birth (1.4%, 1/74). Induction of labour was also used in a small number of cases (16.4%, 12/74).
Data on neonatal outcomes were available for 71 cases. Intrauterine death / stillbirth was reported in one-third of cases (35.2%, 25/71) of whom one was a twin pregnancy. Mean gestational age when foetal death occurred was 30 weeks. Termination of pregnancy was decided in 1 case (1.4%, 1/74). Information on the gestational age at delivery was reported in 58 cases with the majority of patients delivering preterm (63.7%, 37/58) and the remaining delivering at term (36.2%, 21/58). Data on foetal growth was available in 46 cases of whom 6 babies were large for gestational age (13%, 6/46). Data on foetal glucose readings was not consistently provided. Information on amniotic fluid volume was provided in 26 cases of whom 5 (19.2%, 5/26) had polyhydramnios.
Studies without individual patient data (case series and observational studies)
We identified 9 case series without individual patient data.3,66 -73 Schneider et al reported 4 cases of DKA on the background of GDM with mean gestational age at 29 + 1 weeks. The most common precipitating factor was infection. There were no maternal deaths, but 1 foetal demise was reported. Cullen et al reported 11 cases with pre-existing type 1 or 2 diabetes with 1 foetal demise and 4 macrosomic infants. Similarly, Kilvert et al published 10 cases, of which 9 had pre-existing diabetes and 1 pre-diabetes; 6 of the 8 patients treated with insulin at the time of the ketoacidosis had 7 further episodes of ketoacidosis and at least 11 admissions for severe hyperglycaemia either before or after DKA. There were 2 foetal deaths. Dhanasekaran et al reported 71 cases, 48 with T1DM (82.8%) and 23 with T2DM (17.2%); foetal demise occurred in 10 pregnancies (6 miscarriages and 4 stillbirths) and macrosomic infants in 16 cases (33.3%).
In a case series with fulminant diabetes, foetal demise occurred in 21 out of the 23 cases (91.3%) (Liu et al). No maternal or foetal deaths were reported by Bryant et al whose cohort consisted of 33 women with the majority (67%) having T1DM. On the other hand, Maseko et al reported 56 cases with 30.6% stillbirth rate. Guo et al identified 8 DKA events out of 90 patients with GDM/overt diabetes with 2 stillbirths and 1 spontaneous abortion. Finally, Montero et al reported high frequency of foetal death in 35% of the cohort which consisted of 20 women with T1DM.
Quality of the studies
Regarding case reports and series quality assessment revealed that most studies were graded either as of good or moderate quality. Details on demographic characteristics and interventions of the included cases was not sufficiently reported in 20 and 18 articles respectively. Only 1 study did attain a perfect score (Table S1).
Among studies without individual patient data, only 1 study was considered to have a high risk of bias. The rest were either low risk of bias (4/9) or medium risk of bias (4/9). The most frequently missing information was the prospective sample size calculation, which was absent in all studies (0/9) (Table S2).
Discussion
In this systematic review, 74 cases of DKA during pregnancy were identified, predominantly in women with GDM or T1DM, most frequently occurring during the third trimester. Typical symptoms included nausea, vomiting, and osmotic symptoms (polyuria, polydipsia) preceding the onset of DKA. Although classic DKA with hyperglycaemia was the most common presentation, almost 30% of cases were EDKA, requiring high clinical suspicion for prompt diagnosis and management. EDKA was common in patients with gestational diabetes (40%). All but 1 woman fully recovered. However, 25.6% of the cases were associated with foetal demise. Trigger factors included infections (with several cases published during the COVID-19 pandemic), poor adherence to insulin therapy, and the use of steroids for lung maturation.
Results in the context of the literature
With the ultimate goal of providing adequate nutrition to the foetus, insulin resistance increases during pregnancy due to rising hormones such as progesterone, peaking during the second and third trimesters. As resistance increases with gestational age, insulin production is enhanced to compensate for the higher requirements. This is achieved through pancreatic beta cell hyperplasia. Additionally, a relative state of starvation and hypoglycaemia characterises pregnancy, leading to increased lipolysis and subsequent ketogenesis, which further supports the nutritional needs of the foetus. 74 On the background of a precipitating factor such as an infection, decompensation and subsequent diabetic ketoacidosis might occur. 75 Therefore, pregnancy is a ketogenic state that can progress to diabetic ketoacidosis when a trigger factor enhances ketogenesis against a background of relative insulin deficiency.76,77 It is worth noting that since respiratory alkalosis is also seen in pregnancy, baseline bicarbonate levels are already lower due to compensation. The above also explain why DKA most commonly presents in late pregnancy; This was also evident in our study with most reported cases presenting in women during the third trimester. However, since it can still occur early in pregnancy, it’s important to maintain a low threshold for ketone testing when women present with relevant symptoms even in the absence of previous diagnosis of diabetes. 24
EDKA presents more frequently during pregnancy due to increased expression of placental glucose transporters, which aim to provide nutrition to the foetal-placental unit and lead to lower blood glucose levels. Interestingly, these receptors are higher in people treated with insulin. Moreover, increased plasma volume is seen in pregnancy leading to haemodilution and therefore normal blood glucose levels. EDKA is equally detrimental as classic DKA in pregnancy and can result in cardiac arrhythmias secondary to electrolyte imbalances, 20 myocardial infarction, and cardiogenic shock secondary to acidosis requiring ITU admission. There is a higher risk of recurrent decelerations, foetal hypoxia and mortality before and during delivery of the foetus. Ketones can also cross the placental barrier causing intellectual disability, encephalomalacia, cleft lip, cleft palate, and neural tube defects. 78 As there is an inverse relationship between maternal ketone levels and peripartum/neonatal outcomes, early diagnosis and treatment of classic and EDKA is crucial. It’s worth noting that in some cases, recurrent episodes of DKA were reported during the same or subsequent pregnancies. Multiple episodes of DKA during pregnancy pose a high risk to the foetus and increase the chances of foetal complications and demise.79 -81 Causes of recurrent DKA include omission of insulin and poor adherence to treatment. 82 Therefore, patients after the first DKA episode require increased attention.
A notable observation is that the most frequently reported ethnic background in our study was Asian, which is partly explained by the existing data on a higher prevalence of GDM in women of South Asian and South East Asian decent compared to Caucasian, African-American and Hispanic. 83 Another important observation is the high percentage of women with GDM. Previous studies conducted in 2019 to 2022, such as a case-control study in the United Kingdom, have indicated that the majority of DKA cases occurred in individuals with T1DM, while GDM was still recognised as a risk factor. However, the high percentage of GDM cases in our study suggests that the population is changing and this is likely due to the increasing prevalence of obesity linked to insulin resistance. 84 Therefore, this emergency condition can be expected in women regardless of the underlying type of diabetes.24,79 Another interesting finding is the frequency of macrosomia which was 13% based on the available information for 46 cases and is consistent with the reported worldwide prevalence.
Strengths and limitations
Our study constitutes the first systematic review providing an overview of the cases of DKA during pregnancy. This research provides a detailed synthesis of existing literature, incorporating quality assessment of the included studies. Despite the comprehensive nature of our review, it is imperative to acknowledge several inherent limitations. A primary limitation arises from the inclusion of low-quality case reports and case series, which may compromise the validity and generalisability of our conclusions. These types of studies are prone to biases, such as overinterpretation and selection bias, potentially skewing the results. Therefore, while the findings reported herein are noteworthy, they may not fully capture the variety associated with DKA during pregnancy regarding presentation, management and outcomes. To establish a stronger body of evidence, further insights are required ideally from prospectively design studies.
Conclusion
In this systematic review, DKA during pregnancy most commonly presented in women with T1DM or GDM. It was often triggered by infections, suboptimal adherence to treatment, and steroid administration. DKA can be life-threatening for the mother and can also lead to foetal demise which occurred in around one-fourth of the cases in this cohort. These findings underscore the necessity for clinicians to consider the possibility of DKA in any deteriorating pregnant woman. Early recognition, immediate hospitalisation and aggressive treatment remain the mainstay of DKA management.
It is important to recognise that pregnancy induces a diabetogenic state to facilitate the delivery of glucose to the foetus, ensuring proper growth. DKA during pregnancy is not exclusive to T1DM but also affects women with GDM and T2DM. Ongoing patient education on sick day rules and the importance of adherence to insulin therapy, increased awareness among both patients and clinicians, and careful glucose monitoring during steroid administration are all crucial in preventing, or at the very least effectively managing, diabetic emergencies during pregnancy. This approach is essential to reducing adverse outcomes associated with DKA.
Supplemental Material
sj-docx-1-end-10.1177_11795514241312849 – Supplemental material for Diabetic Ketoacidosis in Pregnancy: A Systematic Review of the Reported Cases
Supplemental material, sj-docx-1-end-10.1177_11795514241312849 for Diabetic Ketoacidosis in Pregnancy: A Systematic Review of the Reported Cases by Dimitra Stathi, Florence Ning Lee, Mili Dhar, Stergios Bobotis, Elisavet Arsenaki, Taruna Agrawal, Konstantinos Katsikas Triantafyllidis and Konstantinos S Kechagias in Clinical Medicine Insights: Endocrinology and Diabetes
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.