
Abstract
Endoscopic ultrasound-guided transoesophageal biopsy (EUS-FNA/FNB) is a minimally invasive and highly accurate diagnostic technique for evaluating mediastinal lesions, particularly in centres where surgical approaches or endobronchial ultrasound are unavailable. We report the case of a 79-year-old woman with multiple comorbidities who presented with non-specific abdominal pain and a 5 kg weight loss over 1 month. Imaging revealed a 50% left pleural effusion and mediastinal and retroperitoneal lymphadenopathy. Endoscopic ultrasound demonstrated hilar, retroperitoneal and interaortocaval lymph nodes, prompting a transoesophageal fine-needle biopsy using a 22G needle and fanning technique, which was performed without complications. Initial histopathology suggested a lymphoproliferative process, and a subsequent excisional lymph node biopsy confirmed classical mixed-cellularity Hodgkin lymphoma associated with Epstein–Barr virus. This case highlights the diagnostic value of EUS-FNA/FNB in mediastinal lesions that are difficult to access using traditional techniques. Although its diagnostic yield is high, lymphomas—particularly Hodgkin lymphoma—may require additional tissue sampling to preserve architectural detail. Procedure success depends on sample adequacy, needle selection and operator expertise. Integrating EUS-guided biopsy into a multidisciplinary diagnostic pathway enables safe, effective and timely evaluation of mediastinal pathology, especially in resource-limited settings or in patients with significant comorbidities.
Keywords
Introduction
Mediastinal lesions comprise a heterogeneous group of tumours that may originate within the mediastinum or extend into it from adjacent structures. The most common histological entities include non-Hodgkin lymphoma (30.7%), thymoma (14%), Hodgkin lymphoma (12.9%), neurogenic tumours (10.9%), thyroid carcinoma (9.9%), germ cell tumours (4.95%), small round-cell tumours (3.96%), thymic hyperplasia (2.97%) and teratoma (1.98%). Less frequent lesions—each representing <1%—include lipoma, cutaneous tumours, fibrous tumours, spindle-cell neoplasms and giant-cell tumours. 1
Accurate tissue diagnosis is essential for appropriate staging and therapeutic planning. Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is considered the standard method for sampling mediastinal lesions. However, in centres where this technique is unavailable, alternative approaches such as mediastinoscopy or mediastinotomy may be required, although these procedures are costly, invasive and associated with prolonged hospital stay and postoperative complications including pneumonia and mediastinitis. 2
These limitations have led to increased use of less invasive sampling methods, including ultrasound-guided biopsy, computed tomography-guided percutaneous biopsy and endoscopic ultrasound-guided biopsy (EUS-FNA/FNB). 3 Although EUS-guided sampling is traditionally used for the diagnosis, staging and management of gastrointestinal lesions, it has also demonstrated safety and efficacy in evaluating benign and malignant mediastinal lesions. 4
EUS-FNA/FNB enables real-time puncture of target structures using negative-pressure aspiration to obtain adequate tissue for histopathological analysis. 5 It is generally considered a safe technique, with minimal complications such as transient pneumothorax, minor self-limited bleeding and mediastinal emphysema. 6
The diagnostic yield of EUS-guided sampling is comparable to that of surgical biopsy, even in the evaluation of lymphomas and other malignancies. 7 Furthermore, EUS allows access to a wide range of regions, including the anterior and posterior mediastinum, paratracheal space, subcarinal area and retroperitoneum. 8
Various needle calibres, such as 22G and 19G, in combination with techniques like fanning, have improved diagnostic performance by reducing the need for repeated procedures. 9 Additionally, the ability to obtain samples suitable for molecular and cytogenetic analysis enhances precision in therapeutic decision-making, 10 positioning EUS-guided biopsy as a valuable tool in modern oncological practice. 11
Case Presentation
A 79-year-old woman with a history of type 2 diabetes mellitus, hypertension, chronic obstructive pulmonary disease and chronic kidney disease presented with 1 month of non-specific abdominal pain and a 5 kg unintentional weight loss. She also reported reduced physical activity due to fatigue. Chest radiography revealed a 50% left pleural effusion, and thoracentesis demonstrated an exudative fluid.
Laboratory findings included leucocytes 11.8 × 103/µl, haemoglobin 7.9 g/dl, glucose 115 mg/dl, creatinine 3.2 mg/dl, carcinoembryonic antigen 3.0 ng/ml, CA-125 51.9 U/ml and CA 19-9 < 0.8 U/ml. Upper endoscopy showed no significant abnormalities. Due to persistent suspicion of an underlying malignancy, an endoscopic ultrasound (EUS) examination was performed.
EUS revealed abundant ascites and multiple enlarged hypoechoic lymph nodes in the hilar region (Figure 1A), retroperitoneum (Figure 1B) and interaortocaval space (Figure 1D), measuring up to 30 mm. The left lung appeared atrophic with an associated pleural effusion (Figure 1C).

Endoscopic ultrasound images showing: (A) hilar lymphadenopathy, (B) retroperitoneal lymphadenopathy, (C) atrophic left lung with pleural effusion, and (D) interaortocaval lymphadenopathy.
A fine-needle biopsy (FNB) of mediastinal and retroperitoneal nodes was performed using a 22 -gauge needle with 10 passes employing the fanning technique. The procedure was completed without complications.
Histopathology demonstrated fibrosis with eosinophilic infiltrate, raising suspicion for Hodgkin lymphoma, and a larger tissue sample was recommended. A subsequent excisional biopsy of a left sub clavicular lymph node revealed loss of normal nodal architecture (Figure 2A) with diffuse infiltration by medium-sized neoplastic lymphocytes and frequent mitoses (Figure 2B). Occasional Reed–Sternberg-like cells were identified (Figure 2C). Immunohistochemical staining for CD15 (Figure 2D), CD30 (Figure 2E) and LMP-1 (Figure 2F) confirmed a diagnosis of classic mixed-cellularity Hodgkin lymphoma associated with Epstein–Barr virus.
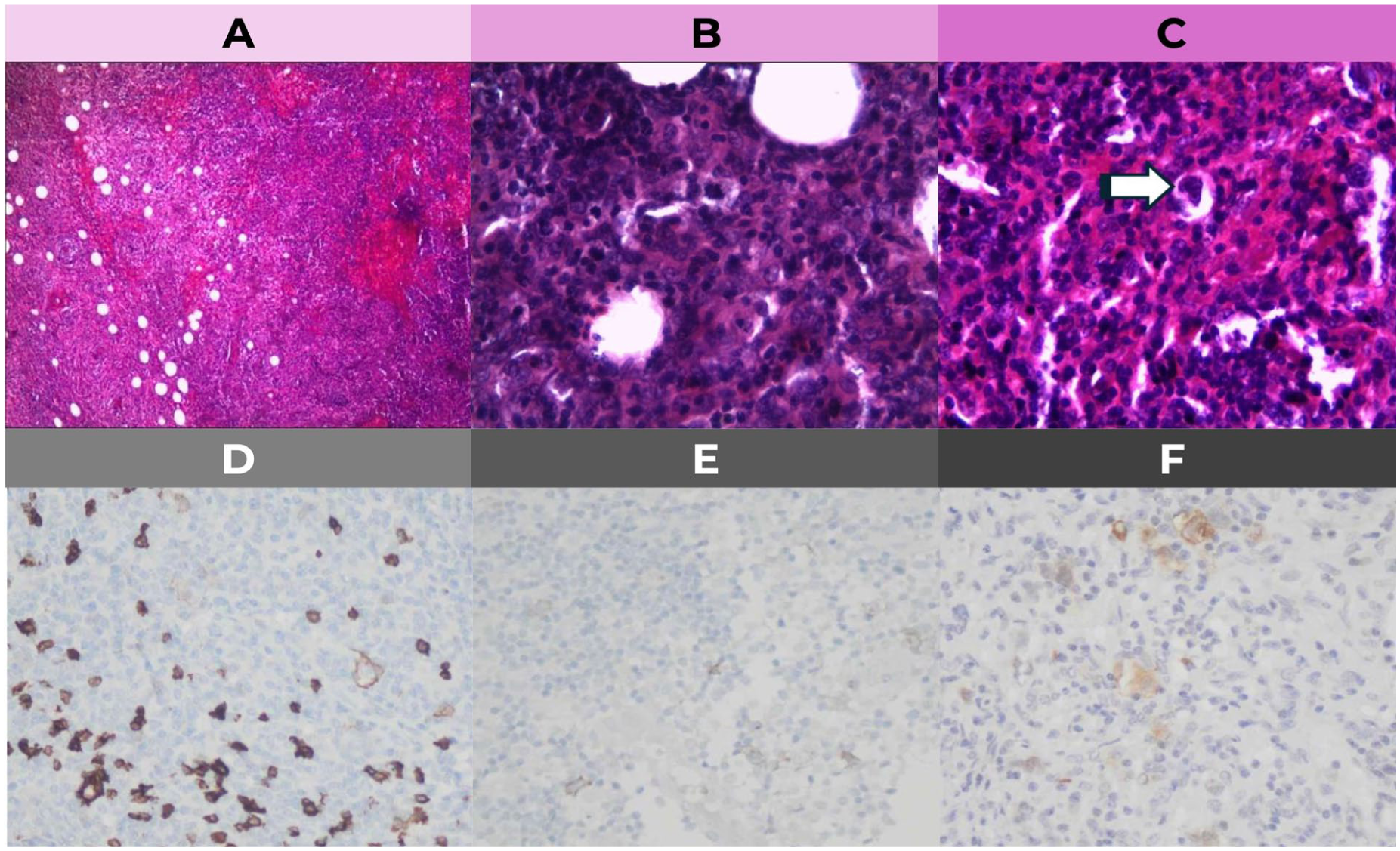
Histopathological and immunohistochemical findings of the excisional lymph node biopsy: (A) loss of normal nodal architecture, (B) diffuse infiltration by atypical lymphoid cells with increased mitotic activity, (C) occasional Reed–Sternberg-like cells, (D) CD15 positivity, (E) CD30 positivity, and (F) LMP-1 positivity consistent with Epstein–Barr virus-associated classic Hodgkin lymphoma.
Following histopathological confirmation of classical mixed-cellularity Hodgkin lymphoma associated with the Epstein–Barr virus, the patient was referred to the haematology service for further oncological management. Due to the patient’s advanced age and multiple comorbidities, including chronic kidney disease and chronic obstructive pulmonary disease, the available treatment options were carefully evaluated by a multidisciplinary team. After the diagnostic procedures, the patient remained clinically stable and was discharged with outpatient follow-up. At the time of reporting, she remains under specialist evaluation for the initiation of appropriate systemic therapy.
Discussion
Endoscopic ultrasound-guided fine-needle biopsy (EUS-FNA/FNB) has become an essential tool in the evaluation of mediastinal lymphadenopathy, particularly in settings where surgical access is limited or high-risk. Although traditionally used for the staging of gastrointestinal malignancies, its diagnostic utility has expanded significantly to include mediastinal, pulmonary and retroperitoneal lesions. 12
The technique offers several advantages over mediastinoscopy, including real-time imaging, minimal invasiveness, reduced procedure-related complications and the ability to access areas such as the aortopulmonary window, subcarinal space and interaortocaval region — regions that may be challenging to approach surgically. 13 In experienced centres, EUS-FNA/FNB provides diagnostic yields comparable to surgical biopsy, with sensitivity exceeding 85% for malignancy. 14
However, the diagnosis of lymphoma using EUS-guided sampling remains challenging. Hodgkin lymphoma in particular requires preservation of nodal architecture, which may not be adequately represented in fine-needle aspirates. 15 For this reason, many guidelines recommend obtaining core biopsy samples, using larger needle calibres (eg, 19 G), or supplementing cytology with immunohistochemistry, flow cytometry and molecular studies when feasible. 16 Despite these advances, an excisional biopsy often remains necessary to confirm the diagnosis, as demonstrated in the present case.
Several technical factors influence diagnostic accuracy, including operator experience, the number of needle passes, the use of suction, needle calibre and the fanning technique. 17 Additionally, immediate onsite cytopathological evaluation (ROSE) has been shown to significantly improve sample adequacy and reduce the need for repeat procedures, although it is not universally available. 18
Importantly, the safety profile of EUS-FNA/FNB is favourable. Reported complications are rare and generally mild, including self-limited bleeding, transient pneumothorax and mediastinal emphysema. 19 This makes the technique particularly valuable for elderly patients and those with significant comorbidities, such as the patient described in this report.
Overall, this case underscores the clinical relevance of EUS-guided biopsy in the diagnostic workup of mediastinal lesions, especially in resource-limited environments. While its limitations in the context of lymphoma must be acknowledged, EUS-FNA/FNB remains an indispensable component of modern thoracic oncology diagnostics.
Limitations
This report has several limitations inherent to single-patient case reports. Firstly, an additional excisional biopsy was required for the diagnosis of Hodgkin lymphoma because fine-needle sampling alone was insufficient to preserve nodal architecture for definitive subtyping. Secondly, long-term clinical follow-up was limited at the time of reporting, restricting assessment of treatment response and long-term outcomes. Despite these limitations, this case report demonstrates the significant diagnostic value of EUS-guided biopsy as an initial, minimally invasive approach for evaluating mediastinal lymphadenopathy
Conclusion
EUS-guided transoesophageal biopsy represents a safe, minimally invasive and effective diagnostic option for mediastinal lesions, particularly when access to surgical techniques or endobronchial ultrasound is limited. Although fine-needle sampling may not always provide sufficient tissue for definitive lymphoma subtyping, especially in classic Hodgkin lymphoma, it offers valuable initial diagnostic information and guides further clinical decision-making. Complementary excisional biopsy remains essential when architectural evaluation is required. This case highlights the importance of integrating EUS-guided sampling into a multidisciplinary diagnostic pathway to optimise timely and accurate diagnosis in complex mediastinal diseases.
Footnotes
Acknowledgements
The authors wish to thank the clinical staff involved in the patient’s care for their support and collaboration throughout the diagnostic process.
ORCID iDs
Ethical Considerations
Ethical approval was not required for this single-patient case report in accordance with institutional guidelines.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and all accompanying images.
Author Contributions
All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable as no datasets were generated or analysed for this case report.