
Abstract
Hyperglycaemia during inpatient admission is indicative of higher morbidity and mortality risks in critically ill patients. The severe acute respiratory distress coronavirus 2 (SARS-CoV-2) has been reported to induce ketoacidosis and diabetic ketoacidosis (DKA) even in nondiabetic patients. The pathophysiology of the SARS-CoV-2 infection that can contribute to hyperglycaemia, and the exacerbated inflammatory cytokine storm can overlap with the metabolic chronic inflammatory state attributable to the metabolic syndrome, which underlies diabetes mellitus. In this report, we explore the possible pathophysiology and metabolic mechanisms that lead to metabolic acidosis in nondiabetic patients.
Background
Diabetic ketoacidosis is the commonest hyperglycaemic crisis of decompensated diabetes. 1 In diabetic ketoacidosis, excessive ketone body formation and acidosis occur in the clinical setting of pathological absolute or relative insulin deficiency. 1 Hyperglycaemia has been recognized as a common finding in critically ill patients and is considered a sign of greater morbidity in previously nondiabetic patients. 2 During the pandemic caused by the severe acute respiratory distress coronavirus 2 (SARS-CoV-2), the coronavirus disease (COVID-19) has been reported to cause ketoacidosis and induce DKA in nondiabetic patients. 3 In a study conducted among 658 hospitalized patients with confirmed SARS-CoV-2 infection, 42 (6.4%) patients presented with ketosis at the time of admission; 27 of these 42 patients did not have a history of diabetes. Thus, 2 out of 5 patients with diabetic ketoacidosis at hospital presentation were previously not known to have diabetes. 3 During the peak of the COVID-19 outbreak in our region, we experienced a similar surge in diabetic ketoacidosis cases in nondiabetic patients. However, it remains to be ascertained whether the SARS-CoV-2 infection accelerates the metabolic processes in undiagnosed diabetes patients or has a different inflammatory process that overwhelms the body’s defensive metabolic mechanisms to induce diabetic ketoacidosis.
Severe acute respiratory syndrome (SARS), which occurred as an outbreak in 2003, was initially recognized as atypical pneumonia caused by a virus of the coronavirus family, now named SARS-CoV-1. Notably, soon after, hyperglycaemia was reported to be a predictor of mortality in diabetes and non-diabetes patients with acute illnesses. 4 Both SARS-CoV-1 and SARS-CoV-2 belong to the diverse coronavirus family, and despite this, both viruses have many differences. 5
In this report, we present a representative case of a man without a previous diabetes diagnosis who had COVID-19 pneumonia at hospital presentation and developed diabetic ketoacidosis soon thereafter. This case was reviewed by the ethical and institutional review board committee to protect the patient’s privacy.
Case Presentation
A 36-year-old man with a history of traumatic brain injury, followed by depression and maintenance therapy with antidepressant drugs but without other relevant medical history, presented to our emergency department after a few days of experiencing shortness of breath, fever, and cough. Physical examination initially revealed hypotension (blood pressure 96/65 mmHg), tachycardia (heart rate 116 beats per minute), tachypnoea (respiratory rate 29 breaths per minute), impaired oxygenation (oxygen saturation 84% on room air), hyperglycaemia (blood glucose 375 mg/dL), and fever (temperature 38.6°C). The patient was immediately started on supportive oxygen via mask, and his saturation increased to 95% on 6 L of oxygen. On general examination, the patient was conscious and oriented (Glasgow Coma Score 15) and appeared tired and unwell, without other significant physical findings. By Day 5, the clinical condition of the patient had not improved markedly, and his clinical picture and laboratory values began to worsen, with sinus tachycardia (164 beats per minute), tachypnoea (respiratory rate 30 breaths per minute), fever (temperature 38°C), and his oxygen saturation remained 95% on room air.
Investigations
The results of the initial laboratory tests showed a white blood count of 6.31 × 109 cells/L, with high neutrophil percentage (80%) and lymphopenia (13%). Venous blood gas analysis showed a pH of 7.31 and bicarbonate of 20 mmol/L with an anion gap of 23.8 mmol/L. The D-dimer level was high at 1.56 µg/mL. Chest radiography revealed bilateral hazy opacities in the lower lobes, but predominantly on the left side. Therefore, the patient was admitted to the intensive care unit (ICU) with a diagnosis of pneumonia and high suspicion of SARS-CoV-2 infection. The results of the respiratory viral panel were negative for other viruses, and the polymerase chain reaction (PCR) test of the nasopharyngeal swab was positive for SARS-CoV-2. During hospitalization, the patient’s blood glucose level and anion gap continued to increase despite treatment. On Day 5, the results of the laboratory test showed an increased anion gap (43.2 mmol/L), hypernatremia (sodium 164 mmol/L), acidosis (HCO3 6.4 mmol/L), osmolality of 395, venous pH of 7.1, and blood glucose level of 500 mg/dL, and his glycated haemoglobin level was 14.9%.
Differential Diagnosis
The initial differential diagnosis included pneumonia, COVID-19, dehydration, sepsis, ketosis, and diabetic ketoacidosis, which are all likely pathologies to be considered in patients presenting with the abovementioned clinical condition.
Treatment
The patient was clinically managed in accordance with a diabetic ketoacidosis protocol, and his clinical condition soon improved. The treatment included the initiation of insulin therapy, managing the fluid deficit to correct the dehydration status, and potassium monitoring and correction as needed. The patient received supportive care for COVID-19 that included oxygen supplementation and antibiotic and interferon therapy. No corticosteroids were administered because of the patient’s hyperglycaemic state.
Outcome and Follow-Up
The patient was discharged after 13 days of hospitalization with a diagnosis of new-onset diabetes mellitus and was instructed to continue an insulin regimen after discharge (Table 1).
Laboratory parameters of the patient during hospitalization.

Discussion
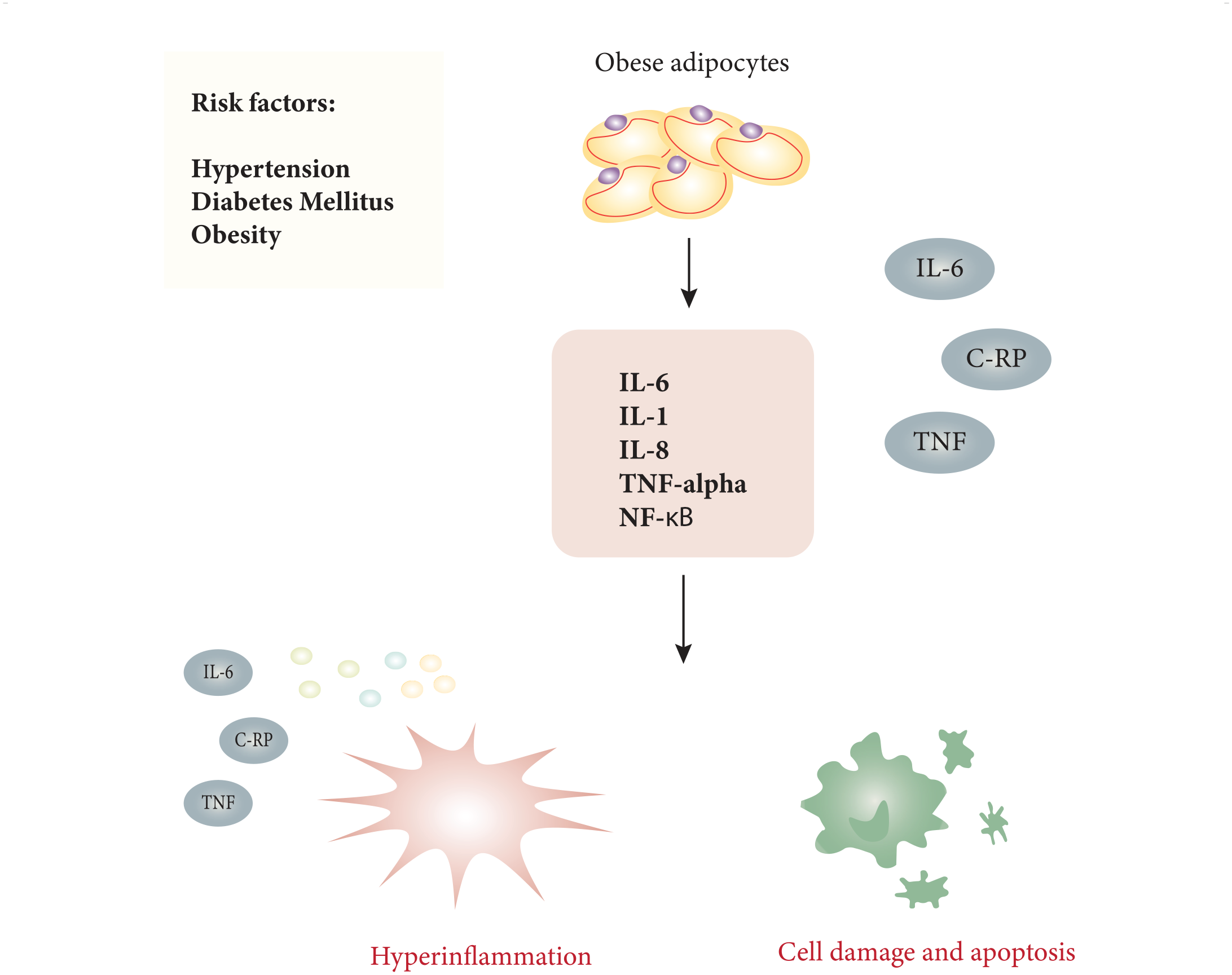
Hyperglycaemia is a common finding in critically ill patients and can be used as a prognostic factor for predicting the morbidity and mortality risk of inpatients. 2 Elevated levels of proinflammatory cytokines, such as tumour necrosis factor-alpha (TNF-α), interleukin 6 (IL-6), IL1-beta, and IL-8, have been associated with hyperglycaemia, regardless of the patient’s diabetic status. 6 Moreover, higher levels of cardiovascular biomarkers, oxidative stress, and plasma lipid peroxidation have been detected along with hyperketonaemia in patients with diabetes.7,8 Notably, the secretion of these cytokines (TNF-α and IL-6) is interrelated with the pathological states of obesity and insulin resistance. 9
Adipokines are a collective set of hormones and signalling molecules secreted by the adipose tissue and have major roles in the modulation of glucose metabolism and immunity. Adipokines contribute to insulin resistance by exhibiting proinflammatory or anti-inflammatory properties. 10 The obesity-related state of “metabolic inflammation” (chronic low-grade systemic inflammation) is considered a major factor in the pathogenesis of insulin resistance. 11 In 1999, it was found that adipocytes synthesize and secrete TNF-α, 12 which is believed to induce insulin resistance by multiple mechanisms, although mainly through the promotion of lipolysis and downregulation of adipogenic genes as well as the activation of (NF-κB) genes that are involved in lipid uptake and storage.13,14 Furthermore, TNF-α induces IL-6 production, thereby inhibiting glucose uptake and impairing insulin signalling (Figure 1). 15
Conditions that are associated with a higher risk of chronic low-grade systemic inflammation confer an increased risk for metabolic inflammation.
In the SARS-CoV-2 era, multiple reports have linked obesity with severe illness, use of invasive mechanical ventilation, ICU admission, and higher mortality.16-19 A report indicated the doubling of the risk for critical illness necessitating ICU admission or resulting in death associated with obesity in COVID-19 patients. 20 However, the exact association, if any, and suggested mechanisms are yet to be established because metabolic and immunologic cellular interactions are complex and require delineation through further research. 16
During the previous SARS-CoV-1 outbreak, hyperglycaemia and type 2 diabetes mellitus were identified as independent predisposing factors for morbidity and mortality. 21 In 1 study, 50% of the patients hospitalized with SARS-CoV-1 infection developed diabetes during their hospitalization. 4 This finding was attributed to the direct damage to the pancreatic β-cells by the virus that resulted in acute hyperglycaemia and transient type 2 diabetes mellitus. 4 It was then postulated that the metabolic inflammatory state associated with obesity could enhance cytokine release during a SARS-CoV-1 infection. 4 With the COVID-19 pandemic, SARS-CoV-2 infection was reported to cause ketoacidosis and induce diabetic ketoacidosis in patients with diabetes. 3 Few of those diabetic ketoacidosis-related admissions have been reported for previously nondiabetic patients.3,22
In 1 retrospective observational study in which 1122 hospitalized patients with COVID-19 in 88 United States hospitals were studied, patients with diabetes and/or uncontrolled hyperglycaemia had a longer length of stay and higher mortality than patients who did not have diabetes or uncontrolled hyperglycaemia.23,24 Patients with pre-existing diabetes are thought to be highly susceptible to COVID-19 and are associated with further increased mortality. 25 The exact mechanism underlying this association is still to be explored. In another retrospective report, hyperglycaemia has been linked to worsening initial radiological findings in acute respiratory distress syndrome patients. 26
It has been theorised that, in COVID-19, the associated cytokine storm (exaggerated release of inflammatory cytokines) plays a major role in the disease severity and has been attributed to the powerful activation of the systemic inflammatory response.27-29 Excessive visceral adipose tissue in obesity is known to induce mitochondrial production of reactive oxygen species (ROS), along with higher levels of proinflammatory cytokines, such as IL-6 and C-reactive protein levels.16,30 This inflammatory damage is further exacerbated by the oxidative stress induced by the higher ROS level associated with the SARS-CoV-2 infection. Mainly, the Toll-like receptor 4 (TLR4) pathway is thought to be triggered by the SARS-CoV-2 infection and amplifies the host’s inflammatory response.31,32 In hyperglycaemic states, increased ROS production will induce increased glycosylation and activation of protein kinase C. These changes will induce further cellular damage and apoptosis that will increase cell-cell adhesion and disrupt coagulopathies. 32 Moreover, animal studies have revealed that enhanced ROS expression with dysfunction of the antioxidant defence systems can tremendously affect and exacerbate the host’s cellular responses. 33 This imbalance and the weakened metabolic ability to counteract the increased oxidative stress is further strained by the prothrombotic and systemic inflammatory states in COVID-19. The overexpression of proinflammatory markers and higher lipid peroxidation levels have been noted in hyperglycaemic patients, regardless of the SARS-CoV-2 status upon admission. 4
Furthermore, it is important to note that SARS-CoV-2 disrupts pancreatic β-cell function by interacting with its ACE2 receptors, which are concentrated in type II alveolar cells, macrophages, and pancreatic cells and have been implicated in hypertension, diabetes, and heart failure.4,34-36 In addition, it has been postulated that the overactivation of the renin–angiotensin–aldosterone system (RAAS) can cause insulin resistance by interfering with glucose uptake in the target tissues, leading to hyperglycaemia and excessive oxidative stress because of increased ROS production.37,38 The binding of the SARS-CoV-2 virus to the ACE2 receptors results in the accumulation of angiotensin II, which can also activate the NF-κB and IL-6 pathways.34,39 When stimulated by the release of TNFα, or other cell stressors, the NF-κB pathway can exaggerate the proinflammatory process. 40
The binding of the SARS-CoV-2 virus to ACE2 receptors can lead to further disruption of the major components involved in the homeostasis of the RAAS, which may play an important role in the pathophysiology of DKA in patients with COVID-19 (Figure 2).41-43

Exacerbation of different pathogenic mechanisms underlying cellular damage in the hyperglycaemic state, thereby generating a cytokine storm in severe coronavirus disease.
As we continue to better understand COVID-19 and the implications of its cytokine storm on the metabolic, oxidative, and inflammatory stresses on the body, it is important to monitor this aspect in COVID-19 patients. The approach to the clinical management of COVID-19 patients should consider the specific pathophysiology associated with SARS-CoV-2 infection.
Nonetheless, a diagnosis of diabetes mellitus cannot be confirmed until further testing on follow-up. However, other factors besides virus-induced diabetes, such as genetic variations, laboratory interference (eg, carbamylated haemoglobin), and antipsychotic medication use, can contribute to elevated glycated haemoglobin levels.44,45 Further studies to ascertain the metabolic and inflammatory abnormalities in COVID-19 patients can provide insights to develop different treatment approaches and strategies, such as the use of anti-inflammatory, antiviral, targeted immunomodulation, and antioxidant therapies. The possibility of ketosis and DKA should be considered in all COVID-19 patients, as it worsens the morbidity and mortality risks. Moreover, longer follow-up for recovered COVID-19 patients should be undertaken as it is unknown whether COVID-19–induced diabetes is a transient or permanent condition.
Ketosis and ketoacidosis should be considered in all hospitalized COVID-19 patients as they can increase the morbidity and mortality risks. The metabolic, oxidative, and inflammatory stresses associated with the SARS-CoV-2 infection can increase the burden of a cytokine storm in patients with chronic inflammatory conditions. Inflammatory and oxidative abnormalities should be considered when defining the treatment strategies in patients with a SARS-CoV-2 infection. This case report is limited by the sample size and its retrospective nature; hence, it is mainly aimed to highlight this theory and emphasize the need to further explore this finding and the possible mechanisms to support or refute this hypothesis.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.