
Abstract
Irreversible pulmonary arterial hypertension is considered a contraindication for surgical or percutaneous closure of atrial septal defects (ASD) due to risk of right heart failure. We present a case of 37 years-old woman who was referred to our center due to progressive worsening fatigue and high probability of pulmonary hypertension on a transthoracic echocardiogram. The diagnostic work-up revealed the presence of an ostium secundum atrial septal defect and severe pre-capillary pulmonary hypertension on right heart cathetherization (RHC). The patient was considered inoperable and started medical therapy with sildenafil and bosentan. After one year of treatment, she repeated RHC that showed a significant reduction in pulmonary vascular resistance making her eligible for closure. Surgical closure of ASD with a fenestra was performed with success. Our case emphasizes the importance of individual assessment even if cases where initial evaluation is unfavorable to closure in accordance with the guidelines.
Keywords
Introduction
During the past few years, remarkable scientific advances have been made regarding pulmonary hypertension (PH) treatment. However, the presence of the latter in a subgroup of patients (pts) with congenital heart disease, especially atrial septal defect (ASD), still poses a clinical dilemma. Pts with ASD and mild PH are ideal candidates for closure, preventing disease progression, the same is not true for pts with more advanced degrees of PH. 1

Pulmonary scintigraphy images before anticoagulation showing multiple small perfusion defects.

ASD measurements in 2D and 3D bicaval imaging plan, respectively, by transesophageal echocardiogram.
This is explained by the fact that ASD serves as a pressure outlet, in cases of greater physical effort or PH crisis. 2 Indeed, according to guidelines of the American College of Cardiology and American Heart Association, ASD closure is contraindicated in pts with net right to left shunt or with elevated pulmonary artery pressure and pulmonary vascular resistances (PVR) higher that two-thirds systemic.1,2 Whether treatment with pulmonary artery vasodilators is this subgroup of patient is valuable promoting future closure, is still not well understood.
Case Report
A 37-year-old female patient with no previous medical history, was referred to our Pulmonary Hypertension Unit due to complains of progressive fatigue (functional class WHO II). She had performed a previous transthoracic echocardiography that revealed high probability for pulmonary hypertension, showing dilatation of right ventricle and pulmonary trunk and pulmonary artery systolic pressure of 85 mm Hg.
Taking into account the findings in the previous exams, a more specific diagnostic work-up was performed. Blood analysis and pulmonary functional test were normal. Cardiopulmonary exercise test (CPET) demonstrated decreased functional capacity (Peak VO2 17,1; 50% of predicted; desaturation from 99% to 94%). Pulmonary scintigraphy (PS) showed presence of bilateral pulmonary embolism, with multiple perfusion defects (Figure 1).
A new complete transthoracic echocardiogram (TTE) was performed, that revealed a dilated and dysfunctional right ventricle (TAPSE 13 mm, Tricuspid S’ 8 cm/sec, FAC 30%) with a pronounced systodiastolic D-shape of the left ventricle and a positive agitated saline test after Valsalva Maneuver (Video 1). Afterwards she was submitted to a transesophageal echocardiogram that confirmed the presence of an ostium secundum atrial septal defect (OS-ASD) (1.86 × 1.34 cm) with bidirectional flux (Figure 2).
It was decided to start anticoagulation for 3 months, after which a new PS showed resolution of perfusion defects.

TTE showing a dilated and dysfunctional right ventricle with a pronounced systodiastolic D-shape of the left ventricle. Positive agitated saline test after Valsalva Maneuver, confirmed the presence of a significant atrial shunt.

One year after ASD closure, TTE revealed a significant improvement in right ventricle dilatation and systolic function, as well as right ventricle overload signs. TTE subcostal view showed no signs of residual shunt.
A right heart catheterization (RHC) was performed and confirmed the presence of precapillary severe pulmonary hypertension (Table 1). Vasoreactivity test with epoprostenol was negative, supporting its irreversibility.
RHC and CPET results before and after pulmonary vasodilator therapy and after surgical repair.
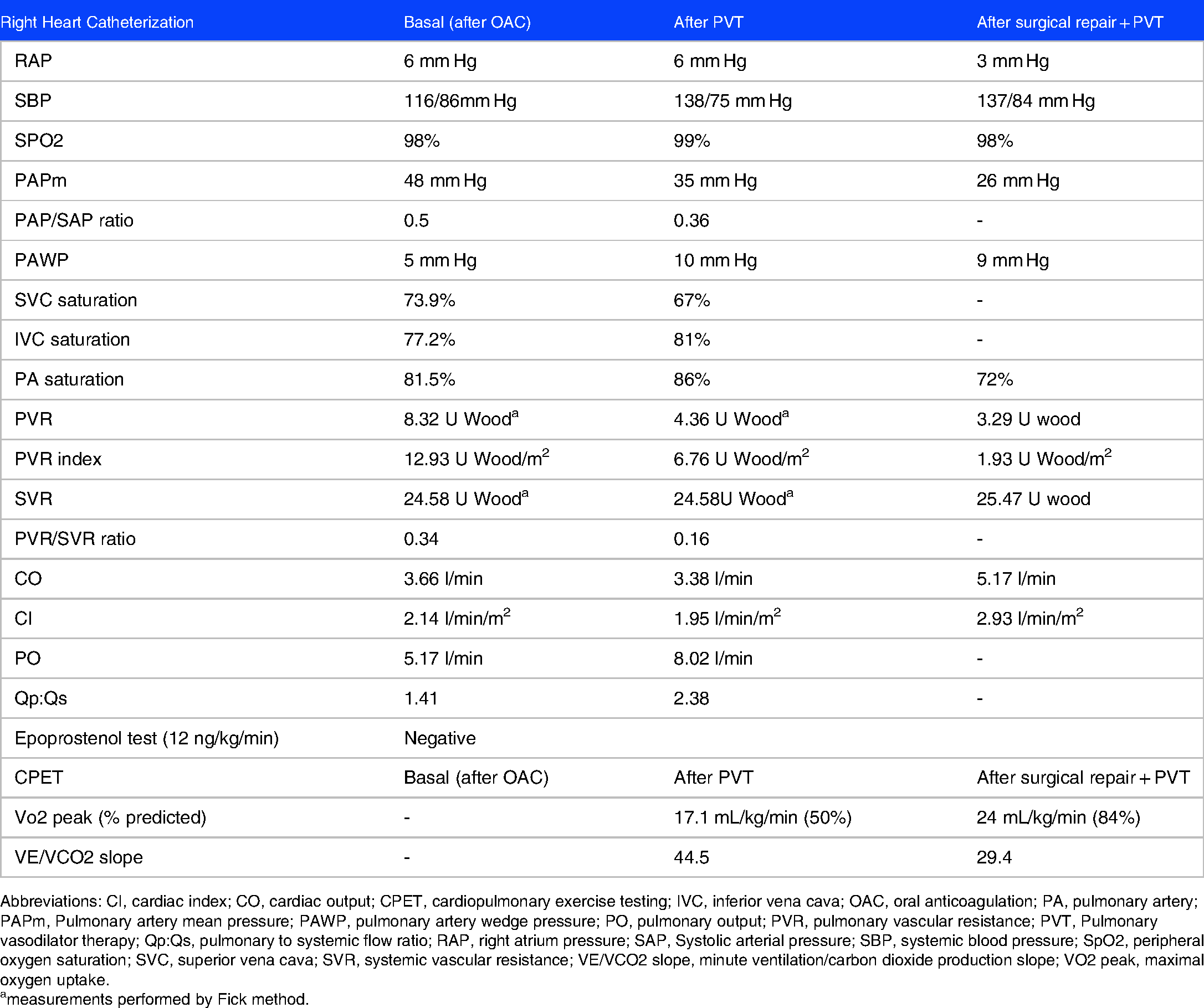
Abbreviations: CI, cardiac index; CO, cardiac output; CPET, cardiopulmonary exercise testing; IVC, inferior vena cava; OAC, oral anticoagulation; PA, pulmonary artery; PAPm, Pulmonary artery mean pressure; PAWP, pulmonary artery wedge pressure; PO, pulmonary output; PVR, pulmonary vascular resistance; PVT, Pulmonary vasodilator therapy; Qp:Qs, pulmonary to systemic flow ratio; RAP, right atrium pressure; SAP, Systolic arterial pressure; SBP, systemic blood pressure; SpO2, peripheral oxygen saturation; SVC, superior vena cava; SVR, systemic vascular resistance; VE/VCO2 slope, minute ventilation/carbon dioxide production slope; VO2 peak, maximal oxygen uptake.
measurements performed by Fick method.
Based in these results, ASD was not considered for closure and medical therapy with sildenafil 50 mg 3 times/day and bosentan 125 mg 2 times/day was started, with good clinical tolerability.
After one year of treatment, she repeated RHC that showed a significant improvement in pulmonary hypertension, but with an increase in Qp:Qs (Table 1). The case was discussed in a multidisciplinary team with cardiology, interventional cardiology, and cardiac surgery. Since the borders of the ASD were not suitable for percutaneous closure (large ASD with highly mobile edges), she was referred for surgical closure. The patient was accepted and was submitted to surgical closure with a 4.5mm-fenestrated patch, with success. Six months after surgery, the patient was on WHO class I, with a significant improvement of peak VO2 to 24,1 mL/kg/min (81% of the predicted) and of the TTE signs of right heart dysfunction (TAPSE 22mm, Tricuspid S’ 14cm/sec, FAC 37%). She repeated RHC that showed only mild pulmonary hypertension (Table 1). The patient is currently on pulmonary vasodilator therapy (PVT) with sildenafil 25 mg and bosentan 150 mg, remaining asymptomatic from a cardiovascular point of view.
Discussion
Patients having ASD with moderate-to-severe PH create a clinical dilemma due to lack of solid data.1‐5 Determining reversibility of PH plays an important role in treatment decision.3‐5 Closing ASD in patients with irreversible PH can be clinically catastrophic and it's not recommended. On the other hand, not closing in pts with reversible PH deprives them of clinical improvement.3,4
According to American College of Cardiology and American Heart Association guidelines, ASD closure is contraindicated in pts with net right to left shunt or with elevated pulmonary artery pressure and PVR higher that two-thirds systemic. European Society of Cardiology, in turn, consider ASD closure contraindicated if PVR > 5 mm Hg after PVT and significant shunt.
However, there is no consensus regarding the best parameters to evaluate reversibility of PH. Therefore, this must include a multi-dimensional approach, bridging together clinical, imaging, and hemodynamic variables.3‐6
Our patient presented several criteria considered to be a contraindication for ASD closure: presence of spontaneous bidirectional shunt with slight desaturation in CPET and RHC showing severe PH with negative vasoreactivity test.
In patients with irreversible PH, PVT is reported to have beneficial effects, reducing pulmonary vascular resistance, and improving functional capacity.3–6 The maximum dosage of these drugs should be achieved to obtain the greatest benefit possible. In our case, bosentan and sildenafil were the treatment of choice, the latter being used at a dose higher than the recommendend by ESC guidelides, since its benefit seems to be dose-related. 7
Until recently, this was the only therapy offered to these pts. However, PVT by itself could lead to an unavoidable increase in interatrial shunt, leading to RV overload and worsening pulmonary vascular disease.2,5 In these cases, the combination of PVT with a fenestrated patch occlusion of the ASD might be an extraordinary solution, limiting right-to-left shunt and also providing a stable outlet to unload RV in case of pulmonary artery pressure rising or PH crisis.2,5 This is, indeed, corroborated by the recent publication of Yan et al, in JACC: Cardiovascular Interventions, which is the first cohort confirming the benefit of combined therapy with PVT and ASD closure.2,5
Our patient experienced an incremental improvement in exercise capacity and in cardiac remodeling after ASD closure, which is in line with the more recent data in literature.
In conclusion, closing ASD in patients with severe PH is increasingly becoming a successful reality, as long as patient's selection is judicious and individualized. Further studies are necessary to evaluate the long- term impact of these interventions.
Footnotes
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for Publication
The patient's consent for publication was obtained.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.