
Abstract
Background:
Pre-diabetes, characterized by elevated glycemic indices, poses a high risk of diabetes development, and is increasingly linked to non-specific low back pain. While mechanisms remain incompletely understood, metabolic, inflammatory, and neurological factors are implicated. Dietary interventions, including low-glycemic and anti-inflammatory diets, alongside weight management, may improve outcomes in this population.
Objectives:
In this non-randomized controlled trial, we aim to evaluate the influence of decreasing HbA1c levels on reducing chronic non-specific low back pain in pre-diabetic, non-obese individuals, as well as emphasizing the importance of such a study in supporting the literature.
Methods:
A non-randomized controlled single-blind clinical trial was conducted among 82 participants with chronic non-specific low back pain and pre-diabetes at an outpatient clinic in Baghdad from the 30th of January to the 22nd of September. The intervention methods aimed at reducing HbA1c levels to assess the reduction impact on alleviating chronic non-specific low back pain included dietary adjustments, sleep optimization, and correction of vitamins and minerals deficiencies. The follow-up process was conducted individually for each participant, with a monthly assessment over a period of six months.
Results:
At 12 weeks a significant decrease in chronic non-specific low back pain severity was observed in patients with lower HbA1C levels yielding a P-value of .021. Similarly, at 24 weeks there was a decline in the number of patients who reported chronic non-specific low back pain, and the association to lower HbA1C levels was significant with a p-value of .005.
Conclusion:
This study suggests the presence of a statistically significant association between reduction of HbA1C levels and ensuing improvement in chronic non-specific low back pain symptoms in non-obese prediabetic patients.
Plain language summary
Pre-diabetes is a condition where blood sugar levels are higher than normal but not high enough to be classified as diabetes. People with pre-diabetes are at risk of developing diabetes and other health problems, including low back pain, a type of low back pain without a clear cause. Researchers believe this link might be due to problems with metabolism, inflammation, or nerve function. Changes in diet, especially focusing on lowering blood sugar levels and reducing inflammation, along with managing weight, may help people with pre-diabetes who have low back pain without a clear cause feel better.
In this study, 82 people with both pre-diabetes and low back pain without a clear cause that lasted for more than 3 months took part in a clinical trial at a clinic in Baghdad. The trial lasted from January to September and was designed to see if lowering blood sugar (measured by HbA1c levels) would reduce low back pain. The participants received personalized care, which included making changes to their diet, improving their sleep, and correcting any vitamin or mineral deficiencies they had. They were followed closely for six months, with monthly check-ups.
The results showed that after 12 weeks, many people who managed to lower their blood sugar levels experienced less severe low back pain. The improvement was even more noticeable after 24 weeks, as fewer people reported ongoing low back pain, and this improvement was strongly linked to lower blood sugar levels.
In conclusion, the study found that reducing blood sugar levels in people with pre-diabetes who are not obese can significantly improve symptoms of low back pain. This suggests that managing blood sugar could be an important way to relieve low back pain without a clear cause.
Introduction
Non-specific low back pain is defined according to Balagué et al. as low back pain that cannot be attributed to a recognizable specific pathology, such as infection, tumour, osteoporosis, fracture, structural deformity, inflammatory disorder, radicular syndrome, or cauda equina syndrome. 1 According to the length of time that a low back pain episode lasts, published works typically classify the pain as acute, sub-acute, or chronic. Three common cutoffs are shorter than 6 weeks, 6 to 12 weeks, and longer than 12 weeks. 2 Acute low back pain becomes chronic in around 10% to 15% of patients. The chronic condition is the most difficult to manage since it takes up the majority of resources and rarely gets better over time. 3
Pre-diabetes is a hyperglycemic state characterized by glycemic indices that are higher than normal but less than the diabetes threshold. While the criteria for diagnosing pre-diabetes differ among world-wide professional associations, it presents a high risk of developing diabetes, with an annual conversion rate of 5%-1. 4 The association between pre-diabetes, diabetes, and non-specific low back pain is becoming more and more recognized. While the precise mechanisms by which these conditions are linked are still not completely understood, there is growing evidence that the interplay between metabolic variables, inflammation, and neurological processes could be involved. 5 Additionally, dietary changes, including intermittent fasting, which emphasizes glycemic control and anti-inflammatory approaches, have demonstrated potential for addressing low back pain associated with diabetes. 6
A variety of complications can arise from chronic hyperglycemia. Prolonged exposure to elevated blood glucose levels may trigger systemic inflammation, which can adversely affect the soft tissues and joints in the back. 7
Diet plays a pivotal role in glycemic control, and adopting a low-glycemic diet can be beneficial for individuals with diabetes and pre-diabetes. Low-glycemic foods are absorbed more slowly, leading to a gradual rise in blood glucose levels and reduced insulin demand. 8 The intermittent diet has the ability to boost neuronal plasticity and neurotrophic factors in the central nervous system. It has been established that a decrease in neuronal plasticity is one of the most important underlying causes of many chronic pain conditions, including neuropathic pain. Studies have shown that intermittent fasting reduces pro-inflammatory indicators, lowering inflammation. 9 This dietary approach can help manage diabetes by preventing large fluctuations in blood sugar levels, which may indirectly contribute to the alleviation of non-specific low back pain associated with the condition.
In addition to glycemic control, the anti-inflammatory aspect of diet modification is crucial in managing diabetes-related low back pain. Chronic inflammation is a common denominator in both diabetes and non-specific low back pain. 10 Certain dietary patterns, such as the Mediterranean diet, which is rich in fruits, vegetables, whole grains, and omega-3 fatty acids, have been associated with anti-inflammatory effects. These dietary components can modulate inflammatory pathways, potentially reducing inflammation in the joints and soft tissues of the back.10,11
Furthermore, pre-diabetes and low back pain treatment also require proper weight management. Weight, especially abdominal obesity, is a key diabetes risk factor. Increased mechanical stress on the spine might worsen low back pain. A balanced, calorie-controlled diet serves to help with weight management, spine pressure, and musculoskeletal health. 12
Individuals with pre-diabetes can significantly improve their overall quality of life by following a balanced diet that meets nutritional needs and ensures adequate consumption of micronutrients such as vitamin D and magnesium, as well as establishing effective weight management approaches. This comprehensive strategy tackles interrelated health issues and had the potential to have a favorable impact on outcomes linked to musculoskeletal health and low back pain. 13
In this non-randomized controlled trial, we aim to evaluate the influence of decreasing HbA1c levels on reducing chronic non-specific low back pain in pre-diabetic, non-obese individuals, as well as emphasizing the importance of such a study in supporting the literature.
Methodology and Patients
Ethics, registration and trial design
A non-randomized controlled single-blind clinical trial was conducted among 82 participants who had been diagnosed with chronic non-specific low back pain, after obtaining ethical approval from the ethical committee of the university of Warith Al-Anbiyaa / College of Medicine on 10th of January 2023. The follow-up process was conducted individually for each participant, with a monthly assessment over a period of 6 months, from the 30th of January to the 22nd of September. The study was done in the Middle East Private Hospital in Baghdad, Iraq. The CONSORT flow diagram detailing participant recruitment and study progress is provided in Figure 1.
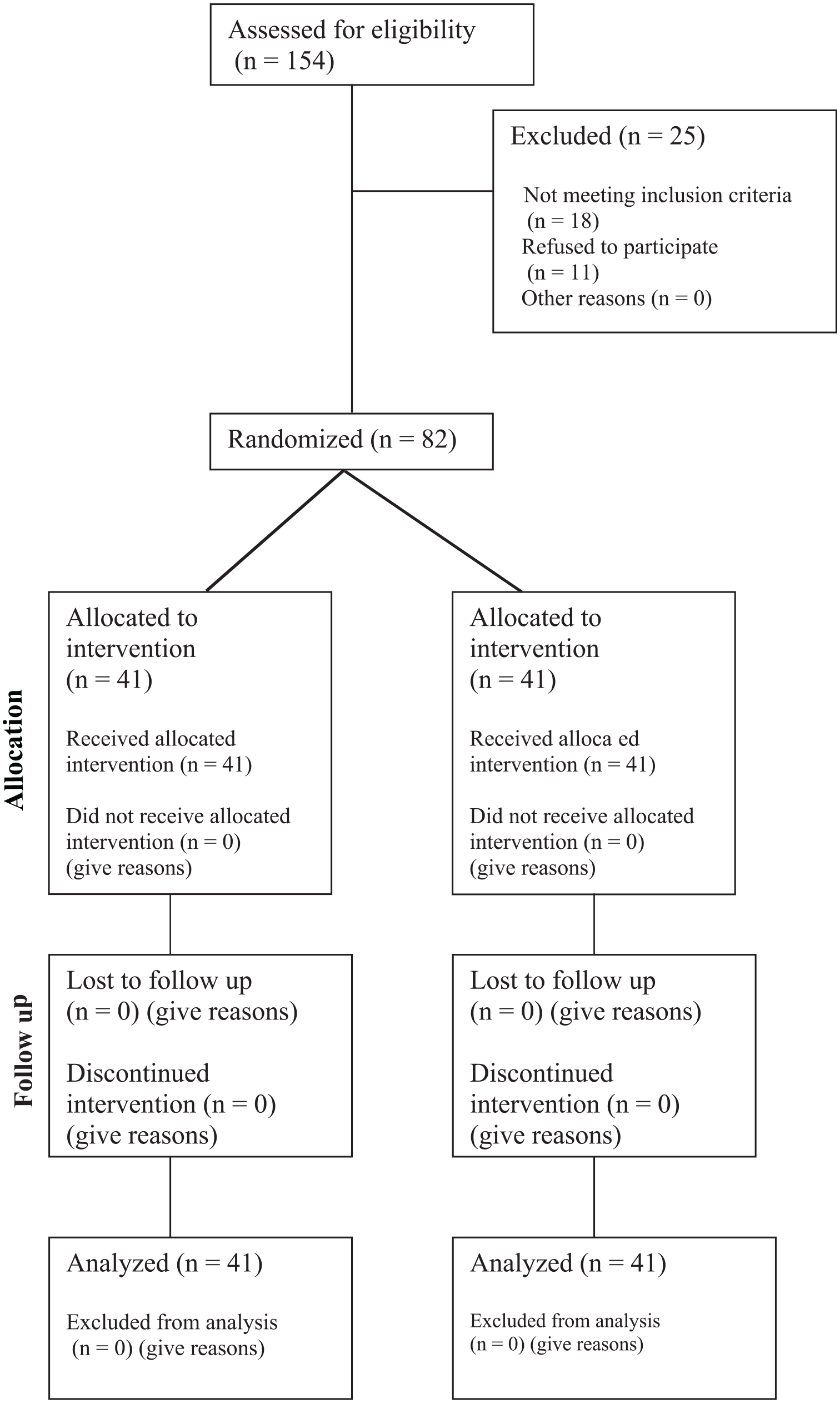
CONSORT flow diagram.
Inclusion and exclusion criteria
The inclusion criteria for participants in this clinical trial require individuals to meet several conditions. First, participants must have chronic non-specific low back pain lasting more than three months without identifiable specific causes as defined by Fleckenstein et al 14 . This is determined through a thorough evaluation involving history-taking, physical examination, and relevant investigations. Second, eligible individuals must have HbA1c levels within the range of 5.7 to 6.4, indicating a prediabetic state. Third, participants must be non-obese, with a Body Mass Index (BMI) below 30. Additionally, participants must demonstrate the ability to consistently record relevant data throughout the trial period and show a commitment to compliance with the prescribed treatment plan. This commitment will be assessed through regular follow-ups during the trial to ensure adherence to the intervention protocols and contribute to the study’s reliability.
The exclusion criteria for this clinical trial disqualify individuals with acute low back pain, defined as pain lasting less than 3 months. Participants with specific causes of low back pain, such as previous spine surgeries, spinal stenosis, peripheral vascular disease, rheumatological disease, or lumbar disc prolapse, as determined through comprehensive evaluation, will also be excluded. Individuals with HbA1c levels outside the prediabetic range—those below 5.7 or at or above 6.5—will not be included. Those taking medications that affect glycemic control, weight, or analgesics will be excluded if they are unable to discontinue these medications 2 months before the trial. The study will also exclude individuals working in occupations involving the operation of heavy machinery, such as those involved in the displacement of heavy construction equipment, truck drivers, and those engaged in cyclic lifting, due to the potential impact on low back pain outcomes. Pregnant individuals and those with multiparity will also be excluded to eliminate any influence on the study variables. Participants will be required to avoid moderate-to-intense physical activity for the duration of the study to maintain the integrity of the findings, though light activities such as walking are permitted. Those who are unable or unwilling to adhere to this restriction will be excluded. Finally, individuals who fail to comply with the prescribed treatment plan, demonstrate non-compliance during follow-up, or lose recorded data will also be disqualified from participation.
The intervention
The intervention methods aimed at reducing HbA1c levels to assess the reduction impact on alleviating chronic non-specific low back pain included dietary adjustments, sleep optimization, and correction of vitamins and minerals deficiencies.
1. Diet: The diet employed in the study adhered to the American Diabetes Association (ADA) guidelines, 15 emphasizing food choices low in saturated fat, trans fat, added sugar, and sodium. Additionally, participants were instructed to incorporate intermittent fasting through time-restricted feeding. This plan permitted a specific feeding window of 4 to 8 hours per day, with fasting periods lasting 16 to 20 hours. The integration of intermittent fasting was based on evidence from a meta-analysis conducted by Borgundvaag et al 16 which demonstrated its significant effect on glycemic control. According to ADA, participants were instructed to consume nonstarchy vegetables such as asparagus, green beans, carrots, and vegetable juices without added salt, fat, or sugar; fruits like apples, blueberries, oranges, and other fresh or canned options without added sugars; fat-free or low-fat options including unflavored soy milk, plain nonfat yogurt, and light yogurt without added sugars; grains and starchy vegetables such as whole grain foods, beans, peas, lentils, and starchy vegetables without added fats, sugars, or sodium; protein sources such as fish, chicken, and lean meats; and healthy fats from sources like avocados, olives, and seeds (flax, pumpkin, sesame). Whole grain foods such as cereals, breads, and grains with whole grains as the primary ingredient were also emphasized. 15 Participants received detailed instructions, translated into Arabic, and guidance from a nutritionist to modify their food choices based on individual factors, including weight and caloric needs, ensuring adherence to the dietary plan within the cultural and individual contexts of the participants.
2. Sleep: There was an association between both the quality and quantity of sleep and glycemic control.17 -19 Our objective was to improve the sleep quality of participants by following the guidelines provided by the National Sleep Foundation, which recommend aiming for 7 to 9 hours of sleep every night. 20
3. Vitamin D and magnesium: Magnesium and vitamin D supplementation are associated with a decreased risk of developing diabetes.21,22 Vitamin D is measured in the blood by assessing the concentration of 25-hydroxyvitamin D. This is the most accurate indicator of vitamin D status. 23 Magnesium is measured through blood tests, typically assessing the concentration of magnesium in the serum (serum magnesium level). 24 Although practitioners’ actual supplementation amounts may differ, we followed the protocol provided by Pepper et al. 25 for patients suffering from vitamin D insufficiency which recommends the following: 1,000 IU/day of vitamin D3 if 25(OH)D is 30–40 ng/ml, 2,000 IU/day of vitamin D3 if 25(OH)D is 20–30 ng/ml, and, for adults with serum levels <20 ng/ml, prescribe 50,000 IU of vitamin D2 once to three times per week for 4 weeks followed by 3,000 IU/day until serum 25(OH)D levels are >30 ng/ml. Then, recheck serum 25(OH)D levels 3–6 months later, and continue treating until serum levels are >40 ng/ml. As for magnesium, capsules containing MgSO₄ were used as magnesium supplements, with each capsule containing 100 mg of elemental magnesium. Based on the Recommended Dietary Allowance (RDA) for magnesium intake—400 to 420 mg/day for men, 310 to 320 mg/day for women, and 400 mg/day for pregnant and lactating women—we provided four capsules daily for male participants and pregnant or lactating women, totaling 400 mg of elemental magnesium, and three capsules daily for non-pregnant women, totaling 300 mg. 26
The Follow-up
The follow-up process was conducted individually for each participant, with a monthly assessment over a period of 6 months for each participant throughout the entire trial duration. Participants were queried regarding adherence to the prescribed protocol, any experienced discomfort, potential complications, and sensations such as tingling or pain. Detailed inquiries were made concerning the specific time and method of protocol application. A comprehensive physical examination was performed during each follow-up session, accompanied by a thorough review of the participant’s medical history. Furthermore, investigations of HbA1c levels were systematically conducted at every follow-up session, contributing to the comprehensive monitoring of participants’ health and treatment progress.
Statistical Analysis
Results were analyzed using Statistical Package for the Social Science (SPSS) version 25. The t-test was used to test the significant differences between the variables, and P-value < .05 was considered a statistically significant with a confidence interval of 95%. Odds ratio used to assess how strongly chronic non-specific low back pain associated with higher HbA1c.
Results
In this study, a total of 82 participants with chronic non-specific low back pain were evaluated prior to the interventions. The participants had a mean age of 38.61 years (SD ± 9.24), with the majority being female (61%). The average BMI of participants before the intervention was 26.08 (SD ± 2.33), and all individuals were included based on a BMI of less than 30 (Table 1).
Demographic and Health-related Data for the Participants.

In this study, a total of 82 participants with chronic non-specific low back pain were evaluated prior to the interventions. The participants had a mean age of 38.61 years (SD ± 9.24), with the majority being female (61%). The average BMI of participants before the intervention was 26.08 (SD ± 2.33), and all individuals were included based on a BMI of less than 30.
Prior to the interventions, the mean HbA1c level was 6.02% (SD ± 0.163), with participants meeting the inclusion criteria of having HbA1c levels between 5.7% and 6.4%. After 12 weeks of interventions, the mean HbA1c level decreased to 5.52% (SD ± 1.836). At 24 weeks, the mean HbA1c level further reduced to 5.17% (SD ± 0.124).
A statistical comparison of HbA1c levels and chronic non-specific low back pain after 12 weeks of interventions was conducted. Among participants who did not experience low back pain after 12 weeks, the mean HbA1c level was 5.378 (SD ± 0.0941). In contrast, participants who still reported low back pain had a mean HbA1c level of 5.626 (SD ± 0.1601). The comparison yielded a p-value of .021, indicating a statistically significant difference in HbA1c levels between those who experienced low back pain and those who did not. Additionally, an odds ratio (OR) of 0.041 suggests that participants with an HbA1c level lower than 5.5 were significantly less likely to experience chronic non-specific low back pain compared to those with an HbA1c level of 5.5 or higher.
After 12 weeks of interventions, chronic non-specific low back pain and HbA1c levels were compared statistically. Participants who no longer experienced low back pain after 24 weeks had a mean HbA1c level of 4.929 (SD ± 0.1747). In contrast, those who continued to experience low back pain had a mean HbA1c level of 5.219 (SD ± 0.1108). The associated p-value for this comparison was 0.005, indicating a statistically significant difference in HbA1c levels between the two groups. Furthermore, the odds ratio of 0.0001 suggests that chronic non-specific low back pain is significantly less likely in patients who achieved an HbA1c level below 5, compared to those with an HbA1c level of 5 or higher.
Discussion
The adverse effects of uncontrolled type 1 or type 2 diabetes on several organ systems are well-documented, including but not limited to cardiovascular disease, kidney disease, and neurological complications. 27 Individuals with diabetes mellitus often experience pain, a significant symptom that severely affects their quality of life. However, pain is not limited to those with diagnosed diabetes; prediabetic individuals also face a substantial burden of chronic pain. A study by Aldossari et al. revealed a strong association between pre-diabetes and diabetes with chronic pain, even after controlling for variables such as age, gender, education level, cholesterol, and smoking status. This highlights the importance of recognizing and addressing pain management early, even in prediabetic populations, to improve overall quality of life and prevent further complications. 28 The studies have shown contradictory findings regarding the relationship between diabetes and non-specific low back pain. The fact that low back pain was typically self-reported and that its definition differed among studies may explain the inconsistencies in these results. 29 Diabetes is positively associated with both low back and neck pain, according to a meta-analysis of eight studies conducted by Pozzobon et al. 30
Several factors are believed to contribute to chronic non-specific lower back pain in diabetic patients. These include cell death in spinal discs caused by hyperglycemia, the buildup of advanced glycation end products which speed up spinal degeneration, costochondritis, pain sensitivity around the lumbar spine, weak muscles, depression, and the sedentary lifestyle.5,6,12 A study by Rinaldo et al 5 suggested that exogenous insulin use may have a negative association with chronic back pain. Given that insulin is typically administered as a secondary treatment for type 2 diabetes, it is possible that over time, improved blood glucose control facilitated by insulin could lead to a reduction in CBP symptoms. This aligns with our study’s findings, which indicate that reducing HbA1c levels may lead to improvements in severity of chronic non-specific low back pain. Other diabetic medications, such as dipeptidyl peptidase-4 (DPP-4) inhibitors, have been reported to increase joint pain, further complicating the role of diabetes treatments in musculoskeletal pain.5,6,12
Vitamin D plays a significant role in both diabetes and musculoskeletal health, particularly in the context of low back pain. According to a study by Dutta et al., supplementing vitamin D in individuals with pre-diabetes who are deficient or insufficient in vitamin D reduces insulin resistance and lowers the risk of developing diabetes. This suggests that vitamin D may contribute to better glycemic control. 31 In relation to musculoskeletal pain, the connection between vitamin D and chronic back and neck pain is evident, though the exact mechanism remains unclear. One possibility involves imbalanced homeostasis of intracellular or extracellular electrolytes. Another potential factor is the role of vitamin D receptors in cellular signal transduction and mediation of immune responses, which may influence pain and muscle health. Further research is needed to clarify these pathways. 32
Magnesium has been shown to play a beneficial role in reducing blood glucose levels and improving insulin sensitivity. Many Studies has demonstrated that higher magnesium levels correlate with better glycemic control.33 -35 A meta-analysis by Dong et al. provides evidence supporting a significant inverse association between magnesium intake and the risk of type 2 diabetes, consistent with a dose-response relationship. 22 This improvement may be explained by the effect of magnesium on insulin receptor activity, where it enhances tyrosine kinase phosphorylation, leading to improved insulin action. Another possible mechanism involves magnesium facilitating the translocation of glucose transporter number 4 (GLUT4) to the cell membrane, thus aiding in glucose uptake. 33 In addition to magnesium’s role in glycemic control, its effects on low back pain remain controversial. According to Park et al.ʼs systematic review, neither the efficacy nor the safety of magnesium as a treatment for chronic pain has been adequately established. 36 While the current evidence is inconclusive, some trial data indicate potential analgesic benefits in chronic pain conditions. Similarly, Bayram et al. discovered that treating acute low back pain with magnesium did not lead to better clinical outcomes. 37 In the context of our study, while magnesium’s role in glycemic control is more established, its potential impact on musculoskeletal health, specifically low back pain, remains uncertain.
The significance of our study lies in addressing an important gap in the current research. While numerous studies have investigated the association between non-specific low back pain and diabetes, none have specifically examined whether improving glycemic control—by reducing HbA1c levels—can lead to a reduction in low back pain. This gap is critical because effective management of HbA1c in diabetic and pre-diabetic populations could potentially have broader musculoskeletal benefits beyond metabolic control. Our study aims to explore this relationship in detail, offering new insights into how optimizing glycemic control might positively affect chronic non-specific low back pain, a condition that significantly affects the quality of life in diabetic individuals.
The results of our 12- and 24-week analyses revealed a significant reduction in the severity of chronic non-specific low back pain following interventions aimed at lowering HbA1c levels. At 12 weeks, patients who continued to experience pain had higher mean HbA1c levels than those who reported complete resolution of their symptoms. This persisted at 24 weeks, where patients with no reported low back pain had significantly lower HbA1c levels than those with ongoing pain. These findings indicate that reducing HbA1c levels may lead to improvements in severity of chronic non-specific low back pain, suggesting that glycemic control could play a crucial role in alleviating this condition.
When considering current treatment guidelines for chronic low back pain, which primarily recommend the use of non-steroidal anti-inflammatory drugs, antidepressants where necessary, exercise therapy, and psychosocial interventions, the addition of strategies targeting glycemic control offers a promising complementary approach. Given that most guidelines also recommend referral to a specialist if there is no improvement within 4 weeks to 2 years or if serious pathologies like radiculopathy are suspected. 38 Our study provides evidence that glycemic optimization may serve as an adjunct to traditional treatments. It suggests that individuals with chronic non-specific low back pain could benefit from not only pharmacological and therapeutic measures but also from dietary adjustments and other interventions aimed at lowering HbA1c levels. This integrated approach could enhance treatment outcomes, particularly for patients with diabetes or pre-diabetes, by addressing the metabolic contributions to musculoskeletal pain.
Limitations
This study has potential limitations. One may be the small sample size included in the intervention which limits the generalizability of our findings and allows for variability to influence results interpretation. Furthermore, the lack of data from previous literature on the incidence of non-specific low back pain in prediabetics makes the subject more challenging to approach. An existing gap in the literature on this subject may present the opportunity to conduct further research on a lager scales. Additionally non-specific low back pain is a subjective self-reported measure; therefore, it may be liable to the exaggeration bias. The model also provides effect estimates that are based on interventional and prospective observational studies that are subject to biases and confounding. Our aim was to improve the sleep quality of participants by following the guidelines provided by the National Sleep Foundation. However, while we focused on the recommendations for sleep duration, we did not incorporate validated sleep quality scales or indexes. This study did not exclude smokers, as smoking may affect low back pain, potentially influencing the study results. Also, A limitation of this study is the lack of a formal sample size calculation or power analysis, which may affect the generalizability and robustness of the findings. Future studies should consider incorporating a formal power analysis to ensure adequate sample size for detecting clinically significant effects.
Recommendations
Considering, these findings, new insights into back pain management targeting better glycemic control may be adopted. One could argue that the most obvious practical implication is the incorporation of new management strategies targeting tighter glycemic control and optimization of nutritional statuses seems to have a marked effect on the severity of chronic non-specific back pain. Thus, evaluation algorithms may be developed to address different aspects of low back pain assessment. Future research should further explore nature of the association of HBA1C levels and chronic nonspecific low back pain, while at the same time guiding practitioners to incorporate new management approaches when dealing with prediabetic patients.
Conclusion
This study suggests a significant association between chronic non-specific low back pain and the reduction in HbA1c levels. Thus, enhancing glycemic control through dietary modification, sleep optimization and correction of vitamin and mineral deficiency may lead to an improvement in chronic non-specific low back pain among prediabetic individuals. The results of our study suggest that glycemic control could be useful in addition to conventional therapies. It implies that, in addition to pharmaceutical and therapeutic measures, dietary changes along with other interventions targeted at reducing HbA1c levels may be beneficial for individuals who suffer from chronic non-specific low back pain. This comprehensive method has the potential to improve treatment results by targeting the metabolic factors that might contribute to musculoskeletal pain.
Supplemental Material
sj-docx-1-end-10.1177_11795514241300995 – Supplemental material for Assessing the Effects of HbA1c Reduction on Alleviating Chronic Nonspecific Low Back Pain in Prediabetic Non-obese Patients: A Non-Randomized Controlled Trial
Supplemental material, sj-docx-1-end-10.1177_11795514241300995 for Assessing the Effects of HbA1c Reduction on Alleviating Chronic Nonspecific Low Back Pain in Prediabetic Non-obese Patients: A Non-Randomized Controlled Trial by Ghazwan Abdulla Hasan, Ahmed Dheyaa Al-Obaidi, Hashim Talib Hashim, Mustafa Najah Al-Obaidi, Yousif Ali Al-Saady, Assalah Othman, Sara S. Khunda, Omar Saab, Hasan Al-Obaidi and Nooraldin Merza in Clinical Medicine Insights: Endocrinology and Diabetes
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.