
Abstract
COVID-19, a global epidemic of infectious disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), not only initially refers to acute manifestations but also chronic symptoms known as Long COVID-19. Long COVID-19 represents a significant burden to healthcare systems worldwide. This syndrome encompasses a wide range of continuing health problems with variable durations and consequences for patients’ everyday lives. A notable aspect of Long COVID-19 is the emergence of new-onset autoimmune diseases that could be triggered in predisposed patients with altered immune responses. Common autoimmune conditions that arise in post-COVID patients include autoimmune hemolytic anemia, immune thrombocytopenic purpura, autoimmune thyroid diseases, Kawasaki disease, Guillain-Barre syndrome, etc., but with unclear evidence of associated disease occurrence. We present a case of a female rheumatoid arthritis patient who developed autoimmune thyroid disease, latent autoimmune diabetes of adults (LADA), and pernicious anemia after SARS-CoV-2 infection.
Keywords
Introduction
COVID-19 is a global epidemic of infectious disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Although initially referring to acute manifestations, chronic symptoms known as Long COVID have been recognized as a significant component of the disease and pose a great burden on healthcare systems worldwide. 1 Long COVID includes a wide range of continuing health problems with variable durations and consequences for patients’ everyday lives. A notable aspect of Long COVID is the emergence of new-onset autoimmune diseases that could be triggered in predisposed patients with altered immune responses. 2 Common autoimmune conditions that arise in post-COVID patients include autoimmune hemolytic anemia, immune thrombocytopenic purpura, autoimmune thyroid diseases, Kawasaki disease, Guillain-Barre syndrome, etc., but with unclear evidence of associated disease occurrence. 3 We present a case of a female patient with rheumatoid arthritis who developed autoimmune thyroid disease, latent autoimmune diabetes of adults (LADA), and pernicious anemia after SARS-CoV-2 infection. Written informed consent from the patient to publish the study was obtained, as well as ethical approval from the Ethics Committee of the Faculty of Medicine, University of Belgrade, with the approval number 25/V—20.
Case Representation
A 58-year-old woman with a medical history of rheumatoid arthritis (RA), Sjogren’s syndrome, osteoporosis, and hypertension was admitted to the hospital with a high fever and dry cough. The patient’s blood count revealed leukocytosis, lymphopenia, as well as elevated levels of CRP. The nasopharyngeal swab was PCR-positive for the SARS-CoV-2. A chest X-ray revealed a mild form of pneumonia. The patient was treated mostly with supportive therapy. After 5 days she was discharged home in good general health condition, normoglycemic and euthyroid.
Approximately 4 months after the COVID-19 infection, she went back to the hospital with symptoms that had lasted for the past 3 weeks. These symptoms included dry mouth, increased fluid intake, and extreme fatigue. The patient was undergoing antihypertensive therapy and Methotrexate therapy for the treatment of rheumatoid arthritis (RA), which had been diagnosed in 2016 along with Sjogren’s syndrome. Initially, the patient was treated with corticosteroid therapy (Pronison tablets). On admission test results revealed extreme hyperglycemia (35 mmol/l), glycosuria, ketonuria, and values of HbA1c over 10%. The patient was not previously treated for diabetes, nor hyperglycemic episodes were registered. The sudden onset of the disease led us to doubt autoimmune diabetes so we checked for autoantibodies. In laboratory analysis, we found elevated levels of anti-GAD antibodies—4988 IU/ml and anti-IA2 antibodies—21 U/ml (<1). Glucagon test revealed low endogenous insulin reserve with an initial value of C peptide of 11.0 pmol/l and later 21.0 pmol/l, insulin levels in the zeroth and sixth minute were 308.2 and 284.9 pmol/l. All of the mentioned tests led to a diagnosis of LADA, and the patient was placed on an intensive basal/bolus insulin regimen consisting of 4 doses per day. Prandial short-acting insulin (Human Actrapid) was injected 3 times daily before main meals, while intermediate-acting insulin (Human Insulatard) was administered only at 22:00 hours. Later, the patient’s treatment was adjusted to include 3 doses of rapid-acting prandial analog insulin apart and 1 dose of long-acting analog insulin degludec. The patient utilized continuous glucose monitoring (CGM) to improve glycemic control. For optimal management of type 1 diabetes mellitus (T1DM), the patient was educated on matching prandial insulin doses to carbohydrate intake, premeal blood glucose levels, and anticipated physical activity, as well as on how to measure their blood glucose and manage insulin dosing under various circumstances.
Because of the pluriglandular syndrome, we conducted additional tests to evaluate the thyroid gland function. Thyroid gland hormones were within physiological range but with elevated TPO antibodies—42 IU/ml, which indicated potential autoimmune thyroid disease. Echo of the thyroid gland ultrasound revealed hypoechogenic, nonhomogenic echostructure, a slightly more pronounced Color Doppler (CD) signal with mixed micronodules in both lobes, as can be seen at the ultrasound image (Figure 1).
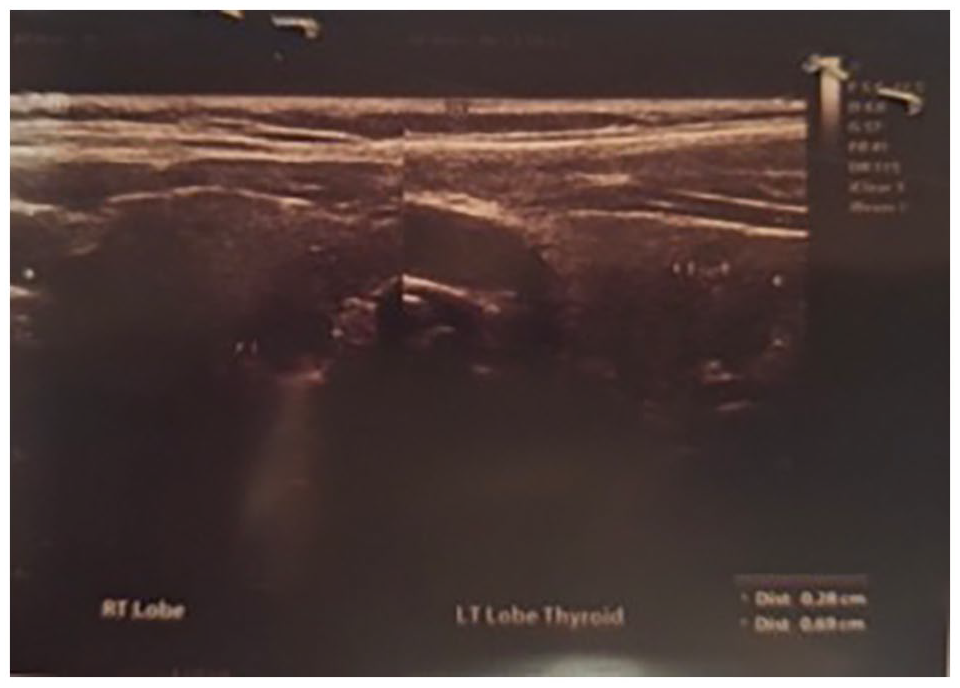
Thyroid micronodular appearance. The ultrasound image shows a hypoechoic, nonhomogeneous echostructure with a slightly stronger Color Doppler (CD) signal and mixed micronodules present in both lobes.
Further, due to the dyspeptic problems and dry mouth, we checked for B12 level. Lab results showed lower values of vitamin B12—152 ng/l and parameters of macrocytic anemia. To detect the origin of B12 deficiency parietal antibodies and antibodies to intrinsic factor were examined. Results showed positive and elevated both types of antibodies. For final confirmation of the diagnosis of pernicious anemia, esophagogastroduodenoscopy and histopathological samples were conducted. Findings confirmed autoimmune atrophic gastritis.
The patient undergoes regular monitoring by rheumatologists, endocrinologists, and gastroenterologists. Previous immunological analyses for autoimmune diabetes mellitus, thyroid disease, and macrocytic anemia were negative.
Discussion
COVID-19 has been confirmed in 770 million people worldwide as of September 2023. However, it is estimated that the actual number of infected patients is much higher, with over 30% of confirmed COVID-19 cases occurring in asymptomatic individuals, and approximately 80% of those hospitalized due to experiencing symptoms develop what is called Long-COVID-19, even without any previous history of illness. The National Institute for Health and Care Excellence defines Long-COVID-19 syndrome as a set of symptoms that develop during or after a COVID-19 infection and last for more than 12 weeks without a proper clinical explanation provided by alternative diagnoses. 4
Noteworthy components of Long-COVID-19 are autoimmune diseases. It has been shown that viral infection can lead to autoimmunity through 3 potential mechanisms: molecular mimicry, bystander T-cell activation, and epitope spreading. 5 The coronavirus responsible for COVID-19, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), gains cellular access through the angiotensin-converting enzyme (ACE2) receptor, a process that requires the transmembrane serine protease 2 (TMPRSS2) protein. Both ACE2 and TMPRSS2 are widely expressed in many endocrine glands. Latent Autoimmune Diabetes in Adults (LADA) is a type of diabetes characterized by the gradual autoimmune destruction of the beta islets in the pancreas. It is described as insulin-independent in the early phase, but with time, and gradual loss of beta cells it progresses to insulin-dependent. 6 As for laboratory findings, LADA patients have positive or elevated levels of islet cell antibody (ICA), glutamic acid decarboxylase antibody 65 (GAD65), or islet antigen 2 (IA2). The patient from our case had multiple times higher values of GAD65 antibodies which confirm diagnosis of LADA. Through a review of the literature, it has been observed that SARS-CoV-2 could induce type 2 diabetes, but there is limited evidence for links to type 1 diabetes. Lee et al 7 presented a case of a 46-year-old male who was diagnosed with de novo LADA 2 days after a COVID-19 infection, with pre-existing type 2 diabetes. LADA was confirmed by positive and elevated IA2 antibodies. One possible mechanism for diabetes pathogenesis in COVID-19 patients could be explained through increased expression of ACE2 messenger ribonucleic acid (mRNA). The expression of ACE2 mRNA in the pancreas has been shown to induce damage and acute dysfunction of beta cells, which could lead to diabetes in healthy individuals or exacerbate already existing diabetes with the developing of ketoacidosis. 8
Autoimmune diseases in the endocrine system are often associated with and presented as a pluriglandular autoimmune syndrome. Due to the symptoms at the admission, a patient from our case was evaluated for thyroid disease. We found that she has a micronodular thyroid gland, level of thyroid hormones within physiological range, and elevated TPO antibodies that led us to doubt for autoimmune thyroiditis. Feghali et al presented a case of a 38-year-old woman who had a severe form of COVID-19, and a month later started experiencing extreme fatigue, enlargement of the thyroid gland, and hair loss. Laboratory tests, neck ultrasound, and fine needle aspiration biopsy led to a diagnosis of Hashimoto’s thyroiditis. 9 Possible explanation of these findings could be due to the same mechanism in LADA, as it is known that ACE2 receptors are present in the parenchyma of the thyroid gland, making it a potential target for SARS-CoV-2 infection. Also, thyroid hormones and immunomodulatory signaling molecules are involved in the complex interplay between the thyroid gland and viral infection, so the hypofunction of the thyroid gland could lead to an alterated immune response. 10
Pernicious anemia is the most common cause of vitamin B12 deficiency worldwide. It is an autoimmune disease characterized by chronic atrophic gastritis and inadequate absorption of B12 from the terminal ileum due to the destruction of the intrinsic factor (IF) by autoantibodies. 11 Our patient had a decreased B12 level, accompanied by positive antiparietal antibodies and a gastroscopy finding of atrophic gastritis. The mechanism of possible correlation of COVID-19 and pernicious anemia could be through One-Carbon metabolism. Cells infected with SARS-CoV-2 modulate their metabolism due to the need for massive viral RNA synthesis, which requires biosynthesis of de novo purines involving folate, B12, and one-carbon metabolism. Also, according to some previous data pernicious anemia is commonly associated with LADA. 12
Studies suggest people with RA may be at increased risk for coronavirus infection and long COVID due to underlying altered immunity, treatment with immunosuppressants (especially glucocorticoids) and additional chronic conditions (comorbidities).13,14 Within the subset of patients with RA infected with SARS-CoV-2, treatment with rituximab was associated with an increased risk for hospitalization (OR 6.12; 95% CI 2.89-12.92) and mortality (OR 12.06; 95% CI 3.90-37.3). Treatment with Janus kinase inhibitors was also associated with an increased risk for hospitalization (OR 2.18; 95% CI 1.56-3.06).14 -16
Conclusion
To summarize, our findings reveal 2 endocrinological autoimmune diseases and macrocytic anemia in a post-COVID-19 patient with RA. This indicates a potential role of SARS-CoV-2 as a trigger for specific autoimmune conditions. Future investigations should prioritize long-term observational studies in rheumatoid arthritis cohorts to monitor the incidence of endocrinological autoimmune disorders.