
Abstract
Testicular tuberculosis (TB) is a rare form of extrapulmonary TB that can closely mimic testicular malignancy, making diagnosis challenging in immunocompetent patients without systemic symptoms. We report the case of a 50-year-old immunocompetent man who presented with a gradually enlarging, painless right testicular mass of several weeks’ duration, without constitutional symptoms such as fever, night sweats, or weight loss. Ultrasonography revealed a well-defined, heterogeneous hypoechoic and relatively hypervascular solid-cystic lesion, while serum tumor markers were within normal limits. Given the high clinical suspicion for malignancy, radical inguinal orchiectomy was performed without complications. Histopathological examination demonstrated necrotizing granulomatous inflammation with Langhans-type giant cells, and Ziehl–Neelsen staining was positive for acid-fast bacilli. Comprehensive systemic evaluation revealed no evidence of pulmonary or extrapulmonary TB, although both PPD and IGRA tests were positive. The patient was treated with standard anti-tubercular therapy and remained asymptomatic at 9-month follow-up. This case underscores the importance of considering primary isolated testicular TB in the differential diagnosis of atypical testicular masses, highlighting that early recognition and appropriate medical therapy may prevent unnecessary
Introduction
Testicular tuberculosis (TB) is one of the rarest manifestations of extrapulmonary TB worldwide, accounting for only about 2% to 4% of genitourinary TB cases. 1 Clinically and radiologically, it can closely resemble testicular tumors, which makes the diagnosis particularly challenging for clinicians. 2 The testes are typically shielded from tuberculosis by the blood testis barrier and when infection occurs it usually results from hematogenous spread or retrograde extension from the prostate, seminal vesicles, or epididymis. 3
Most patients present with a painless scrotal mass. In the absence of systemic symptoms such as fever, weight loss, or night sweats, this presentation may easily be mistaken for a testicular neoplasm. 4 As a result, radical orchiectomy is frequently performed under the assumption of malignancy. However in endemic areas, histopathologic evaluation may reveal granulomatous inflammation consistent with tuberculosis. 5 Isolated testicular TB without pulmonary disease or systemic symptoms is exceedingly rare, especially in immunocompetent individuals. 6
Testicular tuberculosis has been reported across a wide adult age range. Series and clinical studies show mean or median ages around the fourth to fifth decade, and genital TB is often described as more common in men aged approximately 30 to 50 years.7,8 Among infectious causes of testicular disease, tuberculous epididymo-orchitis is an uncommon entity, particularly in tuberculosis-endemic regions, and isolated testicular involvement represents a rare presentation within the spectrum of genitourinary tuberculosis.9,10
Although testicular tuberculosis is typically unilateral, bilateral, or contralateral involvement has been reported, and isolated testicular disease may occur in the absence of pulmonary or renal tuberculosis. 11 These findings underscore the need for a high index of clinical suspicion when evaluating atypical testicular masses, particularly in tuberculosis-endemic regions.
Case Presentation
A 50-year-old man presented with a gradually enlarging mass in the right testis that had developed over several weeks. The mass was painless and the patient reported no systemic symptoms such as fever, night sweats or weight loss. On physical examination the mass was firm and non-tender and the overlying scrotal skin appeared unremarkable while inguinal and pelvic lymph nodes were not palpable.
Scrotal ultrasonography showed that the left testis had normal size, echogenicity and position and both testicular arteries demonstrated normal caliber, flow, and peak systolic velocity. The right testis measured 46 × 22 mm with an epididymis of 11 mm, whereas the left testis measured 44 × 20 mm with an epididymis of 12 mm. Imaging revealed a solid-cystic heterogeneous mass in the lower pole of the right testis measuring 28 × 22 × 20 mm with a calculated volume of 6.6 cc and well-defined margins (Figure 1). Color Doppler evaluation indicated that the lesion was relatively hypervascular and hypoechoic, with no evidence of varicocele or hydrocele. These findings were consistent with a right testicular mass and further assessment of tumor markers was recommended.
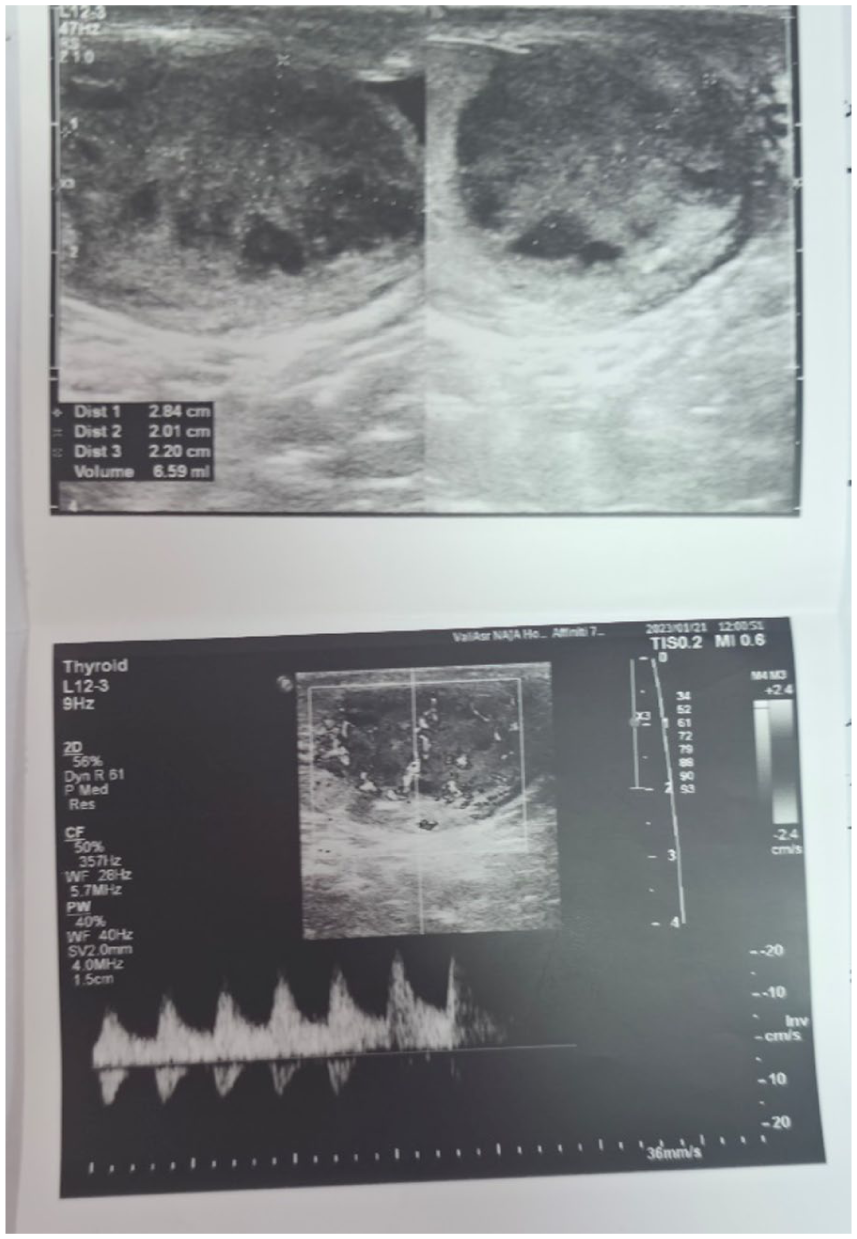
Scrotal ultrasound showing a heterogeneous solid-cystic mass in the lower pole of the right testis.
Tumor markers including alpha-fetoprotein (AFP), beta human chorionic gonadotropin (β-HCG), and lactate dehydrogenase (LDH) were within normal limits. The lesion was considered suspicious for testicular malignancy, as any solid intratesticular mass should be managed as malignant until proven otherwise, and serum tumor markers should be assessed prior to treatment. 12
As preoperative systemic evaluation for tuberculosis, such as chest radiography or CT, had not been performed, the clinical suspicion for testicular cancer was high. Preoperative non-invasive evaluations such as FNAC were not performed because institutional protocols consider any solid intratesticular mass suspicious until malignancy is definitively ruled out, and there was potential concern for tumor cell seeding if malignancy were present. Even when malignancy is suspected, the surgical approach for orchiectomy should be via an inguinal incision, and a scrotal incision is avoided to prevent potential lymphatic spread. Radical inguinal right orchiectomy was performed. The procedure was completed without complications.
Histopathologic examination of the excised testis revealed necrotizing granulomatous inflammation. The testicular parenchyma contained epithelioid histiocytes, lymphocytes and multinucleated giant cells (H&E 100×; Figure 2). On higher magnification (H&E 400×) there was a central area of necrosis surrounded by epithelioid histiocytes, multinucleated giant cells, lymphocytes, and Langhans type giant cells with peripheral horseshoe-shaped nuclei (Figure 3). Ziehl Neelsen staining demonstrated acid-fast bacilli within the necrotic foci and no malignant cells were identified. These histologic findings were consistent with testicular tuberculosis.

Testicular parenchyma demonstrating necrotizing granulomatous inflammation (H&E, 100×). (A) The section predominantly demonstrates extensive caseous necrosis, consistent with tuberculous necrosis. Necrotic foci are mainly rimmed by lymphocytes and epithelioid histiocytes. Three areas of more conspicuous necrosis are indicated by arrows. (B) The section illustrates granulomatous inflammation composed of epithelioid histiocytes, lymphocytes, and multinucleated giant cells. An area with more prominent granuloma formation is highlighted by an arrow.
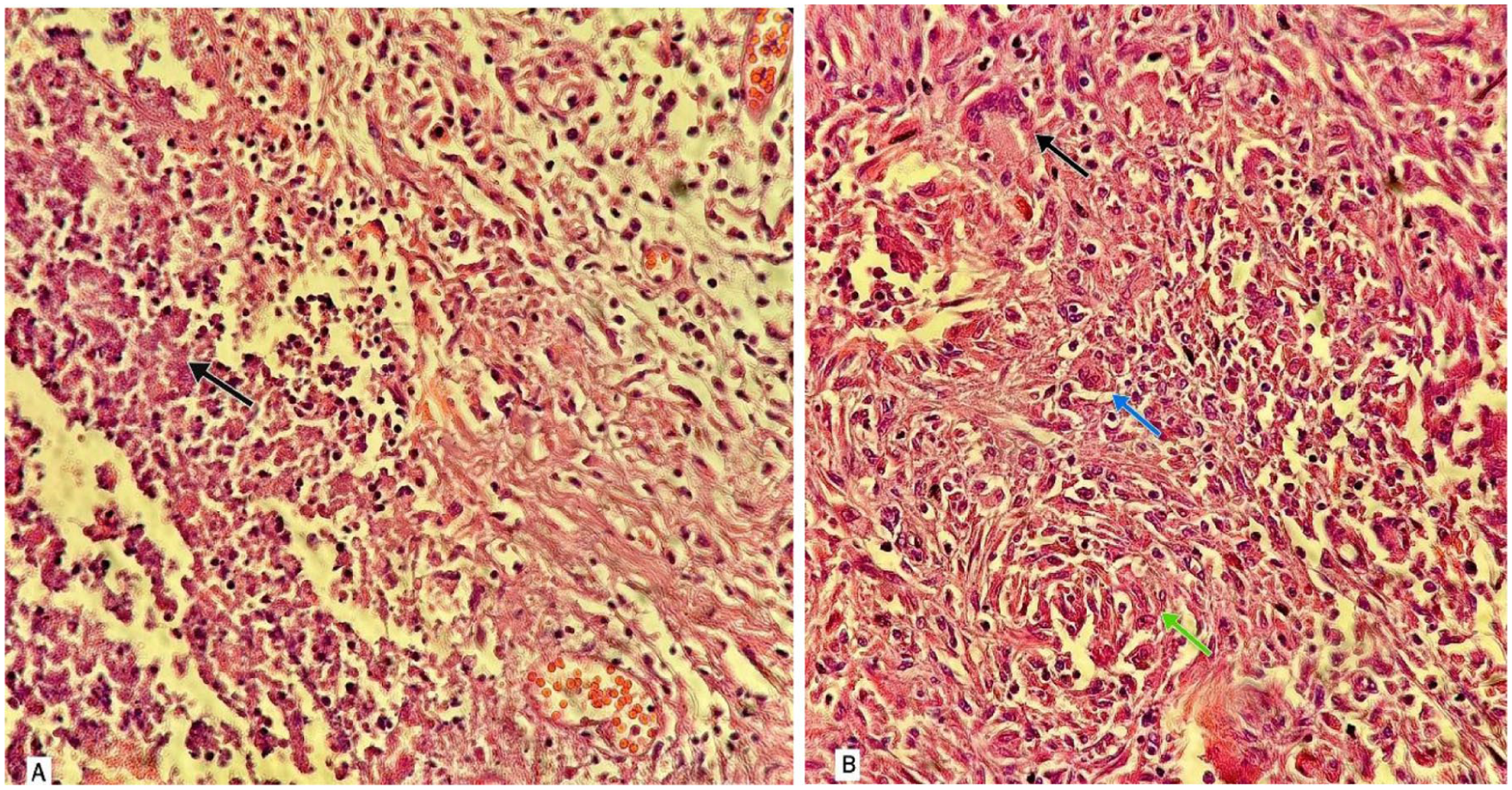
H&E-stained sections at 400× magnification demonstrating necrotizing granulomatous inflammation. (A) The section shows focal necrotic areas accompanied by chronic inflammatory cell infiltration, including lymphocytes and epithelioid histiocytes. One area with more pronounced necrosis is indicated by an arrow. (B) The section shows granulomatous inflammation composed of epithelioid histiocytes, lymphocytes, multinucleated giant cells, and a Langhans-type giant cell with nuclei arranged in a peripheral horseshoe pattern. A Langhans-type giant cell is indicated by a black arrow, a multinucleated giant cell by a blue arrow, and a focal aggregate of epithelioid histiocytes by a green arrow.
Following the unexpected diagnosis, the patient underwent a comprehensive systemic evaluation. The tuberculin skin test (PPD, 5 units) showed a 20 mm induration, which was considered positive. The IGRA test was also positive, consistent with prior sensitization to Mycobacterium tuberculosis. However, clinical examination, patient history, and imaging revealed no evidence of current or past pulmonary or systemic involvement, and the disease manifestation was confined to the testis. This finding highlights the diagnostic nuance of primary isolated testicular tuberculosis.
Chest radiography and abdominal ultrasonography showed no signs of active pulmonary or extrapulmonary disease. The patient had no history of TB exposure or disease and was immunocompetent. The patient was managed under the supervision of an infectious disease specialist, and standard 4-drug anti-tuberculosis therapy was initiated. The follow-up period lasted 9 months, during which the patient received anti-tuberculosis medication for 6 months. At the end of follow-up, the patient remained asymptomatic and showed no evidence of disease recurrence.
Discussion
Although testicular tuberculosis accounts for only a small fraction of testicular masses, it remains endemic in regions including South and South-East Asia, sub-Saharan Africa, and parts of Eastern Europe. 13 Isolated involvement of the testis or epididymis, particularly in immunocompetent individuals, is uncommon. 7 Clinically, testicular TB may closely mimic testicular cancer, as patients often present with painless scrotal swelling, similar to the presentation in our case. Ultrasonography typically reveals a heterogeneous hypoechoic intratesticular lesion, a finding that frequently raises strong suspicion of malignancy. 14 In a retrospective series of 69 patients, over half underwent orchiectomy due to radiologic features mimicking neoplastic disease. 8 In areas where tuberculosis is prevalent, testicular TB should remain a consistent part of the differential diagnosis for solid scrotal masses, particularly in middle aged men. Despite this, the sonographic pattern often overlaps with that of primary testicular tumors, leading to potentially avoidable radical orchiectomies. Features such as heterogeneous echotexture, focal hypoechoic regions, and preserved vascularity may favor granulomatous disease, although distinguishing TB from malignancy before surgery remains difficult.
A definitive diagnosis relies on histopathologic evaluation demonstrating caseating granulomas with Langhans type giant cells and, in some cases, acid-fast bacilli on Ziehl Neelsen staining. 15 In many clinical settings, advanced molecular tests such as PCR for Mycobacterium tuberculosis may not be routinely available. 15 Non-invasive diagnostic methods, including fine-needle aspiration cytology (FNAC) and PCR for Mycobacterium tuberculosis, have been shown in prior studies to facilitate early diagnosis of genitourinary TB and reduce unnecessary orchiectomies.16,17
Recognizing TB as a possible cause of testicular masses can help reduce unnecessary surgical procedures. Fine-needle aspiration cytology (FNAC) has proven effective in diagnosing genitourinary TB, facilitating timely initiation of anti-tubercular therapy and, in selected cases, avoiding orchiectomy. 18 Nevertheless, when malignancy cannot be reliably excluded especially in asymptomatic individuals without systemic features or identifiable TB risk factors radical orchiectomy may still be justified for both diagnostic and therapeutic purposes.
Given the strong clinical and radiologic suspicion of testicular malignancy, a comprehensive preoperative evaluation for tuberculosis was not undertaken prior to orchiectomy. Intraoperative and gross specimen photographs were unavailable due to institutional constraints. Although Ziehl–Neelsen staining confirmed the presence of acid-fast bacilli, the corresponding stained slide could not be retrieved for imaging at the time of manuscript preparation. These limitations reflect the challenges inherent to the diagnosis and documentation of primary testicular TB, particularly when preoperative differentiation from malignancy is difficult.
Following histopathological confirmation, patients require comprehensive evaluation to exclude pulmonary or disseminated TB. The absence of active disease in this case supports the diagnosis of primary isolated testicular TB. Standard anti-tubercular therapy with isoniazid, rifampin, ethambutol, and pyrazinamide remains the cornerstone of treatment, with most patients achieving full recovery without recurrence. 19
In settings with moderate TB prevalence, routine population wide screening is not practiced. Tests such as PPD or IGRA are generally reserved for individuals with clinical suspicion, documented exposure, or occupational risk. These tests cannot distinguish latent TB from active disease and are also unable to detect organ specific forms such as testicular TB. Therefore, routine screening would not have identified this patient’s condition before symptoms appeared.This case underscores the importance of considering TB in the evaluation of atypical testicular masses. Enhanced clinical awareness and broader access to non-invasive diagnostic modalities may help reduce unnecessary orchiectomies and improve patient outcomes.
Conclusion
This case is distinguished from previous reports by the complete absence of pulmonary or systemic tuberculosis, radiologic findings closely mimicking malignancy despite normal tumor markers, and definitive histopathologic confirmation with positive Ziehl–Neelsen staining. Testicular tuberculosis (TB) often presents with clinical and radiologic features that closely mimic testicular malignancy and may frequently lead to aggressive surgical interventions such as orchiectomy. Despite this, isolated testicular TB is rare and commonly misdiagnosed. This diagnostic challenge is particularly evident in immunocompetent patients who have no systemic symptoms and no prior history of tuberculosis. Definitive diagnosis still relies on histopathologic examination, which is essential for accurate identification. Clinicians should therefore maintain a low threshold of suspicion in patients presenting with atypical testicular masses, especially in regions where TB is prevalent.
Timely and accurate diagnosis enables clinicians to avoid unnecessary surgery while initiating prompt anti-tubercular therapy. Evidence indicates that, in most cases, appropriate treatment results in full recovery without recurrence. This case emphasizes the importance of considering tuberculosis in the differential diagnosis of testicular lesions, even in the absence of systemic manifestations.
Footnotes
Consent for Publication
Written informed consent for publication was obtained from the patients.
Author Contributions
Saeid Sadeghzadeh: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. Mohammad Eslami: Supervision, Writing – review & editing. Zohreh Panahi: Conceptualization, Validation. Shabnam Danaei Mehrabad: Investigation, Writing – original draft, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.