
Abstract
We report a rare case of childhood-onset Minimal Change Disease (MCD) in a 31-year-old male, originally diagnosed at age 2.5 with nephrotic syndrome. Repeated biopsies throughout his childhood and adolescence revealed normal glomeruli on light microscopy and diffuse effacement of podocyte foot processes on electron microscopy, confirming pure MCD. Despite multiple relapses, prolonged corticosteroid therapy, and adjunctive immunosuppressants including cyclosporine, tacrolimus, and 2 courses of Rituximab, the patient developed progressive renal decline culminating in end-stage renal disease (ESRD) and initiation of maintenance hemodialysis in August 2025. His course also included an ischemic stroke at age 20. This case illustrates an atypical, aggressive phenotype of MCD, without transformation to focal segmental glomerulosclerosis, that challenges the conventional prognosis of MCD and underscores the need for long-term monitoring and reporting of such exceptional cases.
Keywords
Introduction
Minimal change disease (MCD) is the leading cause of idiopathic nephrotic syndrome in children, accounting for roughly 70% to 90% of cases in children older than 1 year, but is much less common in adults (approximately 10%-15%). 1 MCD is a podocytopathy characterized histologically by near-normal glomeruli on light microscopy and diffuse effacement of podocyte foot processes on electron microscopy. 1 Podocyte dysfunction, including alterations in nephrin and other slit-diaphragm proteins, and immune-mediated circulating factors have been implicated in its pathogenesis; recent studies have described circulating anti-nephrin autoantibodies in a subset of patients with active disease. 1 Nephrotic syndrome, characterized by periorbital, scrotal, labial, and lower limb edema, is the most common presenting manifestation of minimal change disease (MCD). 1 The edema results from decreased oncotic pressure, leading to ascites, pleural and pericardial effusions, and ultimately anasarca. In many cases, these symptoms are preceded by an upper respiratory tract infection. 1
Most patients, particularly children, respond to corticosteroids and have a favorable prognosis; however, relapses are common, and a minority develop steroid-dependence or steroid-resistance, necessitating second-line immunosuppression such as calcineurin inhibitors or biologic therapies (eg, rituximab). 2 Although the use of rituximab was confirmed for refractory MCD, and complete remission at a higher rate, there are still reported incidence where relapse can still occur according to Feder et al.3,4
We report a 31-year-old man with childhood-onset MCD who progressed to ESRD despite prolonged corticosteroids and multiple immunosuppressive therapies, highlighting the rare, atypical progressive form of MCD despite stable histology.
Case Presentation
A 31-year-old Palestinian male was diagnosed with nephrotic syndrome at the age of 2 and a half years after presenting with periorbital edema, mild generalized body swelling, and frothy urine, without hematuria or respiratory distress. He was treated with high-dose corticosteroids, achieving partial remission but experiencing multiple relapses whenever the medication was tapered. Because of frequent relapses and incomplete remissions despite prolonged corticosteroid therapy, several renal biopsies were performed during childhood and adolescence to reassess disease activity and exclude histologic progression to focal segmental glomerulosclerosis (FSGS). Light microscopy consistently showed normal-appearing glomeruli without segmental sclerosis, while electron microscopy demonstrated diffuse effacement of more than 80% to 90% of podocyte foot processes and absence of immune deposits, confirming minimal-change disease (MCD) and excluding FSGS.
His clinical course was consistent with steroid-dependent nephrotic syndrome rather than purely steroid-sensitive disease, as he achieved remission with corticosteroids but relapsed whenever the dose was tapered, ultimately requiring long-term maintenance therapy to sustain remission. He received prolonged corticosteroid therapy with several immunosuppressive agents, including cyclosporine (ages 9-11), tacrolimus (ages 14-16), and 2 courses of rituximab in May 2024 and June 2025.
At the age of 20, he developed an ischemic stroke confirmed by brain computed tomography, presenting with residual right-sided weakness and dysarthria. The event could possibly be associated with long-term nephrotic syndrome complications, caused by hyperlipidemia and urinary loss of natural anticoagulants such as antithrombin III, protein C, and protein S, rather than direct steroid toxicity. His regimen was subsequently adjusted to include antiplatelet therapy and stricter blood pressure control, with partial neurological recovery but persistent right-sided spastic hemiparesis. Neurological examination revealed flexion deformity of the right upper limb, reduced power in the right lower limb, increased tone, brisk reflexes, and an upgoing right plantar response (positive Babinski sign). His right thumb and hand remained partially flexed, and he exhibited mild facial asymmetry and impaired fine motor control, consistent with a chronic upper motor neuron lesion.
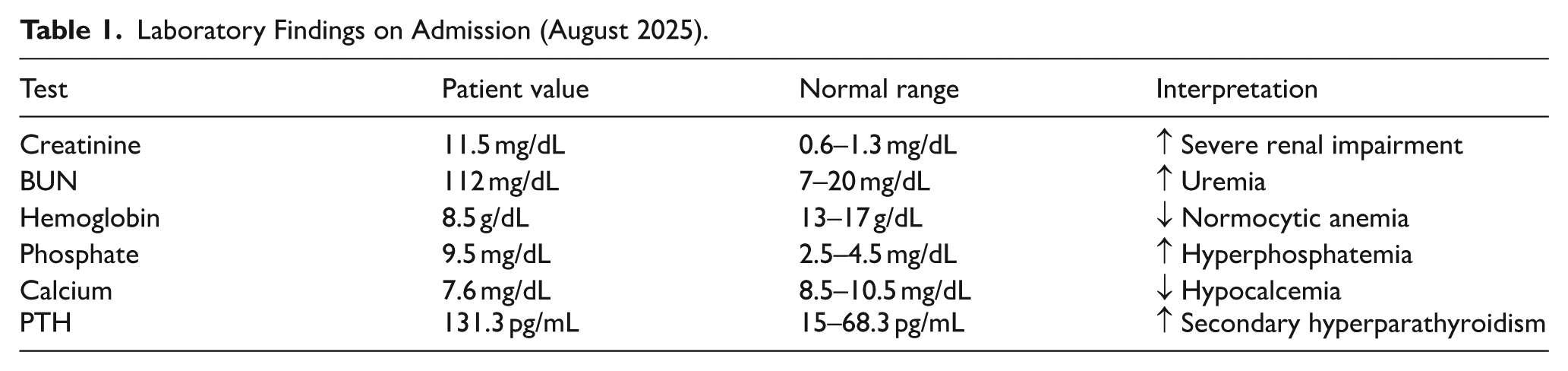
Despite intermittent responsiveness to steroids, his renal function progressively deteriorated. In August 2025, he presented with uremic symptoms and volume overload. Laboratory evaluation demonstrated severe renal impairment summarized in Table 1 with anemia, hyperphosphatemia, hypocalcemia, and markedly elevated parathyroid hormone, consistent with CKD-mineral bone disorder. Ultrasound revealed bilaterally small, echogenic kidneys with loss of corticomedullary differentiation, confirming ESRD.
Laboratory Findings on Admission (August 2025).
He started thrice-weekly hemodialysis through a right internal jugular tunneled catheter, which he tolerated well with stable vital signs.
He remained clinically stable on maintenance hemodialysis and was planned for long-term nephrology follow-up. Management included creating a permanent arteriovenous fistula, optimizing blood pressure, and CKD–mineral bone disorder parameters, starting erythropoietin and iron for anemia, and assessing suitability for future kidney transplantation.
The writing of this case report complied with the CARE checklist guidelines (Supplemental Material). 5
Figure 1 illustrates the clinical course of our patient.

Visual timeline of clinical course.
Discussion
Minimal Change Disease (MCD) usually has a favorable prognosis; however, it can rarely lead to renal failure without progression into Focal Segmental Glomerulosclerosis. 6 Such a scenario is more prominent among patients who are initially resistant to treatment or those who develop secondary resistance. 7
Typically, MCD in the pediatric age groups is the most common cause of idiopathic nephrotic syndrome and responds well to steroids, while relapses are common, progression into ESRD is fairly rare. 8 It is a less common cause of nephrotic syndrome among adults, but still associated with a good prognosis, even if associated with transformation into FSGS. 9
This case is considered atypical due to multiple biopsies excluding FSGS, which is commonly associated with MCD progression into ESRD. 10 Use of steroids and other immunosuppressive therapies over a lifetime, with failure to taper medications repetitively. Lastly, eventual loss of renal function leading to dialysis dependency.
MCD was named as so due to minimal changes among microscopy, where the main change seen is effacement of foot processing on the electron microscope, with no findings on light microscopy. Even though renal biopsy is not commonly indicated unless the clinical scenario suggests an alternative diagnosis, our patient presented with recurrent relapses among tapering medications, prompting the need for a renal biopsy, which excluded other etiologies of glomerulonephritis.
MCD in children usually presents as edema; preorbital, scrotal, or labial, and in lower extremities, in some cases, anasarca might be seen with pleural, pericardial effusions, and ascites, adding abdominal pain, dyspnea, and cold extremities to the presentation. 11 Sepsis or other severe infections, such as peritonitis or pneumonia, might be present at the time of diagnosis or during the disease course; this is thought to be attributed to Ig depletion during the disease. 11
The treatment of MCD relies heavily on corticosteroid therapy as the first-line treatment; other immunosuppressive therapies, including B-cell targeted therapies, are also found to be effective, which suggests an autoimmune component to the pathophysiology of MCD, where nephrin autoantibodies have been discovered in both children and adults with MCD.11,12
In a recent case report exploring novel treatment options, a 45-year-old man with steroid-resistant MCD leading to End Stage Renal Failure and prompting dialysis, the study shows significant improvement in renal function after a combination of supportive measures and supplementation. 7 Another case study of adult-onset Minimal Change Disease shows the regaining of renal function after intermittent dialysis for an acute phase flare. 13
In observational cohort studies looking into nephrotic syndrome in childhood, a small percentage of steroid-resistant or relapsing patients had progressed into End Stage Renal Failure or Chronic Kidney Disease. While not all cases were pure MCD, a study showed 37.5% progression into ESRD another showed about 3% progression into CKD.14,15
Reporting atypical, progressive forms of MCD is important because they challenge the conventional expectation that MCD is uniformly steroid-responsive with excellent long-term renal survival. In our childhood-onset MCD with repeated relapses, prolonged exposure to multiple immunosuppressants (including cyclosporine, tacrolimus) and rituximab, and eventual progression to ESRD without histologic transformation to FSGS on repeated biopsies illustrates a less common, progressive phenotype. Possible contributory mechanisms include cumulative podocyte injury from repetitive relapses/protein-loss, calcineurin-inhibitor-associated chronic nephrotoxicity, and unrecognized circulating pathogenic factors (eg, anti-nephrin antibodies described in recent series).12,16,17
Similar case reports and small series emphasize the heterogeneity of adult MCD and the need for individualized management. For example, recent case reports in the adult population have highlighted diagnostic and therapeutic challenges and underscore the need to document atypical courses.4,12,13
It’s crucial to report such cases and to keep a long-term follow-up record for these patients even after achieving full remission to help better understand the spectrum of MCD progression and update clinical guidelines accordingly, which may further prompt better diagnostic modalities and treatment options, especially for atypical cases that may fail conventional interventions.
Conclusion
This case demonstrates a rare progressive course of childhood-onset Minimal Change Disease that advanced to end-stage renal disease despite preserved histology and multiple immunosuppressive therapies. It emphasizes that a small subset of patients may deteriorate even without transformation to focal segmental glomerulosclerosis, highlighting the importance of long-term follow-up and reassessment when the clinical trajectory is atypical.
Although this report contributes valuable insight into an exceptionally rare trajectory, its limitations include reliance on a single case and lack of longitudinal biomarker data, which restricts the ability to draw mechanistic conclusions. Broader longitudinal cohorts and systematic reporting of similar cases are needed to refine risk stratification, optimize immunosuppressive strategies, and guide referral for advanced therapies such as transplantation.
Supplemental Material
sj-docx-1-icr-10.1177_11795476251413414 – Supplemental material for When Minimal Becomes Massive: A Case Report of Childhood-Onset Minimal Change Disease Marching to End Stage Renal Disease Despite Modern Immunotherapy
Supplemental material, sj-docx-1-icr-10.1177_11795476251413414 for When Minimal Becomes Massive: A Case Report of Childhood-Onset Minimal Change Disease Marching to End Stage Renal Disease Despite Modern Immunotherapy by Momen Zetawi, Hossam Salameh, Malak K. Assi, Shahd Aldarak and Safa’ Ramez Altiti in Clinical Medicine Insights: Case Reports
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
All procedures performed in this report involving human participants were in accordance with the ethical standards of the institutional, national research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Authors confirm that all mandatory laboratory health and safety procedures have been complied with in the course of conducting any experimental work reported in this paper.
Consent to Participate
Authors obtained verbal and written informed consent from the patient regarding this case and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author Contributions
Dr. Momen Zetawi contributed to the writing of the original manuscript and provided essential resources. Dr. Hossam Salameh participated in writing and editing the manuscript and was responsible for visualization. Dr. Malak Assi and Dr. Shahd Aldarak contributed to drafting the original manuscript. Dr. Safa’ Ramez Altiti provided supervision throughout the development of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.