
Abstract
Background
Hyperkalemia is one of the more common acute life-threatening metabolic emergencies. Although only a small proportion of cases progress to cardiac arrest (CA), early detection and timely intervention often yield excellent outcomes. Dynamic and characteristic ECG manifestations combined with point-of-care testing (POCT) potassium management provide timely evidence for hyperkalemia treatment. Wide QRS complex rhythms blended with T waves are extremely high-risk signals for CA due to hyperkalemia.
Case Presentation
We report a 68-year-old male patient who presented to the hospital with syncope. ECG findings included peaked T waves, loss of P-waves, sinoventricular conduction, and a wide QRS complex rhythm. Shortly after admission, the patient experienced CA. POCT potassium levels were 9.0 mmol/L. With the help of ECG and POCT potassium results, the patient achieved return of spontaneous circulation (ROSC) after 32 minutes of CPR without residual neurological deficits.
Conclusion
This paper highlights the role of dynamic ECG monitoring and POCT potassium management in rescuing patients with lethal hyperkalemia.Through POCT potassium monitoring, identification of high-risk ECG signals, combined with effective pharmacological intervention and high-quality CPR, the success rate of rescue treatment can be significantly improved, and patient prognosis can be enhanced.
Introduction
Hyperkalemia is one of the more common acute life-threatening metabolic emergencies, 1 occurring in up to 0.33% to 3% of emergency department patients.2,3 It is point out that only a very small proportion (almost 2.25%) hyperkalemia patients complicating with cardiac arrest (CA). 2 Kose et al 4 review 10 cases of CA caused by hyperkalemia and found serum potassium levels ranging from 8.3-11.4 mmol/l. Hyperkalemia is a condition for which early detection and timely intervention often yield excellent results, whereas delayed treatment can lead to severe consequences.4-6 Electrocardiogram (ECG) a cornerstone in the management of hyperkalemia. 1 Point-of-care testing (POCT) potassium is important for providing timely blood potassium results. Combining POCT potassium with ECG is an effective tool to provide timely evidence for clinical decision. This article reports an interesting case of recurrent lethal hyperkalemia that was successfully managed through dynamic ECG and POCT potassium monitoring, particularly during cardiopulmonary resuscitation (CPR). The aim is to enhance understanding of the dynamic and characteristic ECG manifestations in hyperkalemia and the role of ECG alongside POCT potassium monitoring in therapeutic management.
Case Presentation
We present the case of a 68-year-old male patient presented to the emergency department after experiencing three episodes of syncope over the preceding three hours, each lasting a few seconds and resolving spontaneously, associated with cough, sputum production, and dyspnea, but without chest pain. The patient had a history of hypertension and diabetes for several decades, as well as cerebral infarction for over 7 years. He also had a sleep disorder for more than 1 year and was taking Estazolam orally at two tablets once daily. He underwent lower limb amputations in 2024 and 2025 due to diabetic foot and percutaneous coronary intervention three times, in 2022, 2023, and 2025, respectively. For the past 2 years, he had been undergoing hemodialysis three times per week for end-stage chronic kidney disease. His last dialysis was performed 2 days before admission. Notably, despite his dietary restrictions for end-stage renal disease, he had consumed a significant amount of passion fruit—a potassium-rich food—the day prior to admission.
Physical examination at admission revealed blood pressure (BP) 172/103 mmHg, heart rate (HR) 72 bpm, and respiratory rate (RR) 20 breaths/min with 96% peripheral capillary oxygen saturation (SpO2) in room air. Both lungs were clear to auscultation with no obvious rales, and the heart sounds were normal. The admission ECG showed loss of P-waves, sinoventricular conduction, and a wide QRS complex rhythm blended with T waves (Figure 1A). Shortly after admission (at 14:00), the patient experienced CA. ECG monitoring showed ventricular fibrillation (VF); immediate active CPR was initiated, including chest compressions, endotracheal intubation, defibrillation, and administration of epinephrine and 5% sodium bicarbonate (250ml). Femoral artery pulsations were detected at 14:11, but the patient subsequently experienced CA again approximately 10 seconds later. Point-of-care testing (POCT) serum potassium was 9.0 mmol/L. Therefore, pharmacological treatment for hyperkalemia was administered intravenously, consisting of 10 mL of 10% calcium gluconate, 8 U of regular insulin with 500 mL of 10% dextrose, and 200 mg of furosemide, to antagonize hyperkalemia and promote intracellular potassium influx. Seventeen minutes later, POCT potassium decreased to 6.5 mmol/L. VF was still present on ECG. Ultimately, after a total of 7 defibrillations and administration of amiodarone for antiarrhythmic support, return of spontaneous circulation (ROSC) occurred at 14:32. Subsequently, ventricular tachycardia (VT) occurred three times and was treated with 100J synchronized cardioversion. By 14:51, no further VT episodes were noted; the patient regained consciousness, with pupils that were reactive to light, an HR of 61 bpm, and BP of 160/71 mmHg. Extracorporeal membrane oxygenation was suggested during CPR but not performed due to delayed family consent. POCT potassium and ECG findings are shown in Table 1 and Figure 1B-E. Continuous renal replacement therapy (CRRT) was initiated at 16:15 and continued until 23:30. During CRRT, ECG monitoring showed sinus arrest with ventricular escape rhythm at an HR of 35 bpm, but serum potassium levels were normal (Figure 1F). ECG manifestations at different time points. (A) On initial admission, ECG showed an HR of 53 bpm, QRS duration of 205 ms, QTc time of 397 ms, loss of P-waves, sinoventricular conduction, spiked T wave, ST depression in lead I, II, and V4-V6, and a wide QRS complex rhythm blended with T wave. During CPR, ECG showed VF (B), PEA with an HR of 24 bpm (C), and wide complex polymorphic VT (D). (E) 20min after CPR, ECG showed an HR of 60 bpm, loss of P-waves, sinoventricular conduction. (F) During CRRT, ECG showed sinus arrest and ventricular escape with HR 35 bpm, but serum potassium levels were normal. (G) The following morning, ECG showed sinus bradycardia with an HR of 54 bpm, QRS duration of 132 ms, QTc time of 530 ms, I°AVB, intraventricular block, spiked T waves, ST depression in leads II, aVF, and V4-V6. (H) During CRRT in the following evening, the ECG showed an HR of 85 bpm, QRS duration of 102 ms, QTc time of 500 ms, spiked T waves, ST depression in leads II, aVF, and V4-V6. (I) On subsequent time admission, ECG showed an HR of 23 bpm, QRS duration of 148 ms, QTc time of 429 ms, sinus arrest, and ventricular escape. (J) One hour after treatment, the ECG showed sinus bradycardia with an HR of 46 bpm, QRS duration of 100 ms, QTc time of 446 ms, and I°AVB. ECG: electrocardiogram; HR: heart rate; CPR: cardiopulmonary resuscitation; VF: ventricular fibrillation; PEA: pulseless electrical activity; VT: ventricular tachycardia; CRRT: continuous renal replacement therapy; I°AVB: first-degree atrioventricular block Key Time Points for Serum Potassium and ECG
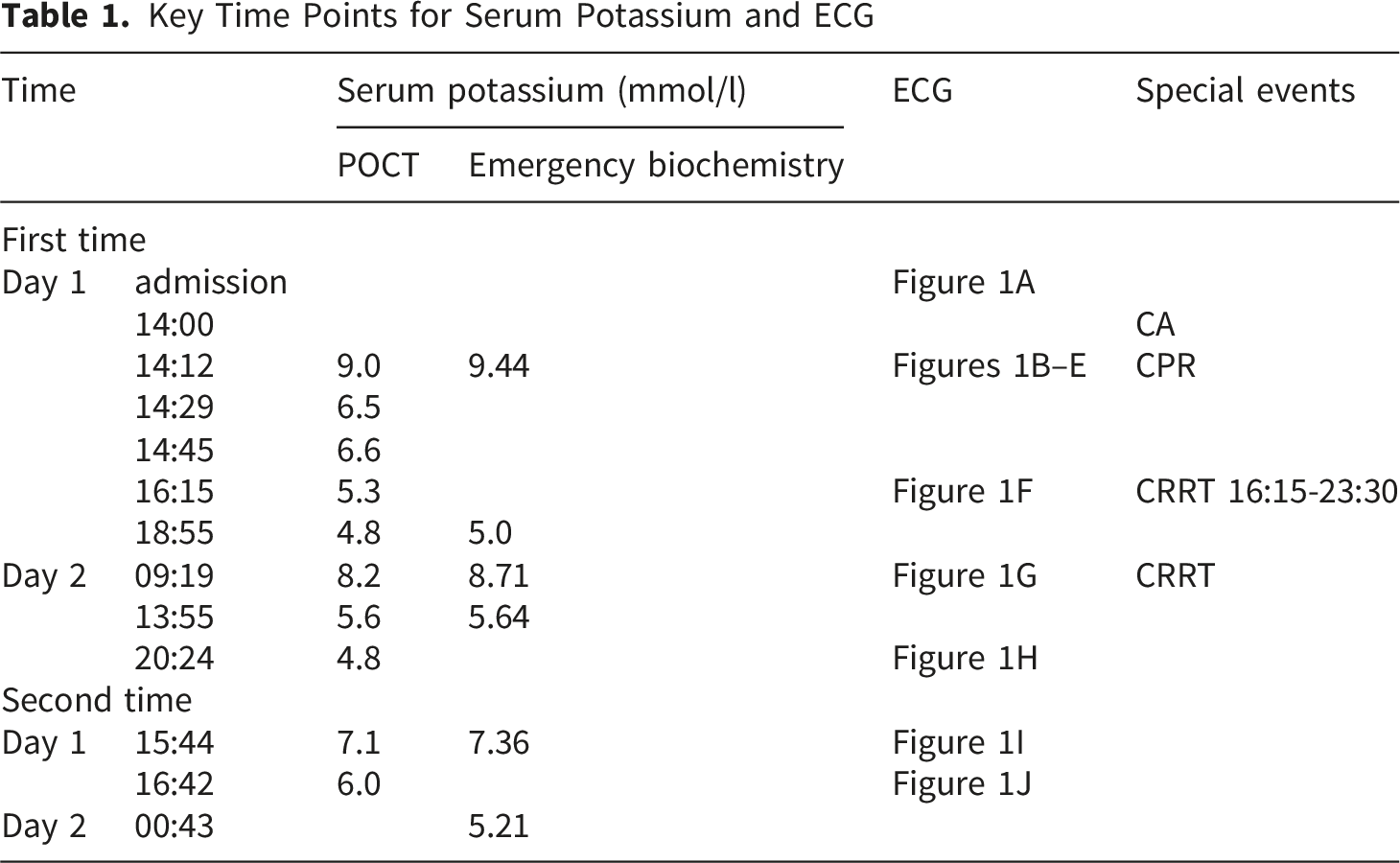
Surprisingly, POCT serum potassium increased to 8.2 mmol/l the following morning, and ECG showed sinus bradycardia with an HR of 54 bpm, QRS duration of 132 ms, QTc interval of 530 ms, and ST-segment depression in leads II, aVF, and V4-V6 (Figure 1G). The patient received subsequent hospitalization with CRRT, potassium-lowering medications, and supportive treatment. Later that evening, during CRRT, ECG showed HR increased to 85 bpm, QRS duration decreased to 102 ms, and QTc time decreased to 500 ms (Figure 1H), with normal POCT potassium. The patient improved and was discharged after 6 days.
Unfortunately, fifty days later, the patient was readmitted due to dizziness and weakness lasting for 1 hour. Physical examination at admission revealed an HR of 23 bpm, BP of 116/65 mmHg, and respiratory rate of 26 times/min with moderate distress. The pulse was very weak and thready, and cardiac auscultation demonstrated weak heart sounds. An ECG was performed immediately, showing loss of P-waves with an HR of 23 bpm (Figure 1I), and POCT potassium was measured at 7.1 mmol/l (Table 1). Immediate potassium-lowering treatment, including 10 mL of 10% calcium gluconate, 125 mL of 5% sodium bicarbonate, 6 U of regular insulin with 50 mL of 50% dextrose, and 100 mg of furosemide, was administered intravenously, and 10 g of sodium zirconium cyclosilicate was administered orally. One hour later, serum POCT potassium had decreased to 6.0 mmol/l, and the ECG showed reappearance of P-waves with HR increasing to 44 bpm (Figure 1J). The patient was discharged after potassium levels normalized. Post-discharge, hemodialysis frequency was increased to four times per week. In addition, potassium-rich foods such as oranges, bananas, and passion fruit should be limited. To date, the patient has had no further admissions for hyperkalemia.
Discussion
Hyperkalemia is one of the more common acute life-threatening metabolic emergencies, 1 it can cause serious complications such as cardiac arrhythmias, muscle weakness, and CA. 7 Lind et al 8 studied 6,658 hospitalized patients with abnormal potassium levels in Denmark from 2017 to 2021, and showed that the incidence of in-hospital CA was found to be 13.13-fold higher in patients with severe hyperkalemia (K+ > 6.5 mmol/l) compared with patients with normal serum potassium concentrations. The severity of hyperkalemia is not solely determined by the serum potassium value, but also by the speed of onset, sex, age, comorbidities, clinical symptoms, and ECG abnormalities.5,9-12 Generally, in patients with hyperkalemia, the typical ECG changes such as peaked T waves and widening of QRS complexes often precede symptoms or signs.5,9 The type of ECG changes is a more important predictor of outcome than the actual potassium level. 10 Therefore, the severity assessment of hyperkalemia as followed: clinical symptoms (such as: CA, shock, syncope); ECG abnormalities; serum potassium value; etc. In our patient, on the second admission, although ECG manifestations were significantly abnormal, clinical symptoms were milder and no CA occurred. This can explain the importance of cardiovascular symptoms in predicting CA caused by hyperkalemia.
ECG can be the most immediately available diagnostic tool for identifying patients with potentially lethal hyperkalemia. 10 Although there is a lack of consensus regarding the role of ECG in the diagnosis and treatment of hyperkalemia, ECG changes are core reflections of its severity, directly indicating the degree of electrophysiological disturbance in myocardial cells. 1 ECG serve as a crucial basis for clinically assessing disease progression and prognosis. Hyperkalemia can cause various characteristic ECG changes, including but not limited to peaked T-waves, shortened QT interval, lengthening of PR interval, QT interval, and QRS duration, loss of P-waves, and various arrhythmias such as atrioventricular blocks (AVB), bradycardia, VT, and VF.1,3,9,13 Rafique et al 1 studied 96 patients with end-stage renal disease to determine the correlation and accuracy of abnormal ECG parameters as a function of serum potassium, and found that a QRS duration of 120 ms or greater is most predictive of hyperkalemia. Azuma et al 5 studied hyperkalemia-induced ECG abnormalities in bullfrog hearts and showed that a widened QRS complex is associated with the highest concentration of serum potassium. Peaking of the T waves, the most widely appreciated ECG sign, is actually rarely a manifestation of life-threatening hyperkalemia. 10 The loss of P-waves suggests severe inhibition of atrial myocardial excitability, also known as sinoventricular conduction. This is because the atrial myocardium is more sensitive to hyperkalemia than the ventricular myocardium.11,14 Importantly, wide QRS complex rhythm blended with T wave harbingered impending VF and asystole. 6 Hence, it is crucial to recognize that the ECG in Figure 1A implies extremely high-risk signals for CA.
Although cardiovascular instability typically occurs at potassium levels > 8 mmol/l, 13 ECG changes of hyperkalaemia did not correlate with serum potassium levels.1,3,11 This variability may be related to underlying diseases (such as chronic renal insufficiency, which confers greater tolerance to high potassium), the rate of potassium increase, and individual myocardial sensitivity. In this case, during the first CRRT session after CPR, the ECG showed sinus arrest and ventricular escape with an HR of 35 bpm, despite serum potassium having already returned to normal at that time. This may be attributed to myocardial stunning caused by hyperkalemia. This was supported by the next morning’s serum potassium level (K+ = 8.2 mmol/l), which may be associated with the release of intracellular potassium. The decrease in potassium levels by 2.5 mmol/l within 20 minutes during CPR indicated significant potassium influx into cells. Another notable finding was the patient’s readmission due to hyperkalemia, which was accompanied by ECG abnormalities. These findings underscored the importance of dynamic monitoring of blood potassium levels and the ECG.
POCT potassium can significantly reduce turnaround time without compromising the quality. 15 In our hospital, central laboratory serum potassium testing requires a waiting period of 0.5 to 2 hours, whereas POCT potassium can yield results in approximately 1 to 3 minutes. Je SY et al 16 studied 1188 chronic kidney disease patients with suspected hyperkalemia, and found that high levels of reliability between POCT and laboratory tests (intra-class correlation coefficient 0.913, 95% confidence interval 0.903--0.922). Notably, some studies did not find the same conclusion, which accounts for 3.6-70% of cases of pseudohyperkalemia.15,17 Pseudohyperkalemia has resulted in the improper administration of potassium-lowering treatments (such as insulin) in individuals with normal potassium levels. 17 Hence, although POCT is crucial for directing prompt, life-saving treatment when there are corresponding high-risk ECG changes (as was skillfully done in this case), it is generally advised to verify POCT results with central laboratory testing when time permits, especially if POCT reveals severe hyperkalemia but the patient does not exhibit corresponding clinical symptoms or ECG abnormalities.
Although clinical evidence supporting the administration of calcium or sodium bicarbonate in humans is limited and their efficacy in improving survival or favorable neurological outcomes in patients with hyperkalemia-induced CA remains uncertain, 18 hyperkalemia is a condition for which timely intervention often yields excellent results. Effective pharmacological interventions can lower potassium levels within minutes to hours. 19 Ngugi et al 20 showed that the combination of insulin with glucose and salbutamol caused a rapid onset of action and a significant decrease (1.09 ± 0.58 mmol/l) in the serum potassium within the first 30 minutes. Although salbutamol was not utilized in our case, our patient’s rapid 2.5 mmol/L decrease within 20 minutes was likely achieved through a combination of insulin/dextrose, furosemide, and the mechanical promotion of intracellular potassium influx via chest compressions.
At last, the patient in our case was successfully resuscitated after 32 minutes of CPR without residual neurological deficits. This positive outcome may be attributed to the following factors: ① The event was promptly detected and high-quality CPR was performed. During chest compressions, pulsation of the femoral artery could be felt on palpation. ② The potassium level decreased rapidly in the early stage. ③Throughout the entire CPR process, the ECG did not show asystole; instead, it most often displayed VF. This result was similar to that of the study by Kose et al, 4 which reviewed 10 case reports in the literature and showed that 30% of CA caused by hyperkalemia presented as VF, but all of these patients survived to hospital discharge.
Conclusion
ECG changes in a patient at risk for hyperkalemia demand immediate recognition by the doctors. The management of hyperkalemia-associated CA requires emphasis on ‘early recognition, comprehensive intervention, and dynamic monitoring’. Through POCT potassium monitoring, identification of high-risk ECG signals, combined with effective pharmacological intervention and high-quality CPR, the success rate of rescue treatment can be significantly improved, and patient prognosis can be enhanced.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report.
Author Contributions
Jiaozhen Chen: Conceptualization, Supervision, Writing - Original Draft, Writing - Review & Editing. Jizhen Chen: Conceptualization, Writing - Original Draft, Patient Management. Xinran Dang: Conceptualization, Writing - Original Draft, Literature Review. Jiali Chen: Investigation, Data Curation, Supervision, Literature Review. Yusuo Chen: Investigation, Data Curation, Literature Review. Yuanli Lei: Conceptualization, Funding Acquisition, Patient Management, Project Administration, Writing - Original Draft, Writing-Review & Editing. All the authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Wenzhou Basic Research Project (Y20220478 and GK20250110). The funding bodies did not have any role in the design of the study, data collection, and analysis, nor on the interpretation and dissemination of the result.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.