
Abstract
Inhaled corticosteroids are widely used in the treatment of chronic obstructive pulmonary disease (COPD). However, their use has been questioned for appropriate dose and a possible increased risk of pneumonia. Here, we reviewed patients with COPD who had received fluticasone–salmeterol combination treatment using data from a linked electronic medical record database. A total of 180 patients received salmeterol with 250 µg fluticasone propionate twice daily and 78 received salmeterol and 100 µg fluticasone propionate twice daily. In both groups, there was no difference in the improved forced expiratory volume in 1 second and COPD assessment test score and the proportion of patients with exacerbations. Although the incidence of common toxicity was approximately equal, that of pneumonia was much higher in the 250 µg group (8.9% vs 1.3%, P=.01). The beneficial effects of inhaled corticosteroids might be obtained at lower doses.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide. 1 It is characterized by airflow limitation and is commonly associated with accelerated lung function decline over time.2–5 At present, pharmacotherapy with inhaled bronchodilators, anticholinergics and β 2 agonists, alone or in combination, is the mainstay of COPD treatment,2,3 and inhaled corticosteroids are also widely used. In a landmark study, Towards a Revolution in COPD Health (TORCH), combination treatment with fluticasone–salmeterol was shown to improve pulmonary function, symptoms, and health status and reduce exacerbations. 6 Because exacerbations accelerate lung function decline, cause a deterioration in health status, and increase the risk of death,4,7–9 preventing them is a priority. A systematic review using the Cochrane Airways Group Specialized Register concluded that inhaled corticosteroids reduced the rate of exacerbation and deterioration in quality of life. 10 In consensus guidelines, inhaled corticosteroids are particularly recommended in severe cases of COPD with a history of exacerbations.3–5
The use of inhaled corticosteroids for COPD treatment has been increasing in recent years, 11,12 but concerns have been raised. First, the dose–response relationship of inhaled corticosteroids remains unknown in COPD. In the treatment of asthma, the efficacy of inhaled corticosteroids is dose-dependent and the dose of the corticosteroid is chosen according to disease severity. Although 500 µg fluticasone propionate in combination with 50 µg salmeterol in a single inhaler twice daily is commonly used for COPD worldwide, few studies have systematically investigated appropriate doses for this indication. A meta-analysis of 7 randomized trials reported that treatment with inhaled corticosteroids led to a 25% reduction in all-cause mortality, 13 but fluticasone propionate equivalent doses ranged from 400 to 1000 µg/d and no dose–response relationship was apparent. In addition, some clinical studies have demonstrated improvements in lung function, symptom control, and exacerbations by adding inhaled corticosteroids at a lower dose, equivalent to 250 µg fluticasone propionate.14–16 It is possible that even lower doses of fluticasone propionate will be effective in the treatment of COPD.
Second, the safety of inhaled corticosteroids in COPD remains debated. Long-term treatment with inhaled corticosteroids has been associated with side effects in patients with COPD. In particular, the risk of pneumonia has been the focus of research attention. In randomized controlled trials, fluticasone–salmeterol has been linked with increases in the incidence of pneumonia compared with alternative bronchodilator regimens.6,17 A large observational study identified an increase in the incidence of hospitalizations for pneumonia and of pneumonia hospitalization followed by death within 30 days. 18 There was a correlation between the dose of inhaled corticosteroids and the risk of pneumonia, with a high rate of pneumonia in those taking high-dose inhaled corticosteroids, equivalent to fluticasone propionate at 1000 µg/d or more. In particular, there was a dose-dependent risk of pneumonia in COPD patients treated with fluticasone propionate.19,20 It is therefore important to examine the efficacy and safety of low-dose fluticasone propionate in combination with salmeterol in patients with COPD.
In Japan, patients receive twice daily fluticasone–salmeterol at 2 different doses, 100 or 250 µg (usual dosage provided in the package insert in Japan), at the discretion of the treating physician. We hypothesized that lower doses of inhaled fluticasone with salmeterol will show similar efficacy to usual dosage of fluticasone propionate. Here, we retrospectively compared the efficacy and safety of these 2 doses of fluticasone propionate in combination with salmeterol twice daily.
Methods
Study design and patients
This was a retrospective observational study conducted in accordance with the ethical standards described in the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Hamamatsu University School of Medicine (certificate #25-302). Because of the retrospective manner of the study, written consent from participants for use of records was waived. All patient records/information were anonymized and de-identified prior to analysis. The study was registered with the University Hospital Medical Information Network Clinical Trial Registry (UMIN ID000013490).
Using linked electronic medical records from 2011 and 2012, we obtained data from patients with COPD who had received fluticasone–salmeterol combination (dry powder inhaler) treatment for 1 year and had undergone examinations before treatment and after 1 year of treatment. Diagnosis and classification of COPD were based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2011 classification. 4 Bronchial asthma was strictly excluded by pulmonary specialists.
Measurement of pulmonary function
Pulmonary function tests (forced vital capacity [FVC], forced expiratory volume in 1 second [FEV1], and inspiratory capacity) were performed using an electric spirometer. FEV1 was expressed as a percentage of predicted values according to the prediction equations of the Japanese Respiratory Society. 21 Symptoms and health status were assessed using the COPD assessment test (CAT).
Definition of exacerbation and pneumonia
The COPD exacerbations were defined as events that required additional pharmacological treatment (systemic glucocorticoids, antibiotics, or both).4,6,22 Diagnosis of pneumonia was based on new-onset respiratory symptoms and infiltration on chest X-ray or computed tomography.
Statistical analysis
The Wilcoxon matched-pair signed-rank test and Mann–Whitney U test were used for continuous variables, and the chi-square test was used for categorical groups. Data are presented as number (percentage) or median (range). Univariate and multivariate logistic regression analyses were performed to identify the risk factors for developing pneumonia. JMP9.0.0 (SAS Institute Japan, Tokyo, Japan) was used for statistical analysis and P < .05 was considered significant.
Results
Patient characteristics
A total of 372 patients with COPD received fluticasone–salmeterol inhaler. Among them, 258 patients completed examinations before treatment and after 1 year of treatment. The median age was 76 (47-94) years. All patients had a history of smoking (median pack-year, 50.0) and 36 patients (14.0%) were current smokers. The median predicted FEV1 was 56.1% (20.0%-143.2%). The percentages of patients at GOLD classification stages I, II, III, and IV were 7.7%, 51.2%, 32.2%, and 8.9%, respectively. The CAT score was 13 (1-35). Sixty-nine patients (26.7%) had a history of exacerbation during the previous year. The proportions of the GOLD combined COPD assessment grades consisting of symptoms, airflow obstruction, and exacerbation history based on 2011 GOLD report 4 were 52 (20.2%) in grade A, 109 (42.2%) in grade B, 20 (7.8%) in grade C, and 77 (29.8%) in grade D. Two hundred (77.5%) patients had also received a long-acting muscarinic antagonist.
Among 258 patients receiving fluticasone–salmeterol, 180 (70.0%) received fluticasone propionate at a dose of 250 µg twice daily (fluticasone 250 µg group) and 78 patients (30.0%) received fluticasone propionate 100 µg twice daily (fluticasone 100 µg group). Table 1 shows the characteristics of patients in each group. Baseline smoking habits, pulmonary function tests, and CAT score were comparable between the 2 groups. Approximately a quarter of patients in each group had a history of exacerbations in the previous year.
Patient characteristics.
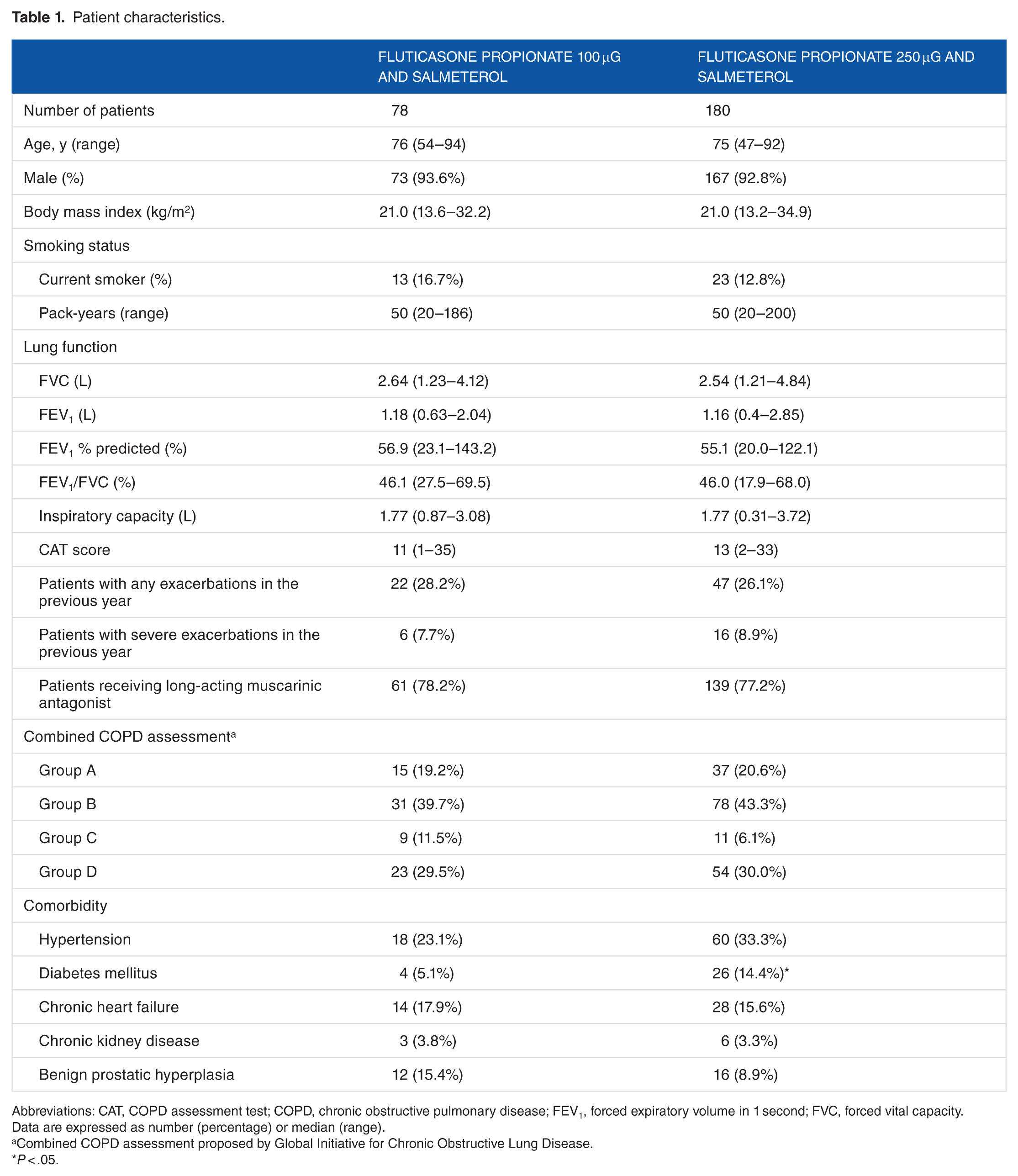
Abbreviations: CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
Data are expressed as number (percentage) or median (range).
Combined COPD assessment proposed by Global Initiative for Chronic Obstructive Lung Disease.
P < .05.
Lung function and COPD control according to fluticasone dose
Treatment with either dose of fluticasone in combination with salmeterol improved FEV1 and CAT (Table 2). There was no inspiratory capacity change in either treatment group. During the 12-month period, approximately equal numbers of patients experienced exacerbations in the 2 groups (35.0% in the 250 µg group and 28.2% in the 100 µg group, P = .22). The percentages of patients with more than 2 exacerbations per year were 12.2% in the 250 µg group and 7.7% in the 100 µg group with no significant difference between them. There was also no difference in the proportion of patients with severe exacerbations between the 2 groups (9.4% in the 250 µg group and 9.0% in the 100 µg group, P = .67). There was no death in the 2 groups during the observation period.
Pulmonary function and COPD assessment test scores before and after combination treatment with fluticasone propionate and salmeterol.
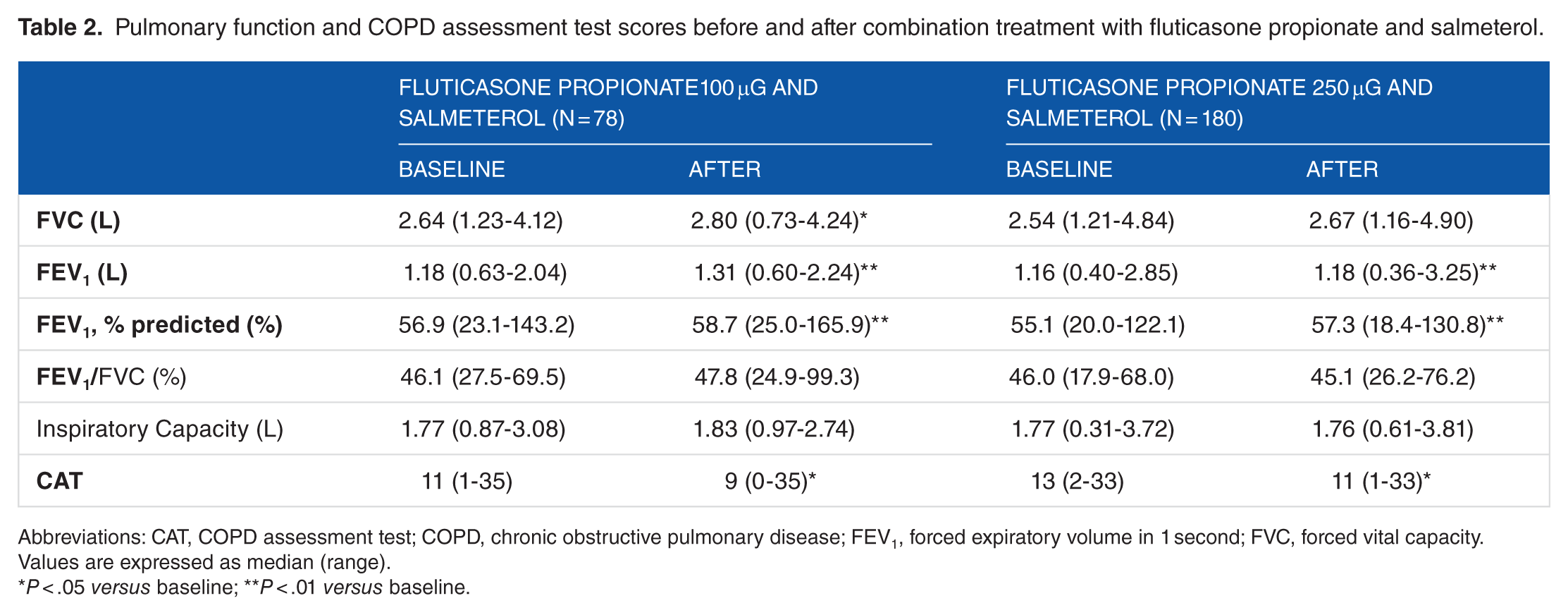
Abbreviations: CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
Values are expressed as median (range).
P < .05 versus baseline; **P < .01 versus baseline.
Adverse events
Major adverse events are shown in Table 3. Incidence of any adverse event in the 250 and 100 µg groups were 22.2% and 18.0%, respectively. The most common toxicity was oral cavity or pharynx problems and the incidence of both was approximately equal. The incidence of lower respiratory tract infection was much higher in the 250 µg group than in the 100 µg group (9.4% vs 1.3%, P < .01). During the follow-up period, fluticasone treatment was withdrawn in 5 patients (6.5%) in the 100 µg group and 9 (6.4%) in the 250 µg group due to oral cavity problems. In addition, fluticasone was withdrawn in 7 patients (3.9%) in the 250 µg group after development of pneumonia, meaning a total of 16 patients discontinued treatment with fluticasone in this group. Univariate logistic regression analysis was carried out to estimate the predictive factors for the development of pneumonia using patient characteristics, spirometric data, and treatment as the variables (Table 4). A low body mass index (BMI < 20) and the use of fluticasone propionate 250 µg were significantly associated with pneumonia development (odds ratio, 5.10; 95% confidence interval [CI], 1.75-18.5; P < .01, odds ratio, 7.51; 95% CI, 1.49-136.7; P = .01, respectively).
Adverse events during treatment with fluticasone propionate and salmeterol.
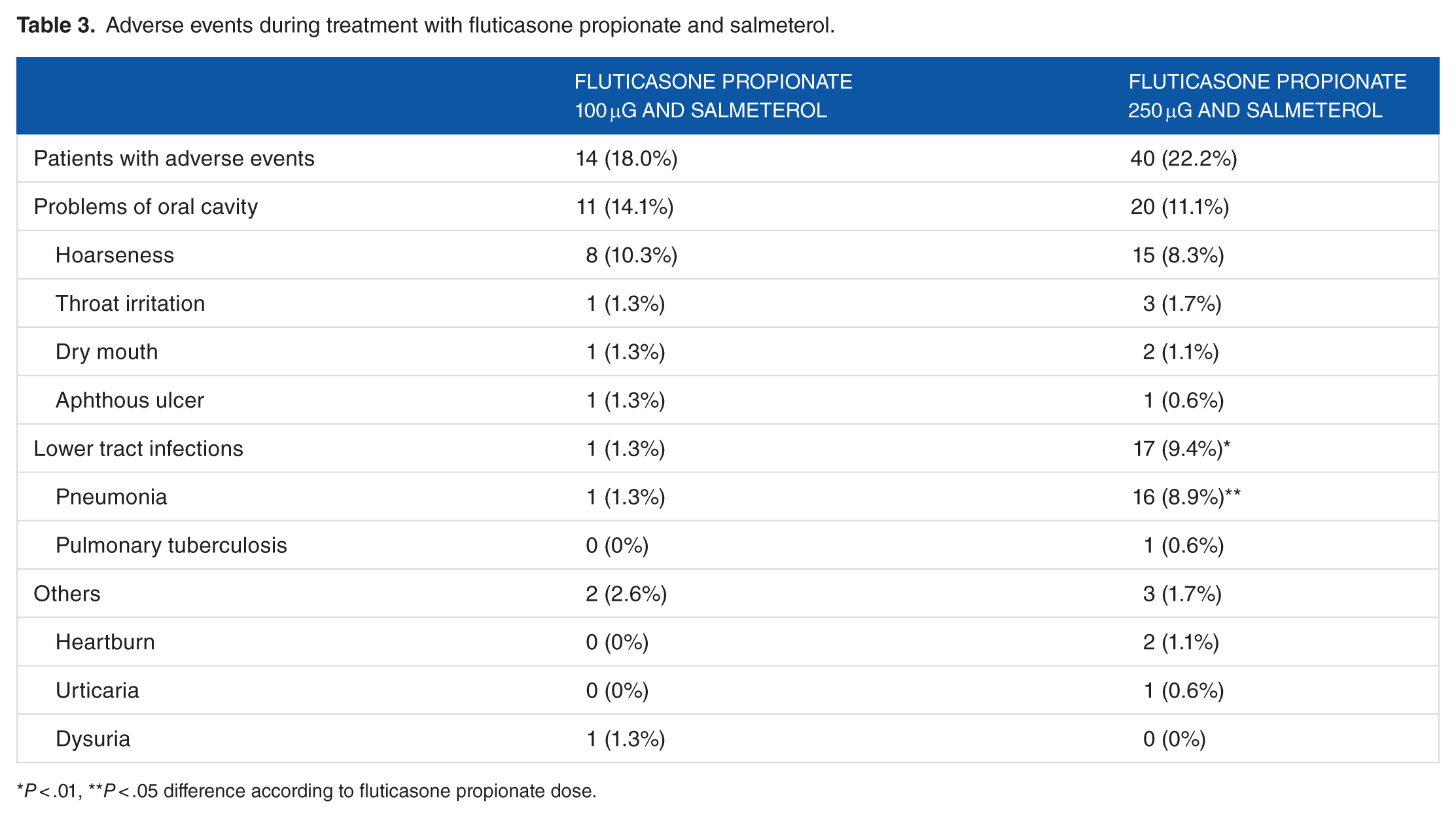
P < .01, **P < .05 difference according to fluticasone propionate dose.
Univariate and multivariate logistic analyses of risk factors for developing pneumonia.
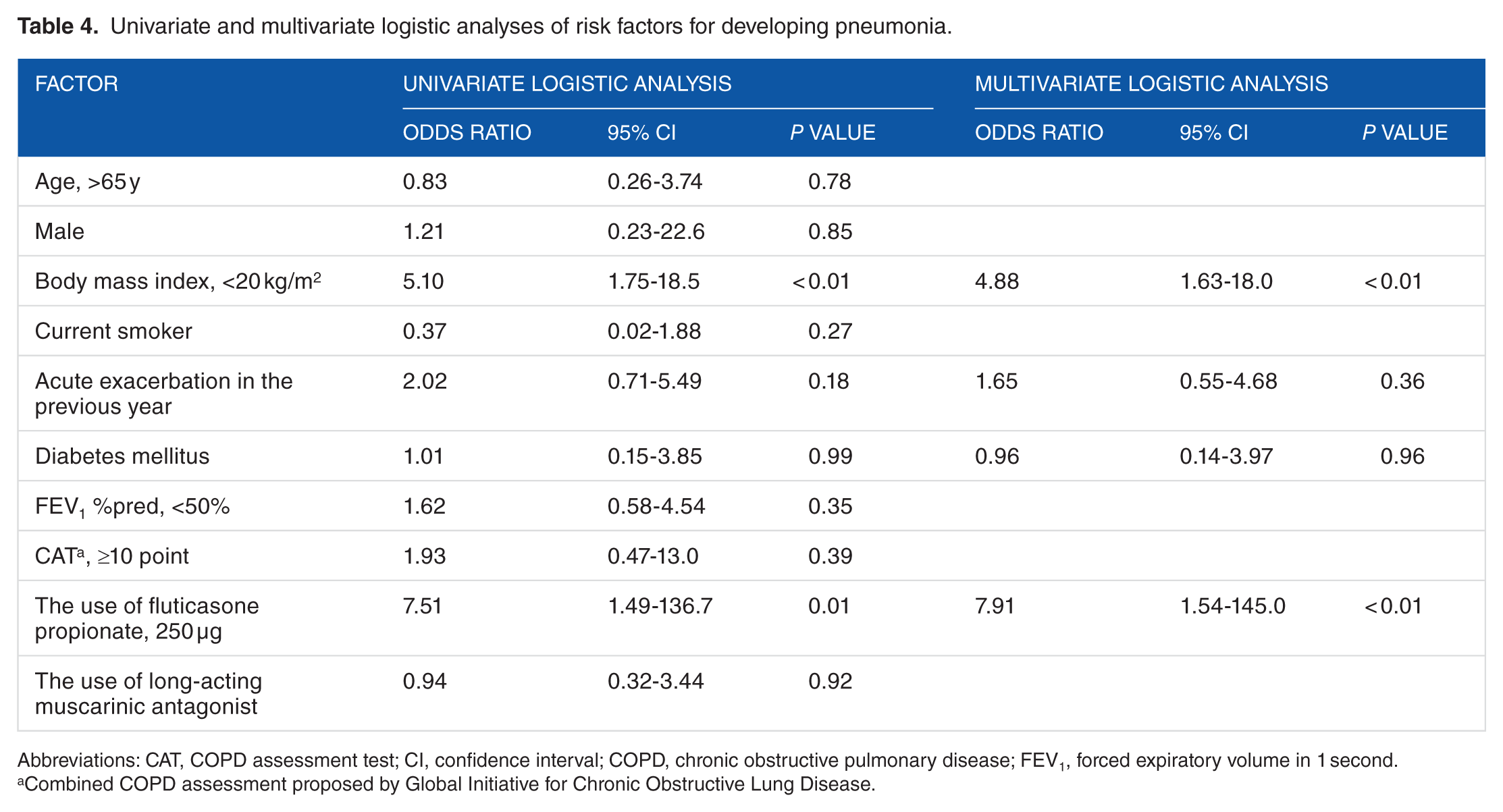
Abbreviations: CAT, COPD assessment test; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second.
Combined COPD assessment proposed by Global Initiative for Chronic Obstructive Lung Disease.
Discussion
In the present study, treatment with 250 and 100 µg fluticasone propionate in combination with salmeterol twice daily improved pulmonary function, symptoms, and health status. There was no significant difference in frequency of exacerbations between the 2 doses of fluticasone. However, patients in the 250 µg group experienced pneumonia more frequently. Although this study did not determine the implications of using inhaled corticosteroids in COPD treatment, it suggests that the beneficial effects of inhaled corticosteroids might occur at even lower doses than those currently used.
Most COPD treatments target bronchodilation, with the aim of relieving bronchoconstriction and improving respiratory distress and exercise tolerance.2–5 However, this strategy does not increase survival. 6 In contrast with bronchial asthma, airway inflammation in COPD is mainly due to neutrophil inflammation, not eosinophil inflammation, which reduces the benefits of corticosteroids in COPD treatment. 22 At present, addition of inhaled corticosteroids to long-acting bronchodilators is recommended for patients at high risk of exacerbations and with a history of frequent exacerbation events and severe obstructive respiratory events.4,5 However, the use of inhaled corticosteroids in COPD is controversial. Recently, continued use of inhaled corticosteroids was evaluated in 2485 patients with severe or very severe COPD. 23 In this Withdrawal of Inhaled Steroids during Optimized Bronchodilator Management (WISDOM) trial, patients received triple therapy with tiotropium, salmeterol, and 500 µg fluticasone twice daily. They were then randomly assigned to withdrawal from fluticasone or continuation of triple therapy to determine the effects of the inhaled corticosteroid. The reduction in trough FEV1 was greater in the withdrawal group at week 18 when fluticasone withdrawal was completed. However, the risk of moderate or severe exacerbations was comparable between both groups. In another study, which investigated the effect of switching from combined fluticasone propionate 500 µg and salmeterol 50 µg twice daily to indacaterol monotherapy, there was no efficacy loss for trough FEV1 or exacerbation rate. 24 As for the combination of a long-acting anticholinergic and a β2 agonist, the Effect of Indacaterol Glycopyronium Vs. Fluticasone Salmeterol on COPD Exacerbations (FLAME) trial showed the combination of indacaterol and glycopyrronium was more effective than salmeterol and 500 µg fluticasone in reduction of the annual exacerbation rate. 25 Regarding safety, Suissa et al evaluated health insurance databases and showed that discontinuation of inhaled corticosteroids reduced the elevated risk of severe pneumonia. 18 Risk reduction by discontinuing inhaled corticosteroids was 37%, and this was more significant in cases with fluticasone. Taking into account the clinical risk–benefit profile of fluticasone, it may be advisable to discontinue fluticasone therapy in COPD.
However, adding inhaled corticosteroids to bronchodilator might nevertheless contribute certain benefits, such as preventing exacerbations and slowing pulmonary function decline .6,10,26,27 In COPD, pneumonia is much less common than exacerbations. 28 Despite the increased risk of pneumonia, the use of inhaled corticosteroids is not associated with all-cause mortality, which might suggest that their adverse effects are not observed consistently. 18 Indeed, some subsets of patients with COPD, such as those with blood eosinophilia 29 or asthma–COPD overlap syndrome, might respond well to inhaled corticosteroids. And there is the possibility that even lower doses of inhaled corticosteroids may provide therapeutic benefit without increasing the risk of pneumonia, as this was related to the daily dose of inhaled corticosteroid. In a retrospective cohort analysis using claims databases, the incidence of pneumonia with low (1-499 µg), medium (500-999 µg), and high (>1000 µg) doses of inhaled corticosteroids (doses equivalent to daily fluticasone propionate) was 0.150, 0.247, and 0.319, respectively. 20 Although fluticasone 500 µg in combination with salmeterol 50 µg twice daily is widely used for treating COPD, few trials have investigated appropriate doses for this indication. Some clinical studies used inhaled corticosteroids at 250 µg,14–16 but the efficacy and safety of 100 µg fluticasone propionate remained unclear. We therefore evaluated the benefit of lower doses of fluticasone propionate in the present retrospective study. There were no significant differences in lung function, health status, or exacerbations between the 100 and 250 µg doses of fluticasone propionate examined in the present study. The incidence of pneumonia in patients receiving 250 µg fluticasone propionate was 8.9%, almost identical to that reported in previous studies.14–16 Conversely, the risk of pneumonia was much lower in patients receiving 100 µg fluticasone propionate.
Crim et al 30 identified risk factors for pneumonia in a post hoc analysis of the TORCH study. Older age (>55 years), lower predicted FEV1 (<50%), exacerbation(s) in the preceding year, worse dyspnea score, and lower BMI (<20) were significantly associated with the probability of pneumonia. In the present study, logistic regression analyses were performed using similar factors and BMI < 20 and the use of fluticasone propionate 250 µg were significantly associated with the development of pneumonia in univariate and multivariate analyses.
This was a retrospective study and there were a number of confounding factors. The dose of fluticasone propionate was selected at the discretion of the treating physicians, which can induce bias as more severe cases tend to receive larger doses. Furthermore, the diagnosis of pneumonia was important in this retrospective study. To date, many clinical trials have demonstrated that patients receiving inhaled corticosteroid-containing treatments had an increased risk of pneumonia.17–20,27,28,30 But in most of those studies, the objective definitions of pneumonia were not determined and the diagnosis was defined clinically, not radiographically.17–20,27,30 Pneumonia has a high degree of clinical overlap with COPD exacerbations. Without a chest radiograph, it can be difficult to distinguish between pneumonia and exacerbation. 28 In the present study, we confirmed pneumonia using a chest X-ray or computed tomography. Our study showed that patients receiving a higher dose of fluticasone propionate developed a higher percentage of radiographically confirmed pneumonia in comparison with patients using a lower dose of fluticasone propionate. Second, because we included only patients receiving fluticasone–salmeterol combination inhaler, the effect of other inhaler corticosteroids remains unclear. Improvements in pulmonary function might be solely due to use of salmeterol in both groups. Third, this study did not determine the validity and implications of using inhaled corticosteroids in COPD treatment. Considering the GOLD combined COPD assessment grades, a large proportion of included patients did not have an indication for inhaled corticosteroids. This was a retrospective study without defined treatment protocol, which might reflect real-world clinical practice. Price et al 12 reported that inhaled corticosteroids were widely prescribed outside guideline recommendations in the United Kingdom.
Conclusions
Treatment with 100 µg fluticasone propionate in combination with salmeterol showed similar improvements in pulmonary function, symptoms, and health status to 250 µg fluticasone propionate, but the risk of pneumonia was lower in patients receiving the lower dose. Although it was a retrospective analysis with confounding factors, these results warrant further investigation in prospective trials to evaluate the effect and safety of low-dose inhaled corticosteroids, such as 100 µg fluticasone propionate, in the treatment of COPD.
Footnotes
Author Contributions
HY, NI, and TS conceived and designed the experiments. HY, TF, MK, and NE analyzed the data. HY, NI, and TS wrote the first draft of the manuscript. YN, SK, HO, KY, JS, MS, NK, MT, TY, MM, and TS contributed to the writing of the manuscript. All authors agreed with manuscript results and conclusions, reviewed, and approved the final manuscript.
Disclosures and Ethics
The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.