
Abstract
Background:
Congential thrombotic thrombocytopenic purpura (cTTP) is a ultrarare genetic disorder caused by reduced or absent ADAMTS13 enzyme activity. In contrast to the acquired form of TTP, which results from inhibitory autoantibodies against ADAMTS13, cTTP arises due to mutations in the ADAMTS13 gene and lacks such inhibitors. cTTP commonly manifests during infancy through recurrent episodes of hemolytic anemia and signs of microvascular damage. Episodes are often precipitated by infections or physical stressors.
Case presentation:
A 23-year-old female patient presented to the emergency department with microangiopathic hemolytic anemia (MAHA), a reduced platelet count and acute kidney injury stage 3 (AKI 3). Three days before she had suffered a knee injury, which was treated with fentanyl. The peripheral-blood smear showed many schistocytes. A thrombotic microangiopathy was suspected and therapeutic plasma exchange (TPE) was initiated. ADAMTS13 activity on admission was 4% without a detectable inhibitory antibody and an inherited ADAMTS13 deficiency was suspected. Genetic testing revealed 2 presumably compound heterozygous variants in the ADAMTS13 gene, confirming the diagnosis of cTTP. After 3 TPE platelet count raised significantly with improvement of renal function. Thereafter the patient received prophylactic plasma infusions every 2 to 3 weeks. At 1-year follow-up she had a normal renal function and no recurrence of hemolytic anemia.
Conclusion:
The present case of cTTP is notable for its late onset at first presentation, with unusual severe renal impairment. Rapid diagnosis and timely initiation of treatment are critical. Differential diagnoses such as malignant hypertension, sepsis, and autoimmune diseases like systemic lupus erythematosus must be excluded.
Keywords
Introduction
Thrombotic microangiopathies (TMAs) represent a diverse group of clinical disorders characterized by widespread microvascular thrombosis, particularly in small arterioles and capillaries. This process typically results in thrombocytopenia, microangiopathic hemolytic anemia (MAHA), and can lead to significant organ damage. 1 Thrombotic thrombocytopenic purpura (TTP) and hemolytic uremic syndrome (HUS) are considered classical examples of TMAs. 2 However, TMAs may also emerge secondary to various systemic conditions, such as severe hypertension, infectious diseases, malignancies, medications, and pregnancy-related disorders like HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelet count).
The estimated annual incidence of TTP is between 3 and 11 cases per million individuals. 3 The congenital form, known as cTTP (formerly hereditary TTP or Upshaw-Schulman syndrome), is extremely rare, though likely underdiagnosed, with a reported prevalence of approximately 1 in a million.4,5 This autosomal recessive disorder arises from pathogenic variants—hereafter referred to as “mutations”—on both alleles of the ADAMTS13 gene located on chromosome 9. 6 These mutations are diverse in nature: about 60% are missense substitutions involving single amino acid changes, while the remaining ~40% consist of frameshift mutations, splice-site alterations, deletions, and insertions.7-9
Case Report
A 23-year-old female patient presented to our hospital’s emergency department with acute kidney injury accompanied by a significantly reduced platelet count.
Three days before this admission the patient suffered a knee injury, which was treated at another hospital with fentanyl. The patient was then released home. However, no blood samples were obtained at that time, so no laboratory results are available from this visit. The next day nausea and vomiting developed and she was subsequently re-evaluated in the emergency departmend of the other hospital.
Upon examination, the patient reported persistent nausea, vomiting, abdominal and back pain, intravenous isotonic crystalloid solution was administered. The platelet count was 26 × 109/l (normal range, 173-390 × 109/l) and creatinine 6.86 mg/dl. The patient was transferred to our hospital for further evaluation.
During initial assessment in the emergency department, the patient reported nausea and pain in the back. She reported no headache, changes in vision, chest pain, shortness of breath, hematuria, or diarrhea. She denied taking any medicines other than pantoprazole and metoclopramide for nausea. She did not have any contact with animals. She reported occasional alcohol consumption and denied any history of smoking or illicit drug use.
Vital signs included a temperature of 36.4°C, heart rate 71 beats per minute, blood pressure of 140/89 mmHg, and oxygen saturation of 98% on room air. The weight was 68 kg, and the mucous membranes were moist. There was no rash or purpura. No other abnormalities were noted on physial examination.
The creatinine level was 6.8 mg/dl, urea 114 mg/dl, lactate dehydrogenase (LDH) 522 U/l, and creatine kinase (CK) 182 U/l. The serum level of troponin I was normal. Examination of a peripheral-blood smear revealed anisocytosis and polychromasia of the red cells, with many schistocytes (1.3%). A pregnancy test was negative. Hepatitis A, B, and C were also negative. At initial presentation, urinalysis showed 80 erythrocytes per high-power field (Normal range: 0-1) with 15 leukocytes per high-power field (Normal range: 1-4), proteinuria was 1.6 g/g creatinine and albuminuria 1.2 g/g creatinine. On urine sediment examined by phase-contrast microscopy, she had erythrocyturia without acanthocytes, that is, no nephritic sediment. Table 1 summarizes the patients laboratory findings.
Laboratory Findings on Admission and During Early Clinical Course.

Renal ultrasonography revealed normal-sized kidneys and no evidence of hydronephrosis. A chest radiograph was normal.
The patient was transferred to the intesive care unit for further management. Under the suspected diagnosis of TTP (PLASMIC SCORE 6) we began treatment with intravenous methylprednisolone (100 mg) and TPE was initiated. Assessment included ADAMTS13 enzymatic activity with anti-ADAMTS13 antibodies and antinuclear antibodies (ANA). Caplacizumab was started on the same day.
After 3 days the platelet count raised to 147 × 109/l and TPE was stopped after 3 sessions in total. ADAMTS13 activity on admission was 4% (50%-100%), anti-ADAMTS13 antibodies were pending. Approximately 4 days after TPE was stopped (and 7 days after admission to this hospital), the ADAMTS13 activity was 29% and 4 days after that activity had decreased to 11% (Table 2). The platelets were normal. Rituximab was added with the initial assumption of acquired TTP and glucocorticoid therapy was rapidly tapered. During the next 2 weeks ADAMTS13 activity fell to less than 5%. The patient did not have a detectable inhibitory antibody and an inherited ADAMTS13 deficiency was presumed. Consequently, no further rituximab doses were administered and caplacizumab was discontinued. Results of genetic testing confirmed the diagnosis of inherited TTP (the Upshaw–Schulman syndrome) and regular fresh frozen plasma (FFP) infusions were administered.
ADAMTS13 Activity and Antibodies.

The patient received prophylactic FFP infusions every 2 to 3 weeks. At 1-year follow-up, the patient remained clinically stable. Renal function had normalized with complete remission of kidney involvement, there was no recurrence of TTP and laboratory parameters—including platelet count, hematocrit, and LDH—were within normal limits.
Discussion
TTP is clinically characterized by the occurrence of MAHA in combination with moderate to severe thrombocytopenia. This presentation may or may not be accompanied by symptoms of end-organ involvement, which can affect the neurological, cardiovascular, gastrointestinal, or renal systems. However, the development of oliguric or anuric renal failure necessitating dialysis is uncommon in typical TTP cases10,11
Blood samples intended to assess for thrombocytopenia, microangiopathic hemolysis, ADAMTS13 activity, and organ dysfunction should be collected prior to the initiation of FFP therapy. In cases of TTP, patients typically present with marked thrombocytopenia (commonly with platelet counts below 30 × 109/l), along with anemia, reduced hematocrit, and laboratory indicators of hemolysis such as elevated LDH, low haptoglobin, elevated indirect bilirubin, and the presence of schistocytes on a peripheral blood smear.12,13 Schistocytes result from the mechanical fragmentation of erythrocytes as they traverse fibrin strands or von Willebrand factor (VWF)-platelet aggregates. According to the International Council for Standardization in Hematology (ICSH), their presence should be quantified as a percentage based on the evaluation of at least 1000 red blood cells under microscopy. A schistocyte count exceeding 1% strongly suggests thrombotic microangiopathy (TMA) when no alternative diagnosis is apparent. 14 In certain conditions such as transplant-associated microangiopathy (TAM), a higher threshold—greater than 4% schistocytes—may be required due to background red cell fragmentation caused by treatments like total body irradiation or chemotherapy. 15 It is important to note that schistocytes may be absent in the early stages of the disease, and in some cases, they may persist despite clinical remission, such as normalization of LDH levels and platelet counts following TPE therapy. 16
It is essential to differentiate TTP from atypical hemolytic uremic syndrome (aHUS; see Figure 1) and other forms of TMA (refer to Table 3), which may arise from factors such as drug exposure, underlying malignancy, severe hypertension, HELLP syndrome, or disseminated intravascular coagulation (DIC). When the initial platelet count is ⩾30 × 109/l and serum creatinine is ⩾2.3 mg/dl, the likelihood of an autoimmune-mediated TTP due to severe ADAMTS13 deficiency is significantly reduced. 17 In such cases, alternative causes of TMA should be thoroughly investigated, as both management strategies and long-term prognoses can differ considerably.

Algorithm for differentiating thrombotic thrombocytopenic purpura (TTP) from atypical hemolytic uremic syndrome (aHUS) and their therapeutic modalities. Plasma ADAMTS13 activity <10% is the single most important test for differentiating TTP form aHUS after excluding other known causes of thrombotic microangiopathy (TMA), including disseminated intravascular coagulation (DIC), mechanic valves and malignant hypertension. Other clinical features, including the platelet count (<30 × 109/l), degree of renal injury (creatinine < 2.2 mg/dl) and swift response to plasma exchange therapy, are also crucial for the initial diagnosis before ADAMTS13 activity becomes available.6,10
Differentiating TTP from Other TMAs.
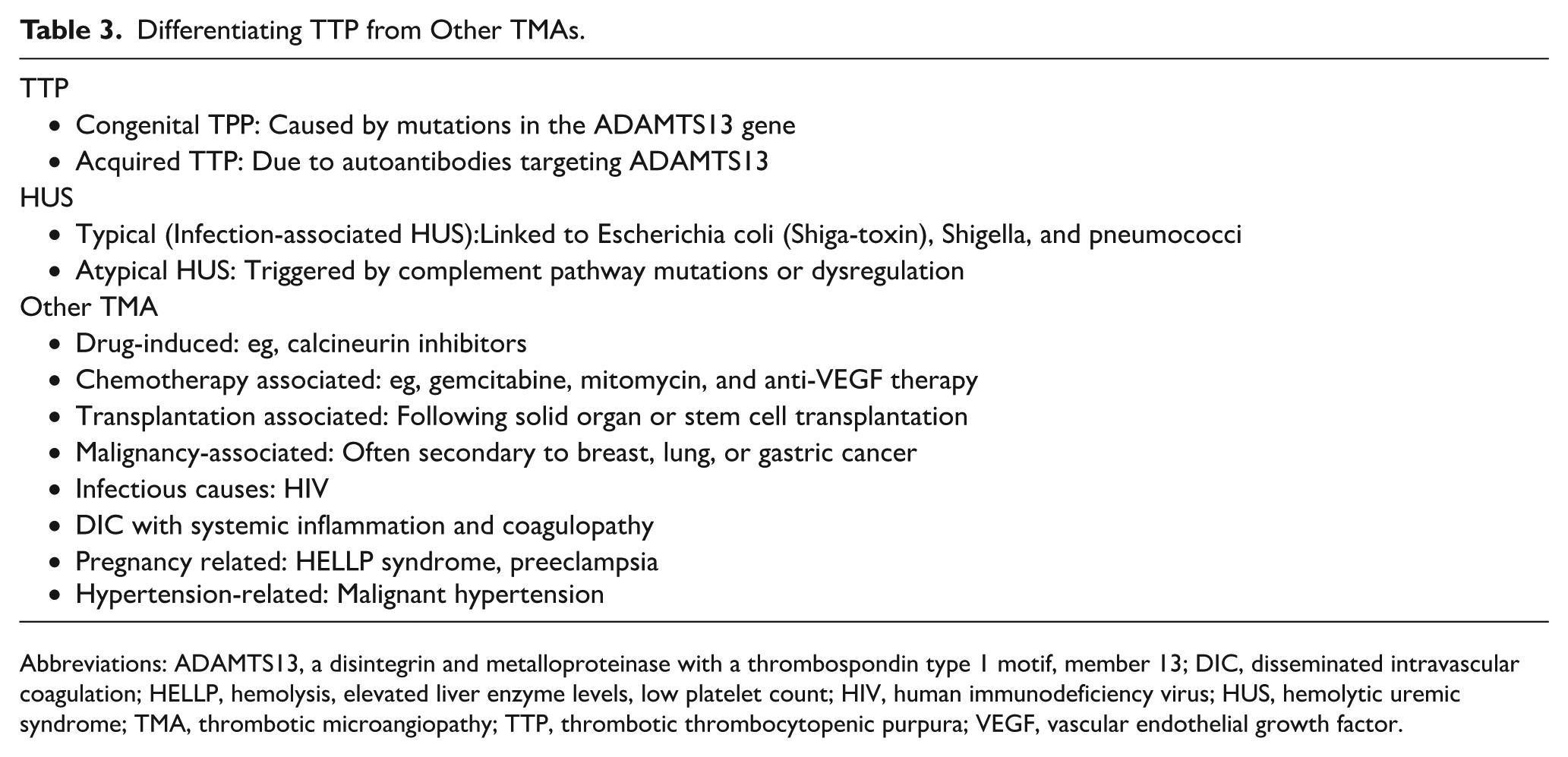
Abbreviations: ADAMTS13, a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13; DIC, disseminated intravascular coagulation; HELLP, hemolysis, elevated liver enzyme levels, low platelet count; HIV, human immunodeficiency virus; HUS, hemolytic uremic syndrome; TMA, thrombotic microangiopathy; TTP, thrombotic thrombocytopenic purpura; VEGF, vascular endothelial growth factor.
Plasma ADAMTS13 activity serves as a pivotal biomarker in the differential diagnosis of TMAs. In the appropriate clinical setting, an ADAMTS13 activity level below 10% is highly specific for TTP.18,19 Recent evidence shows that using this <10% threshold yields a sensitivity of 100% and specificity of 99% for diagnosing TTP, with a positive predictive value of 91% and a negative predictive value of 100%, after excluding confounding conditions such as infections and DIC. 20 To further classify the condition as congenital or acquired TTP, an inhibitor assay is automatically performed when ADAMTS13 activity is found to be markedly reduced. Similar to other coagulation inhibitor assays, 1 inhibitor unit is defined as the amount required to halve the enzyme activity in a 1:1 mixture with normal plasma21,22
In acute clinical scenarios where ADAMTS13 activity results are not immediately available, validated clinical scoring tools can aid in estimating the likelihood of severe ADAMTS13 deficiency. One such model (French Score) was proposed by Coppo et al, 17 who identified 3 clinical parameters at presentation: serum creatinine < 2.2 mg/dl, platelet count <30 × 109/l, and positive ANA. This model yields a positive predictive value (PPV) of approximately 99% and a specificity around 98% for detecting severe acquired ADAMTS13 deficiency. However, its sensitivity is limited to 46%, reducing its utility for broad screening. A more comprehensive model is the PLASMIC score, which incorporates 7 criteria: platelet count <30 × 109/l, evidence of Laboratory hemolysis (elevated indirect bilirubin, reticulocytosis, or decreased haptoglobin), absence of active malignancy, subjects without a history of solid organ or stem cell transplant, mean corpuscular volume (MCV) < 90 fL, INR < 1.5, creatinine < 2.0 mg/dl. 22 This scoring system has shown comparable predictive accuracy to Coppo’s model in identifying patients with severe ADAMTS13 deficiency, but it offers better performance in identifying low-risk patients, making it a valuable triage tool in emergency settings. 22 However, similar to the French Score, its utility is limited in congenital TTP. Patients with hereditary TTP often present with milder thrombocytopenia, normal renal function and episodic or chronic symptoms rather than the fulminant presentation typical of acquired TTP. As a result, both scores frequently underestimate the likelihood of congenital TTP, and diagnosis relies primarily on severely reduced ADAMTS13 activity in the absence of inhibitor supported by confirmatory genetic testing. 17
Hereditary TTP arises from genetic mutations that lead to markedly reduced ADAMTS13 activity, whereas the acquired (autoimmune) form—which is more frequently observed—is caused by autoantibodies that inhibit ADAMTS13 function. 23
Although cTTP is classified as a monogenic disorder, its clinical expression varies widely. In some individuals, symptoms emerge during the neonatal period, while others remain asymptomatic until adolescence or early adulthood. This phenotypic variability is primarily attributed to differences in the nature of the underlying mutations and the residual plasma ADAMTS13 activity.24,25 In neonates, cTTP often presents with jaundice and thrombocytopenia. 26 During early childhood, episodes may be precipitated by infections or routine vaccinations. For individuals who first develop symptoms in adulthood, pregnancy is frequently identified as the triggering factor. 27 Earlier literature described a bimodal age distribution of disease onset, with 1 peak occurring in early childhood (before age 5) and another in young adulthood, particularly during or following pregnancy.26,28,29 Interestingly, some patients in the latter group had received exchange transfusions shortly after birth, raising the possibility that their later-onset symptoms represent a reactivation rather than a true adult-onset presentation.30,31
Additionally, asymptomatic carriers have been identified through family screening, with some individuals remaining without symptoms well into their fifth to seventh decades of life.31,32 Whether these cases represent genuinely mild forms of the disease or are underrecognized due to early morbidity or mortality is still under investigation.
Although the initial onset of cTTP may occur at varying ages, the majority of affected individuals tend to follow a chronic relapsing disease course, often necessitating prophylactic therapy to avert long-term complications, particularly involving the nervous system, kidneys, and other vital organs.
We present a case of late onset of cTTP. The patient exhibited hallmark signs of TPP, including microangiopathic hemolytic anemia, a reduced platelet count, and renal injury. A pregnancy test was negative. The Coombs Test was also negative. An infection was not apparent. Kidney failure was considered to be due to volume depletion after vomiting. After administration of isotonic cystalloid solution, we saw a robust response in urine output and improvement in GFR leading us to the assumption of prerenal acute kidney injury. An autoimmune disorder, such as SLE was unlikely in the absence of antinuclear antibodies (ANA < 1:80).
Serum creatinine is often normal in patients with TTP, though temporary increases may be seen in about one-third of cases; true acute kidney injury is rare. 33 We attributed the TTP manifestation episode to the knee injury or the Fentanyl administration. Anamnestically, the patient reported no prior episodes compatible with TTP and no previous pregnancy. Several drugs, including immunosuppresive therapy, antineoplastic medications, cocaine, and analgesics have been reported to cause TMA. 34 The patient received 3 sessions of therapeutic plasma exchange, each involving the exchange of approximately 1 plasma volume. Following treatment, the platelet count rose to 147 × 109/l. Laboratory analysis revealed a markedly reduced ADAMTS13 activity in the absence of detectable inhibitors, supporting the diagnosis of cTTP (see Table 4).
Clinical scenarios that should prompt evaluation for congenital TTP and ADAMTS13 testing.

Genetic testing by targeted paired-end next-generation sequencing revealed 2 presumably compound heterozygous variants in the ADAMTS13 gene. First, on the maternal allele the heterozygous 1-basepair duplication c.4143dup p.(Glu1382Argfs*6) in the final exon of the gene that represents one of most common pathogenic variants for cTTP in the European population and has been described in multiple homozygous as well as compound heterozygous cTTP patients. Moreover, the heterozygous ADAMTS13 missense variant c.3801C>G p.(Asn1267Lys) which has neither been described in the literature nor in databases so far and is bioinformatically predicted to be damaging. This variant most likely resides in trans on the paternal allele, however, could not be proven as genetic testing of the healthy father was not feasible.
To date, regular prophylactic FFP infusions remain the cornerstone of treatment for hereditary TTP caused by mutations in the ADAMTS13 gene. According to the study by Furlan et al, 38 the half-life of exogenous plasma-derived ADAMTS13 is approximately 2 to 3 days. For preventive purposes, administration of 5 ml/kg of fresh frozen plasma every 2 weeks appears sufficient to reduce the risk of acute episodes. In contrast, when an acute episode occurs, a higher dose of 10 ml/kg every 1 to 2 weeks may be required to achieve clinical stabilization. 39 However, the burden of regular FFP infusions is substantial, and some patients may be unwilling or unable to adhere to such a regimen. Reflecting this, the 2020 ISTH guidelines propose either routine prophylaxis or a watch-and-wait strategy for patients with cTTP in remission. Notably, the strength of evidence supporting this recommendation is low, with limited data and low certainty. 40
In November 2023, the U.S. Food and Drug Administration (FDA) granted approval for ADAMTS13, recombinant-krhn—the first recombinant enzyme replacement therapy specifically designed for use in both adults and children with cTTP. This genetically engineered protein is authorized for both prophylactic and on-demand treatment. It is administered intravenously once every other week for prophylactic enzyme replacement therapy, and once daily for on-demand enzyme replacement therapy. The most common side effects include headache, diarrhea, migraine, abdominal pain, nausea, upper respiratory tract infection. 41
A phase 3 randomized controlled trial investigated the efficacy and safety profile of recombinant ADAMTS13 in comparison to standard FFP based therapy. 42 The study demonstrated that recombinant ADAMTS13 is a viable and effective option for prophylactic treatment in individuals with congenital TTP. Importantly, no significant safety issues were identified, and no neutralizing anti-ADAMTS13 antibodies were observed during the study period.
In the 2025 focused update of the ISTH guidelines for TTP, recombinant ADAMTS13 has replaced FFP as the preferred option for long-term prophylaxis in patients with congenital TTP in remission, based on moderate-certainty evidence. Where recombinant ADAMTS13 is not available or feasible, the use of prophylactic FFP rather than a watch-and-wait approach is preferred, while emphasizing individualized decision-making that considers treatment burden, comorbidities, and patient preference. 43
In our case, the patient exhibited severely decreased ADAMTS13 activity (<1%) in the absence of prior FFP therapy, which prompted initiation of a prophylactic FFP infusion regimen to minimize the risk of future TTP recurrences.
Strengths and limitations
This case report provides a detailed account of a rare adult-onset presentation of cTTP, genetically confirmed through biallelic ADAMTS13 mutations. A major strength lies in the thorough documentation of clinical symptoms, laboratory findings, treatment course, and genetic analysis, which may aid clinicians in recognizing atypical TTP presentations. Additionally, the discussion of differential diagnoses and interpretation of diagnostic scoring systems such as PLASMIC add educational value.
However, the report is limited by its nature as a single-patient observation, without complete genetic family testing or follow-up beyond 3 years. Therefore, caution is advised in generalizing findings, and further studies are needed to better understand late-onset cTTP and its triggers.
Conclusion
Congenital TTP is an ultrarare condition resulting from inherited deficiency of ADAMTS13, typically manifesting as recurrent episodes of MAHA. The present case is notable for its atypically late onset, with pronounced renal impairment at first presentation—an uncommon feature in cTTP.
Given the rarity of TTP, early recognition requires a high degree of clinical suspicion, particularly in the presence of MAHA and thrombocytopenia. Rapid diagnostic confirmation and timely initiation of treatment are critical. Differential diagnoses such as malignant hypertension, severe preeclampsia, systemic infections (eg, sepsis), and autoimmune conditions like systemic lupus erythematosus must be systematically excluded due to overlapping clinical features.
Footnotes
Acknowledgements
The authors thank the patient for her kind cooperation and willingness to share her clinical information.
Ethical considerations
Ethical approval was not required for this case report.
Consent to participate
Written informed consent was obtained from the patient for publication of her medical history.
Author contributions
Athanasios Chatzisfetkos: Patient care, clinical data collection, drafting of the manuscript. Carsten Bergmann: Genetic analysis, interpretation of sequencing results, manuscript review. Ulf Janssen: Clinical supervision, literature review, manuscript revision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.