
Abstract
Introduction:
Near-hanging is a common method of attempted suicide that can cause severe hypoxic brain injury, and survivors often require intensive care. We report a near-hanging case in a resource-limited setting with full neurological recovery despite an initially severe presentation.
Case Presentation:
A previously healthy 22-year-old man presented in mid-2025 unconscious after being rescued from a hanging incident. He had no known psychiatric history or prior suicide attempt. On arrival, he was comatose (Glasgow Coma Scale 6) with stable vital signs. Head CT was unremarkable for acute injury. Airway was secured by rapid sequence intubation without complication; cervical spine immobilization was applied, and imaging revealed no cervical or laryngeal trauma. A bedside ultrasound measurement of the optic nerve sheath diameter (ONSD) was performed (resource-limited setting, MRI unavailable).
Management and Outcome:
The patient received standard intensive care support, including mechanical ventilation, sedation, and monitoring of oxygenation and perfusion. His blood glucose and metabolic status were managed carefully. The initially elevated ONSD prompted continued neuroprotective care. Over 72 hours, he gradually regained consciousness and was extubated on day 4. He exhibited no focal deficits or cognitive impairment. By discharge on day 7, he had returned to baseline neurologic function and was oriented with normal examination.
Conclusion:
This case highlights that even severe near-hanging can have excellent neurologic recovery. It also underscores that a normal head CT in the acute period does not exclude significant hypoxic brain injury. In settings without advanced imaging, bedside ONSD ultrasonography may provide useful information about intracranial dynamics. Clinicians should be aware of these diagnostic and prognostic nuances and maintain aggressive supportive care in such cases.
Keywords
Introduction
Hanging is a leading method of suicide worldwide, and its prevalence has risen in recent decades. 1 Victims of hanging typically sustain global cerebral hypoxia due to asphyxia, rather than the spinal injuries associated with judicial hanging.2,3 In “near-hanging” cases, where patients survive the hanging event, acute airway obstruction and venous congestion lead to hypoxic–ischemic brain injury as the primary pathophysiologic insult. 3 By contrast, mechanical injuries such as cervical spine fracture, carotid artery dissection, or laryngeal/tracheal trauma are uncommon. In most series, major neck injuries are seen in only a small minority of patients (<5%).1,3 Patients typically present with impaired consciousness, hypoxia, and sometimes pulmonary edema or cardiac complications; retrograde amnesia of the event is also common.4,5
Prognosis after near-hanging is strongly related to the degree of hypoxic insult. In a multicenter cohort of 886 near-hanging patients admitted to intensive care units, roughly 56% survived to hospital discharge. 6 Importantly, among survivors in that series, 96% had good neurological function at discharge. 6 Other series have also found that the majority of patients surviving hanging recover fully. 4 Key predictors of poor outcome include initial cardiac arrest, prolonged suspension time, severe coma, metabolic derangements, and evidence of cerebral edema.5,6 For example, patients who present with out-of-hospital cardiac arrest have markedly higher mortality (often > 80%) and much lower rates of good recovery. 5 Likewise, admission Glasgow Coma Scale (GCS) score and laboratory values such as hyperglycemia and elevated lactate correlate with outcome.5,7
Clinical evaluation of near-hanging survivors includes a thorough neurological exam and imaging of the head and neck. 1 Cervical spine and vascular injury are typically assessed with CT (or CTA) of the neck, given the risk of occult trauma.1,3 Brain imaging with noncontrast CT is obtained routinely in comatose patients; however, early CT can be normal despite severe hypoxia.6,8 Indeed, radiologic signs of hypoxic encephalopathy (such as diffuse cerebral edema or loss of gray-white differentiation) may not appear immediately.8,9 Magnetic resonance imaging is more sensitive for detecting hypoxic injury (particularly diffusion-weighted MRI), 10 but is often unavailable in acute resource-limited settings. 2
Point-of-care ultrasound measurement of the optic nerve sheath diameter (ONSD) has emerged as a noninvasive surrogate marker of raised intracranial pressure (ICP) in various conditions.11,12 In adults, an ONSD > 5.0 to 5.5 mm correlates with ICP > 20 mmHg.11,13 Several meta-analyses have shown that ONSD sonography has high sensitivity and specificity for detecting intracranial hypertension in traumatic brain injury.12,14 In the context of global hypoxic-ischemic injury (such as post-cardiac arrest), elevated ONSD has been associated with poor neurological outcome in single-center studies.5,14 However, the utility of ONSD assessment in near-hanging survivors has not been well studied. In resource-limited environments where invasive ICP monitoring and MRI are not available, bedside ONSD ultrasound may offer a practical means to infer intracranial dynamics and guide prognosis.11,13
Case Presentation
A 22-year-old Ethiopian male (weight 60 kg) was brought to the Emergency Department (ED) of Tikur Anbessa Specialized Hospital after being found suspended by a garment at his workplace following an acute interpersonal conflict. Bystanders reported the patient had been suspended for approximately 15 minutes. He was discovered and rescued on scene; the interval from rescue to arrival at our emergency department was approximately 1 hour and 40 minutes (≈100 minutes). The estimated total downtime (suspension + prehospital delay) was therefore ≈115 minutes. On scene, his colleagues noted audible gurgling and agonal breathing; they lowered and cut the ligature prior to transport.
On arrival, he was unresponsive with a Glasgow Coma Scale (GCS) score of 6 (E1 V2 M3) and decerebrate posturing. Initial triage vital signs were: blood pressure 130/75 mmHg, pulse 122 beats/min (feeble), respiratory rate 24 breaths/min, oxygen saturation 89% on room air, and normal temperature. Capillary blood glucose was 110 mg/dL. A Triage Early Warning Score (TEWS) of 11 prompted immediate red-level resuscitation.
The airway was unprotected with copious oropharyngeal secretions. A cervical collar was applied. Rapid sequence intubation was performed on the first attempt using intravenous ketamine–propofol (Ketofol) and succinylcholine, and a 7.5 mm endotracheal tube was placed. He was started on volume-controlled mechanical ventilation with an initial FiO2 of 100% (tidal volume ~400 mL ≈ 6–7 mL/kg), respiratory rate 14 breaths/min, and PEEP 6 cm H2O; FiO2 was subsequently weaned to maintain SpO2 ⩾ 94%. Intravenous fluids were given for perfusion support.
Neurological examination after intubation demonstrated bilateral mid-dilated but reactive pupils and continued extensor posturing. Focused bedside ultrasound (FAST/EFAST) was negative for intra-abdominal or intrathoracic free fluid. Bedside ocular ultrasonography was performed using a high-frequency linear probe (≈10 MHz); optic nerve sheath diameter was measured 3 mm posterior to the globe with the eyelids closed, 3 measurements were obtained for each eye, and the mean value for each eye was recorded (right eye mean 10 mm, left eye mean 8 mm). Findings that are concerning for raised intracranial pressure. There was a definitive ligature mark on the anterior neck, but no facial or conjunctival petechiae, and no other external trauma.
Laboratory investigations showed hemoglobin 15.6 g/dL and platelets 187 × 103/µL. Serum potassium was 2.11 mmol/L and was corrected to 3.74 mmol/L with timely replacement. Serum creatinine was 0.2 mg/dL. Other routine biochemistry, including serum lactate and arterial blood gas on admission, were within clinically acceptable limits for the acute setting. Non-contrast brain and cervical spine computed tomography performed on presentation showed no acute intracranial hemorrhage, cerebral infarction, cervical spine fracture, or laryngeal/tracheal injury (Figure 1).
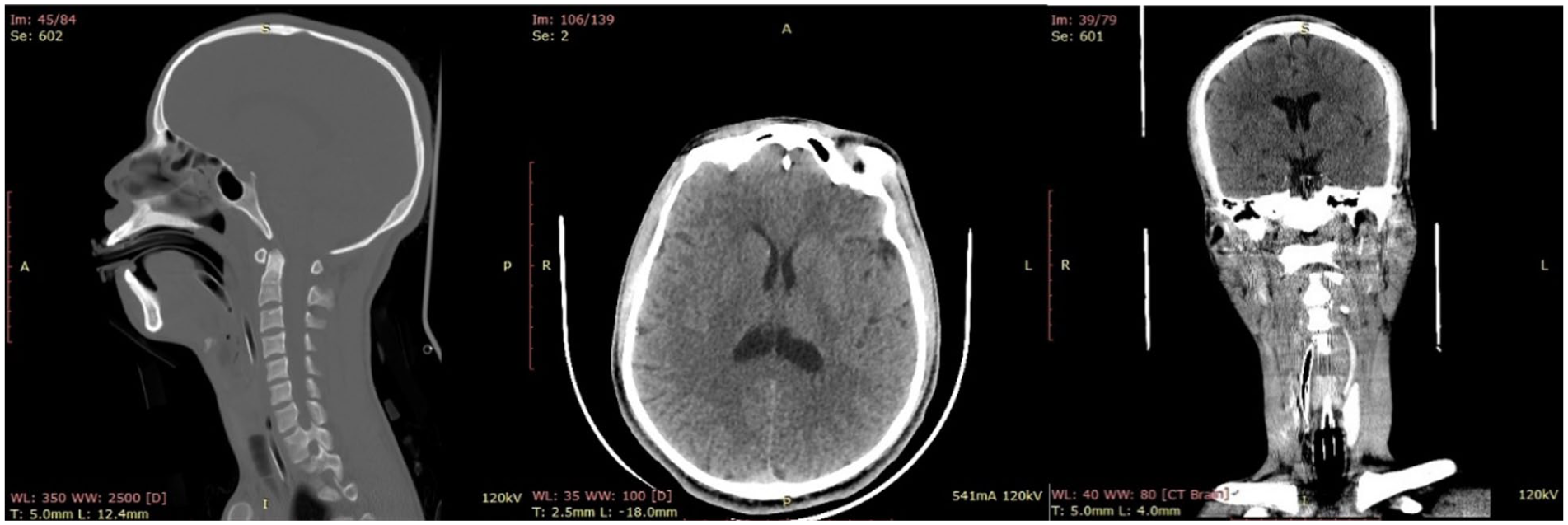
Non-contrast brain and cervical CT obtained approximately 4 hours after the hanging. Images include sagittal, axial, and coronal views of the brain and cervical spine/airway. No acute cerebral edema, intracranial hemorrhage, or focal infarction is evident. No cervical spine fracture or radiographic laryngotracheal injury is identified.
The patient was admitted to the intensive care unit (ICU) within 24 hours. He received neuroprotective and supportive care, including maintenance fluids, airway protection, and ventilatory support, dexamethasone 10 mg IV stat for suspected airway edema, and a single loading dose of mannitol 1 g/kg for presumed cerebral edema. Sedation was maintained with Ketofol. Prophylactic enoxaparin was started for venous thromboembolism prevention once deemed safe. Electrolyte abnormalities were corrected. He remained intubated for 4 days and was successfully weaned and extubated on ICU day 4. He continued to improve clinically and was transferred to the ward after 6 days in the ICU.
Psychiatry was consulted during the inpatient stay; brief psychotherapy was initiated, and a follow-up outpatient psychiatric plan was arranged. The patient made a gradual and complete neurological recovery and was discharged home after an additional 4 days on the ward (total hospital stay 10 days). At discharge, he was fully oriented, ambulatory, and had intact motor and sensory function. At outpatient follow-up, formal cognitive testing and a neuropsychological evaluation were performed and were within normal limits; no follow-up MRI or advanced neuroimaging was obtained.
Discussion
This patient’s course is remarkable for a delayed presentation and initially severe encephalopathy, yet eventual full recovery. In published series, most patients with prolonged hanging or associated cardiac arrest do poorly. For example, in 1 multicenter study of near-hanging patients with cardiac arrest, only 19% of those arrested had a favorable discharge outcome. 5 The median GCS of patients in poor outcome groups is typically <5,1,5 and refractory metabolic acidosis and edema on imaging portend a grave prognosis.6,7 By contrast, our patient ultimately regained consciousness with no deficits. Contributing factors likely included a relatively short suspension time (approximately 15 minutes) and prompt airway support and resuscitation, despite a prehospital delay of about 1 hour and 40 minutes before arrival at the emergency department. Quick return of spontaneous circulation after hanging is known to dramatically improve survival.6,7 Notably, initial serum lactate and glucose levels were not severely deranged in this patient (managed empirically), whereas published data have identified hyperglycemia (>1.4 g/L) and lactic acidosis as independent predictors of death in hanging victims.6,7 These observations highlight the importance of early critical-care management (oxygenation, ventilation, perfusion, and metabolic support) in influencing outcome.
The normal brain CT in our patient also merits discussion. Unlike many cases of anoxic injury, the initial noncontrast CT showed no obvious edema or infarction. Prior work has shown that CT findings of cerebral edema in hanging cases are strongly associated with poor outcomes.6,7 In 1 near-hanging cohort, 66% of patients with adverse outcomes had edema on CT versus 4% with a good outcome. 5 However, the absence of CT abnormalities does not guarantee a benign course, especially early on.6,9 Diffusion MRI can reveal diffuse ischemic injury that CT misses.8,10 In resource-limited settings like ours, MRI was not available, so we relied on clinical monitoring and ancillary tools. In this context, ONSD ultrasound was of interest. 11 Our bedside ocular ultrasound measured an ONSD of 8 to 10 mm, clearly above commonly used adult thresholds (normal < 5.5 mm), 13 suggesting raised intracranial pressure. While ONSD is a useful, non-invasive surrogate for raised intracranial pressure, it is operator- and technique-dependent and can show inter-observer variability. Studies indicate that an ultrasound ONSD ⩾ 5.0 to 5.5 mm has high sensitivity for ICP > 20 mmHg.11,13 Although larger ONSD on admission has been associated with worse outcomes after hypoxic arrest, 14 markedly increased ONSD does not always predict poor long-term recovery, transient ICP elevation, rapid reversal of edema following prompt airway support and resuscitation, or measurement limitations may partly explain this patient’s unexpectedly complete neurological recovery. We interpreted the increased ONSD as evidence of significant cerebral edema, which reinforced aggressive neuroprotective care (head elevation, mild sedation). 12 In future cases, serial ONSD measurements could potentially track the resolution of intracranial hypertension, although this application requires further validation.
Airway management and cervical evaluation were other important aspects. We intubated the patient promptly with manual in-line stabilization. Previous publications indicate that cervical spine injuries occur in a minority of near-hanging victims. For instance, Schellenberg et al found only 5 injuries (6%) in 71 patients, and none required surgical fixation. 3 Similarly, Dorfman note that cervical and laryngotracheal injuries each occur in <5% of cases. 1 Consistent with this, our patient’s neck CT angiogram showed no fractures, dissections, or airway trauma. Laryngeal injury is also rare; in the same cohort, Dorfman et al found that only 1% to 2% of cases had subglottic or esophageal injury. 1 Thus, while caution is warranted, our experience aligns with the literature that intubation is usually straightforward after hanging (provided laryngoscopy is done gently). We used a gentle technique with a bougie and minimized neck extension, in line with best practice for presumed cervical injury.1,3
The role of targeted temperature management (TTM) in hanging-induced cardiac arrest remains uncertain: small series and single-center reviews showed mixed results and selection bias, and larger observational studies have not demonstrated a clear benefit of routine TTM in hanging patients.1,15,16 Although TTM was considered in our patient, it was not initiated. The patient had no documented cardiac arrest requiring prolonged resuscitation, and available evidence for routine TTM after hanging is inconsistent; additionally, resource and logistical constraints (shivering control, infection risk, and intensive monitoring needs) made TTM impractical in our setting. In keeping with current practice for near-hanging care, our management prioritized basic neurocritical measures, early airway protection, optimization of oxygenation and perfusion, avoidance of hyperthermia, prompt correction of metabolic derangements (including glucose and electrolytes), and close neurologic monitoring, which are measures associated with improved outcomes in recent cohorts.1,3,6 Sedation and controlled ventilation were used to manage ICP surrogates and agitation, and early rehabilitation was started once the patient was stable, consistent with critical-care best practice.1,6
This patient’s recovery aligns with published series showing that many near-hanging patients who do not sustain prolonged cardiac arrest achieve good neurologic outcomes: a large ICU cohort reported 56% survival to discharge with 96% of survivors having favorable neurologic function, 6 while smaller series report similarly high rates of intact discharge function. 4 Cardiac arrest is the dominant adverse prognostic factor (OR ≈ 19.5 for mortality), and early return of spontaneous circulation and less severe metabolic disturbance predict survival and better neurologic recovery.5,7 Because MRI and invasive neuromonitoring were not available, bedside optic nerve sheath diameter (ONSD) sonography served as a practical ICP surrogate; ONSD correlates with intracranial hypertension and has prognostic value after hypoxic injury in several studies.11,12,14 Finally, as a single case report, our findings are hypothesis-generating but limited in generalizability and require confirmation in larger series. 17 Additionally, as MRI and formal neuropsychological assessment were not available, subtle cognitive or executive deficits cannot be fully excluded despite a normal bedside neurological examination at discharge.
Although markedly elevated optic nerve sheath diameters on admission, values typically associated with raised ICP, this patient made a complete neurological recovery. The case, therefore, highlights that good outcomes are possible with prompt basic resuscitation and targeted neuroprotection in low-resource settings, and the practical value (and limitations) of bedside ONSD ultrasound as a rapid adjunct when MRI or invasive ICP monitoring are not available.
Conclusion
Near-hanging survivors deserve aggressive care and careful assessment because even severe presentations can improve markedly. This case highlights key learning points. First, a completely normal early CT brain does not guarantee an excellent outcome; significant hypoxic injury may be occult. Clinicians should therefore not be falsely reassured by a normal head CT in a comatose patient. Additionally, noninvasive ONSD ultrasound may be valuable in resource-limited settings for hinting at elevated intracranial pressure and gaging severity, guiding supportive therapy. Furthermore, airway and spinal injuries are uncommon after near-hanging; routine intubation with spinal precautions is appropriate. Finally, maintaining normoxia and normoglycemia and preventing secondary insults seems critical. In summary, even in low-resource environments, careful monitoring and basic neurocritical care, informed by available tools like ONSD, can yield excellent outcomes in near-hanging patients.
Footnotes
Acknowledgements
We thank the patients and their families for agreeing to give their consent to publish their clinical records for this series.
Ethical Considerations
IRB review and approval were waived for this case report.
Consent for Publication
Written informed consent for the publication of the clinical details and accompanying images was obtained.
Author Contributions
Ayenew A. Wolie: Writing – Original Draft, Conceptualization, and Visualization. Chernet T. Mengistie: Writing – review & editing, Conceptualization, and Data curation. Biruk T. Mengistie: Writing – review & editing, Data curation, and Visualization. Gedefaw T. Minwagaw: Writing – Original Draft and Resources. Demmelash G. Nigatu: Supervision and Investigation. Nardos K. Melaku: Investigation and Data Curation. Awetahegn E. Kenno: Supervision and Resources. Akililu Azazh: Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying the results presented in this work are available within the manuscript.