
Abstract
Intestinal tuberculosis (TB) typically presents with gastrointestinal symptoms, and cardiac conduction abnormalities associated with isolated intestinal TB have rarely been reported. We describe a 37-year-old male presenting with abdominal pain, constipation, and significant weight loss, with epidemiological exposure to cattle and raw milk. During hospitalization, he developed sinus bradycardia with a lowest corrected heart rate of approximately 46 beats per minute. The bradycardia persisted despite treatment with propantheline and atropine. Colonoscopy revealed terminal ileitis, and histopathology demonstrated nonspecific chronic ileitis without granuloma formation. Cardiac evaluation including echocardiography, troponin levels, electrolytes, and serum cortisol was unremarkable. Hydrocortisone administration was temporally associated with improvement in heart rate within 48 hours. Empirical anti-tuberculosis therapy was subsequently initiated, and the patient demonstrated sustained clinical improvement. Although causality cannot be definitively established, this case illustrates a rare temporal association between presumptive intestinal tuberculosis and steroid-responsive bradycardia. The report highlights the importance of considering systemic inflammatory processes in unexplained bradycardia, particularly in tuberculosis-endemic settings.
Keywords
Introduction
Tuberculosis (TB) remains a major public health challenge in Bangladesh, with a wide spectrum of extrapulmonary manifestations. Although TB primarily affects the lungs, hematogenous or lymphatic dissemination may lead to involvement of virtually any organ system. Cardiovascular involvement is relatively uncommon, occurring in approximately 1% to 2% of TB cases, but it is associated with increased morbidity and mortality. 1 The most commonly reported cardiac manifestations of tuberculosis include pericarditis and myocarditis; however, other rare presentations such as arrhythmias, aortitis, and cardiac tuberculomas have also been described in both pulmonary and disseminated forms of the disease. 2
Intestinal tuberculosis accounts for approximately 5% to 10% of extrapulmonary TB cases in Bangladesh. 3 The disease commonly affects the ileocecal region and presents with nonspecific symptoms such as abdominal pain, weight loss, fever, anorexia, and altered bowel habits. Because of overlapping clinical and endoscopic findings with inflammatory bowel disease, particularly Crohn disease, diagnosis of intestinal tuberculosis remains challenging. Microbiological confirmation is often difficult, and diagnosis frequently relies on a combination of clinical, epidemiological, endoscopic, and histopathological findings. 4
Systemic inflammatory conditions have been reported to affect cardiac conduction and autonomic regulation. Recent studies suggest that inflammatory cytokines may influence sinoatrial node function and result in transient bradycardia.5,6 However, isolated intestinal tuberculosis presenting with bradycardia has not been previously documented. Here, we describe a patient with presumptive isolated intestinal tuberculosis who developed steroid-responsive bradycardia, highlighting a possible but unproven association between systemic inflammation and reversible sinoatrial node suppression.
Case Study
A 37-year-old male, normotensive and nondiabetic, with a history of chronic smoking, presented to the outpatient department with severe generalized abdominal pain for 3 days. He also reported constipation for 20 days, significant weight loss of approximately 10 kg, and anorexia over the preceding 3 months. There was no history of previous tuberculosis or contact with a smear-positive TB patient. However, he reported frequent handling of cattle and consumption of raw cow’s milk.
On clinical examination, the patient appeared mildly exhausted with evidence of subcutaneous fat loss. His sitting blood pressure was 110/80 mmHg, which dropped to 100/70 mmHg on standing. Heart rate was 60 beats per minute. There was no lymphadenopathy, and respiratory and abdominal examinations were unremarkable. The patient was admitted for pain management and further evaluation.
A few hours after admission, the patient complained of severe weakness. Repeat examination revealed sinus bradycardia (pulse 52 bpm) with further fall in blood pressure. Electrocardiography (ECG) demonstrated sinus bradycardia without conduction abnormalities (Figure 1). Initial management included intravenous fluids and oral propantheline (15 mg 8 hourly). However, the bradycardia persisted. Intravenous atropine 0.5 mg bolus was administered, followed by repeated dosing as per standard bradycardia protocol. Despite these interventions, the heart rate remained low.
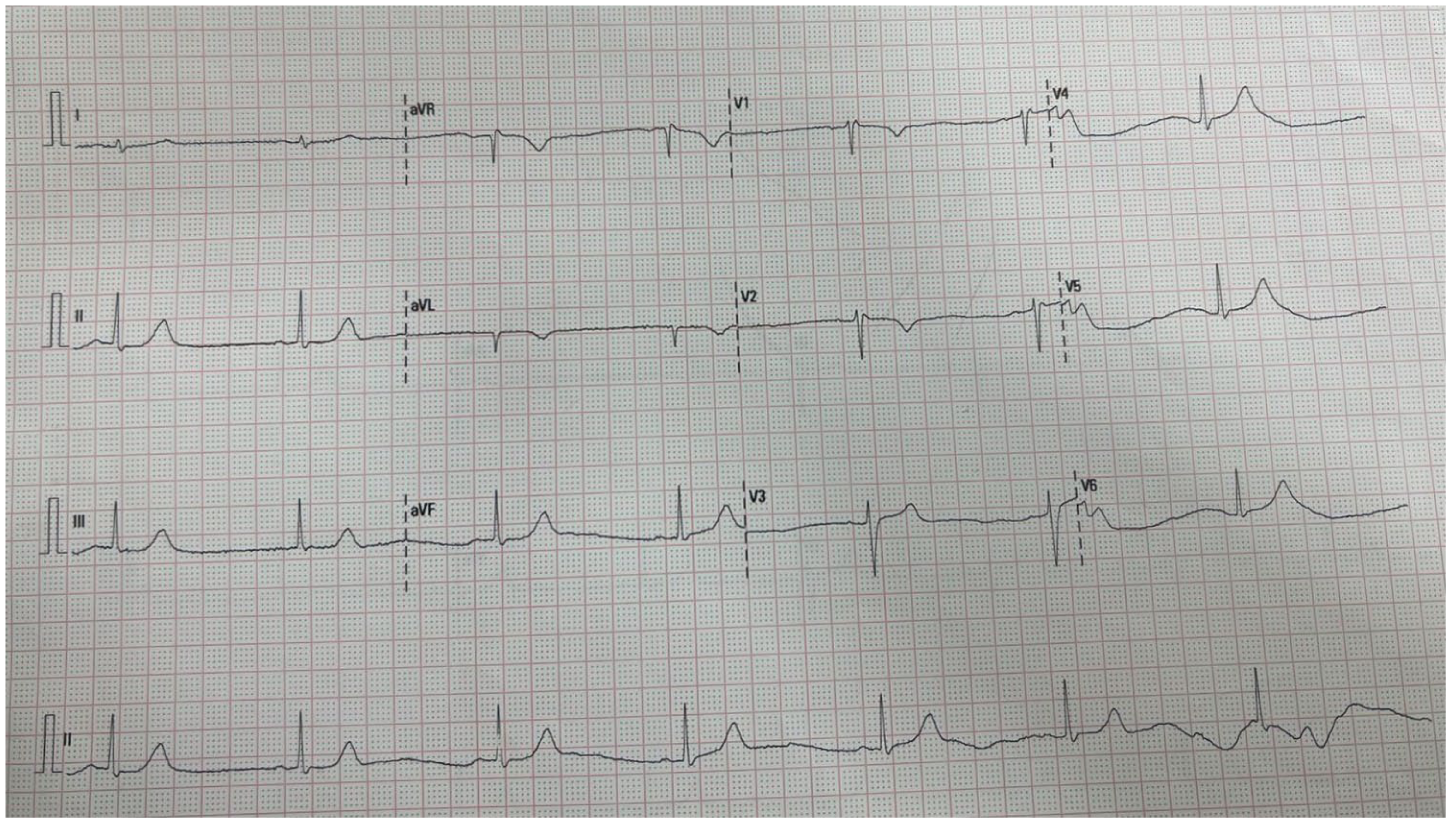
Sinus bradycardia (few hours after admission).
Initial laboratory investigations revealed hemoglobin of 12.9 g/dl, WBC count of 6,220/mm3, and platelet count of 208,000/mm3. ESR was 5 mm in the first hour. Random blood sugar, serum creatinine, serum electrolytes, and SGPT were within normal limits. Sputum GeneXpert for tuberculosis was negative. Chest X-ray and ultrasonography of the whole abdomen were unremarkable. Dilated bowel loops were seen on abdominal X-ray. Given the history of significant weight loss and persistent abdominal pain, colonoscopy with visualization of the terminal ileum was performed. The procedure revealed inflamed mucosa in the terminal ileum without ulceration, with differential diagnoses including intestinal tuberculosis and Crohn’s disease (Figure 2). Biopsy samples were obtained and conservative management was continued.
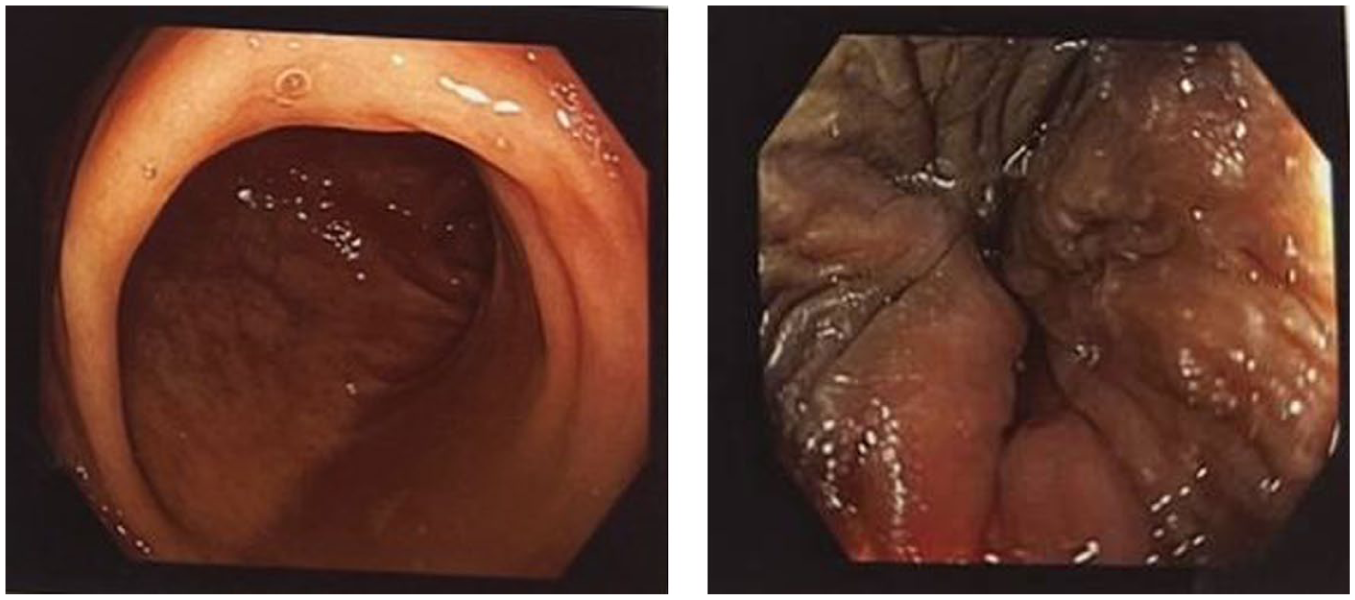
Mucosa of the terminal ileum is inflamed. Rest of the colon appears normal.
Subsequently, the patient developed worsening bradycardia accompanied by further hypotension. Atropine was administered 1.0 mg IV bolus and repeated every 30 minutes to a total dose of 3 mg to maintain heart rate; however, the bradycardia persisted, with the lowest recorded heart rate of 46 bpm (ECG was recorded at 50 mm/s; Figure 3). Serial ECGs continued to show sinus bradycardia without additional abnormalities. There was no associated chest pain or significant postural drop in blood pressure.
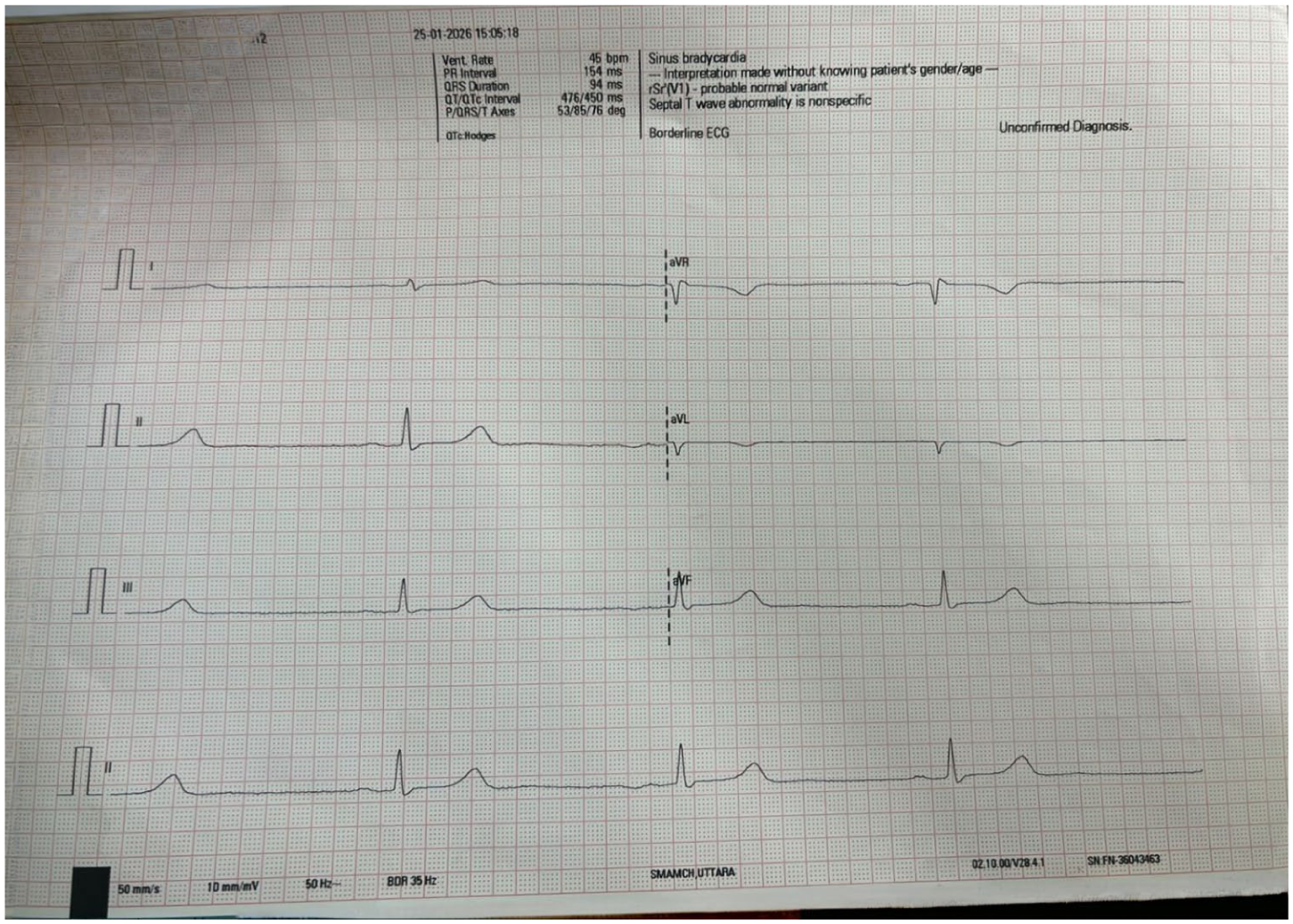
Sinus bradycardia persisted after atropine administration (1 day after admission).
Considering possible adrenal insufficiency, blood was sent for serum cortisol, and 200 mg intravenous hydrocortisone was administered empirically. Following this intervention, the patient’s heart rate increased significantly. The patient demonstrated marked clinical improvement over the following 48 hours, with normalization of heart rate to 70 to 80 bpm. Subsequently, Mantoux test returned negative, basal cortisol and troponin levels were within normal limits, and echocardiography showed no evidence of myocarditis. Histopathological examination revealed chronic ileitis without granuloma formation or caseous necrosis.
Timeline of events revealed that bradycardia developed within a few hours of admission, persisted despite propantheline and atropine administration, hydrocortisone was administered approximately 28 hours of admission, and heart rate improved gradually within 48 hours.
Given epidemiological risk factors, colonoscopic findings, histopathological evidence of chronic ileitis, and clinical response, presumptive intestinal tuberculosis was considered. Empirical anti-tuberculosis therapy was initiated along with tapering doses of prednisolone. The patient demonstrated sustained clinical improvement and was discharged. Prednisolone was tapered over 6 weeks. At follow-up, the patient remained symptom-free and continued anti-tuberculosis therapy for 6 months.
Discussion
This case describes a rare temporal association between presumptive intestinal tuberculosis and steroid-responsive bradycardia. However, the diagnosis of intestinal tuberculosis remains presumptive because microbiological confirmation was not obtained. The biopsy specimen was limited and submitted only for histopathological examination; therefore, GeneXpert or mycobacterial culture could not be performed. The patient declined repeat colonoscopy, further limiting diagnostic confirmation. Alternative diagnoses such as Crohn disease cannot be completely excluded.
Non-invasive microbiological testing such as stool GeneXpert or mycobacterial culture was not performed in this case but could be considered when biopsy samples are insufficient, particularly in resource-limited settings.
A case-based systematic review published in 2016 described a 53-year-old patient presenting with abdominal pain and weight loss, where colonoscopy revealed inflamed mucosa in the terminal ileum without frank ulceration. Although acid-fast bacilli staining was negative, autopsy later confirmed tuberculous ileotyphlitis. The authors suggested that terminal ileitis without ulceration may represent a hypertrophic form of intestinal tuberculosis that closely mimics Crohn’s disease, making diagnosis particularly challenging in endemic settings. 7
In the same review, Gurzu et al emphasized that tuberculosis-related terminal ileitis should be considered in endemic regions, especially in the presence of epidemiological risk factors such as consumption of raw milk or exposure to cattle. They further noted that nonspecific histopathological findings may support early hypertrophic intestinal tuberculosis, even in the absence of classical granulomas or caseous necrosis. 7
Similarly, a retrospective analysis by Zeng et al involving 42 confirmed cases of intestinal tuberculosis demonstrated that colonoscopic findings were variable. Ulcerative lesions were present in 95.2% of cases (ileocecal 59.5%, colonic 35.7%), whereas non-ulcerative inflammation occurred in 28.6% (terminal ileitis 16.7%, colitis 11.9%). Additional findings included ileocecal valve deformation (26.2%), pseudopolyps (21.4%), and strictures (14.3%). Histopathology revealed chronic granulomatous inflammation in 44.4% of cases and caseous necrosis in only 33.3%, while the remainder demonstrated nonspecific chronic inflammation, epithelioid cell hyperplasia (5.6%), or nondiagnostic tissue. Acid-fast bacilli were detected in only 53.1% of samples. 8 These findings highlight the diagnostic limitations of histopathology and microbiology in intestinal tuberculosis and support the role of clinical judgment and therapeutic response in establishing the diagnosis.
Following an extensive literature search, we found no published reports documenting cardiac involvement arising directly from isolated intestinal tuberculosis. A review by Mikalajūnaitė et al reported that cardiac tuberculosis manifestations—including pericarditis, myocarditis, and arrhythmias—typically occur via hematogenous dissemination from pulmonary tuberculosis, which accounts for less than 1%–2% of cases, or as part of disseminated disease, rather than from localized intestinal tuberculosis.9,10
The mechanism of bradycardia in this patient remains speculative. One possible explanation is cytokine-mediated suppression of sinoatrial node function. In 2018, Fan Ye et al proposed a hypothesis suggesting that inflammatory cytokines during systemic inflammation may directly affect sinoatrial node pacemaker cells, altering heart rate and autonomic responsiveness, and resulting in relative bradycardia. 10 Supporting this concept, Srinivasan et al described a case series in 2021 involving 6 COVID-19 patients who developed sinus bradycardia during peak systemic inflammation. These patients exhibited elevated inflammatory markers, including interleukin-6 and C-reactive protein, without evidence of myocardial injury, and bradycardia resolved as inflammation subsided. 5 However, inflammatory biomarkers such as C-reactive protein, ferritin, or interleukin-6 were not measured in this case, limiting assessment of systemic inflammatory activity. Therefore, cytokine-mediated suppression remains a hypothesis rather than a confirmed mechanism.
Furthermore, in 2023, Duong-Quy et al reported a case of severe bradycardia (heart rate 40 bpm) unresponsive to atropine in a COVID-19 patient with Guillain–Barré syndrome. Heart rate normalized following plasma exchange, suggesting reversible suppression of sinoatrial node function mediated by systemic inflammatory cytokines or subclinical myocarditis. 11 These findings are comparable to our patient, where possibly reduction of systemic inflammation led to rapid clinical improvement.
Alternative explanations must also be considered, including vagal-mediated bradycardia, occult myocarditis, primary sinus node dysfunction, medication effects, electrolyte abnormalities, and adrenal insufficiency. In this case, electrolytes, troponin, cortisol, and echocardiography were normal, making these causes less likely, although they cannot be completely excluded.
In the present case, the patient developed sinus bradycardia (lowest recorded heart rate: 46 bpm), which was refractory to propantheline and atropine. The improvement following steroid administration suggests a possible inflammatory mechanism, but causality cannot be established. In contrast, sick sinus syndrome typically demonstrates poor responsiveness to medical therapy and often requires permanent pacemaker insertion. 12 Additionally, anti-tuberculosis therapy and corticosteroids were initiated close together, further limiting causal inference.
Limitation
The biopsy specimen obtained during colonoscopy was small and submitted only for histopathological examination; therefore, GeneXpert or mycobacterial culture could not be performed. As the patient was unwilling to undergo repeat colonoscopy for additional sampling, microbiological confirmation of tuberculosis was not possible. Advanced rhythm evaluation such as Holter monitoring was not performed. Post-atropine serial ECG recordings were not systematically preserved, limiting objective assessment of pharmacological response. Additionally, as a single case report, the findings cannot be generalized and require further validation through larger studies.
Conclusion
To the best of our knowledge, this is the first reported case of steroid-responsive bradycardia temporally associated with presumptive isolated intestinal tuberculosis. Causality remains unproven. This case highlights the importance of considering systemic inflammatory processes in unexplained bradycardia, particularly in tuberculosis-endemic settings. Further studies are required to clarify underlying mechanisms.
Footnotes
Acknowledgements
We thank the patient’s family for consenting to the publication of this case report. We also acknowledge the healthcare team involved in the patient’s care.
Ethical Considerations
Written informed consent was obtained from the patient for publication of this case report, in compliance with institutional ethical guidelines. Ethical approval was not required for this case report in accordance with institutional policies.
Consent for Publication
Written informed consent was obtained from the patient to publish this report per the journal’s patient consent policy.
Authors Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The manuscript is based on a single patient case report; therefore, no datasets were generated or analyzed. Data sharing is not applicable.