
Abstract
Introduction:
Polydrug overdose, defined as the simultaneous ingestion of multiple toxic substances, is increasingly encountered in emergency departments. Overlapping toxidromes often obscure the causative agents, complicating diagnosis and management. Acetaminophen (APAP) overdose can cause hepatotoxicity through N-acetyl-p-benzoquinone imine (NAPQI) formation, metoclopramide may precipitate acute extrapyramidal symptoms, and metronidazole can induce neurotoxicity, typically a cerebellar syndrome.
Case Summary:
Young adult male medical student intentionally ingested 12 g of APAP, 170 mg of metoclopramide, and 8 g of metronidazole. He presented 24 hours later with repeated vomiting, tremor, rigidity, dysarthria, gait ataxia, and transient confusion. Vital signs were stable; laboratory tests showed transaminase elevation and coagulopathy. Peak AST/ALT were 100/76 U/L and INR peaked at 1.74. Management included oral N-acetylcysteine for APAP toxicity, intravenous diphenhydramine and diazepam for extrapyramidal symptoms, supportive ICU care, and psychiatric intervention. Coagulopathy was corrected with fresh frozen plasma. Neurological and hepatic abnormalities resolved within 72 hours, and the patient remained asymptomatic at 2-week follow-up. The patient recovered fully after N-acetylcysteine and supportive care, illustrating the diagnostic challenges of overlapping toxidromes.
Conclusion:
This case highlights the diagnostic and therapeutic challenges of polydrug overdose with overlapping toxidromes. Rapid identification and agent-specific management, including NAC for APAP, symptomatic therapy for metoclopramide and metronidazole toxicity, and supportive care, resulted in full recovery without long-term sequelae. Emergency clinicians should maintain high suspicion for multiple co-ingestants and use targeted interventions to optimize outcomes.
Keywords
Introduction
Polydrug overdose, the simultaneous ingestion of multiple toxic substances, is increasingly encountered in emergency departments.1,2 Recent ED data show most overdose patients test positive for 2 or more drugs, commonly involving sedatives, stimulants, or analgesics. 1 Polydrug use greatly complicates management because overlapping toxidromes can obscure the offending agents.2,3 In this report, a young adult ingested large doses of acetaminophen (APAP), metoclopramide, and metronidazole. Each drug has distinct toxicological effects. APAP, a ubiquitous analgesic, is normally safe but in overdose generates the reactive metabolite N-acetyl-p-benzoquinone imine (NAPQI). 4 When glutathione is depleted, NAPQI causes oxidative stress and centrilobular hepatocyte necrosis.4,5 Acetaminophen overdose is the leading cause of acute liver failure in the United States and Europe. 4 The Rumack-Matthew nomogram is used after a single acute acetaminophen ingestion to plot serum acetaminophen concentration against time from ingestion and predict risk of hepatotoxicity; concentrations above the treatment line indicate need for N-acetylcysteine.5,6 Metoclopramide is a dopamine D2 antagonist antiemetic; overdose can precipitate acute extrapyramidal reactions (dystonia, tremor, rigidity) within hours.7,8 Metoclopramide also has prokinetic 5-HT4 agonist activity and is used clinically for gastro-esophageal reflux disease and gastroparesis. 7 Metronidazole, an antibiotic, crosses the blood-brain barrier easily. 9 Prolonged or massive exposure can cause central neurotoxicity: most often a cerebellar syndrome with ataxia and dysarthria.3,9
This case is noteworthy because simultaneous ingestion produced overlapping hepatic and neurological toxicity that created a diagnostic and management challenge not well documented for this particular drug combination.1,2 Neuroimaging and rapid toxicology assays were not available at presentation, underscoring how clinicians in resource-limited settings must rely on the temporal evolution of symptoms, focused bedside assessment, and clinical reasoning to guide treatment. 10 By describing the timeline, diagnostic reasoning, interventions, and full recovery, this report provides practical, agent-specific learning points for emergency and toxicology clinicians working where confirmatory testing may be limited.2,10
Case Summary
A 19-year-old male medical student was brought to the emergency department 24 hours after intentional ingestion of 12 g of acetaminophen, 170 mg of metoclopramide, and 8 g of metronidazole. The act was impulsive, associated with a 2-year history of emotional instability and recent hopelessness. Shortly after ingestion, he developed repeated vomiting. About 20 hours later, he developed neck stiffness, generalized rigidity, bilateral hand tremors, marked dysarthria, gait ataxia, and transient confusion. The neck stiffness was interpreted clinically as an acute extrapyramidal/dystonic reaction related to metoclopramide (given the concurrent limb tremor/rigidity).
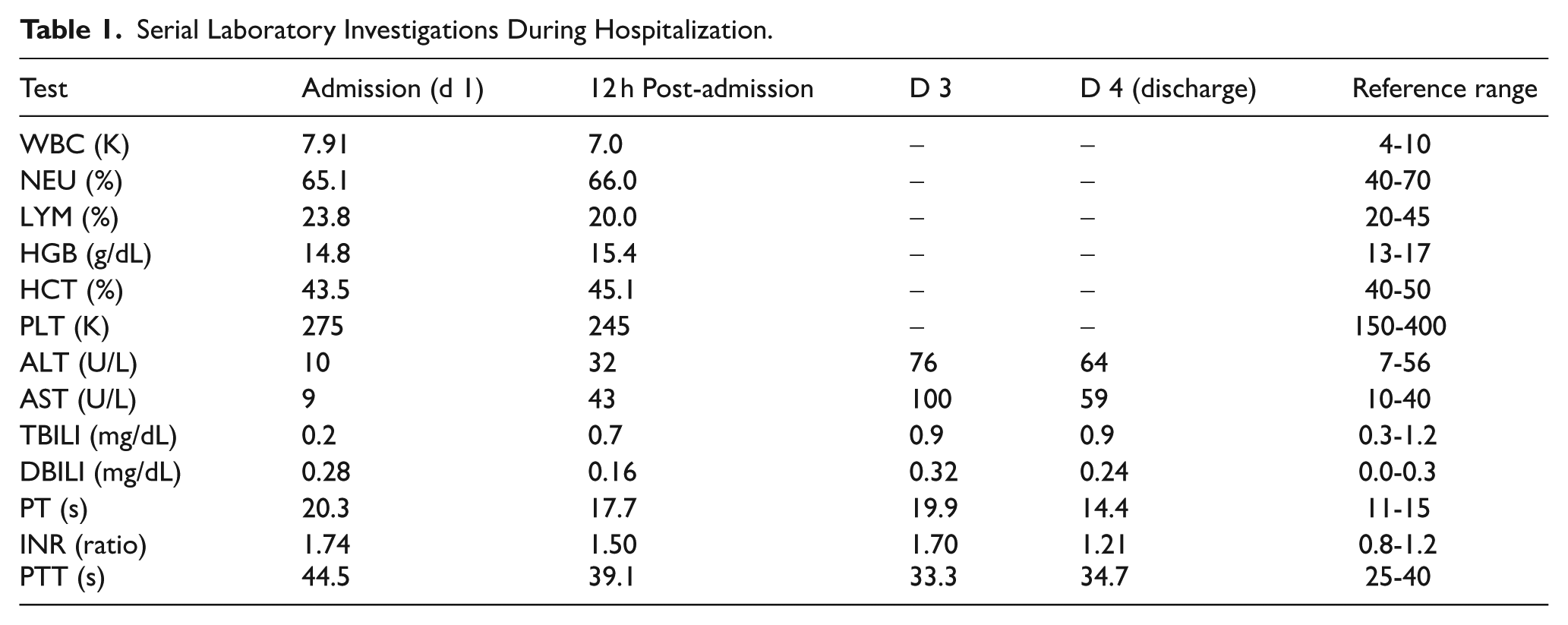
On admission, vital signs were stable, and the patient was confused and lethargic (GCS 14/15). Neurological examination revealed dysarthria, gait ataxia, tremors, and neck rigidity. Cranial nerves were intact, and no focal motor or sensory deficits were present. Chest and cardiac examinations, as well as abdominal examination, were unremarkable. Serial laboratory results are summarized in Table 1 (extracted from the patient’s hospital medical record and laboratory reports).
Serial Laboratory Investigations During Hospitalization.
Management was guided by ingestion history and risk of hepatotoxicity. Oral N-acetylcysteine (NAC) was initiated immediately (because the history indicated ingestion >4 g and transaminases began to rise) following the standard 21-dose protocol. Neurological symptoms, including tremor, rigidity, confusion, and lethargy, were treated with intravenous diazepam, while diphenhydramine was used for extrapyramidal symptoms due to metoclopramide overdose. Supportive care included intravenous fluids with dextrose to maintain hydration and metabolic stability.
Persistent coagulopathy prompted administration of 3 units of fresh frozen plasma (FFP). Serial monitoring revealed a peak in liver transaminases on day 3, followed by normalization by day 4. Neurological deficits improved within 48 hours and resolved completely by 72 hours. Brain MRI, unfortunately was unavailable and was not done thus the attribution of neurological findings was made on temporal pattern, focused exam, exclusion of metabolic causes, and clinical response to therapy. Renal function tests, serum electrolytes, and blood glucose levels were all within normal ranges throughout hospitalization.
Psychiatric assessment post-stabilization identified borderline personality disorder (BPD). The patient was provided with psychoeducation, a safety plan, and arranged for outpatient follow-up. He was discharged on hospital day 4 in stable condition (Table 2). At 2-week follow-up, the patient remained asymptomatic with no recurrence of neurological or hepatic abnormalities.
Timeline of Ingestion, Presentation, Key Laboratory Abnormalities, Interventions, and Recovery.

Discussion
Acetaminophen overdose is common and often involves co-ingestants. 5 In many series of ED overdoses, up to a third involve multiple drugs.1,2,11 In 1 large Spanish ED study, most intoxicated patients had at least 2 substances detected. 1 Common combinations include alcohol, benzodiazepines, opioids, or stimulants2,11; antiemetics and antibiotics, as in this case, are less typical co-drugs. However, any large suicide attempt may include whatever substances are on hand. 12 The combination of APAP with metoclopramide (often available at home) and metronidazole (prescribed antibiotic) is unusual. Nevertheless, this case underscores that clinicians must consider all possible co-ingestants, especially when symptoms cross classic toxidromes. Clinicians and health systems in resource-limited settings should explore emerging technologies to improve diagnostic accuracy, risk-stratification, and triage for toxicology presentations, while addressing local data, infrastructure, and ethical barriers. 13 Polydrug overdoses in general have higher morbidity: hospitalization and intensive care are more frequent compared to single-drug cases.1,2 Psychiatric comorbidity (eg, borderline personality disorder) often underlies deliberate multi-drug ingestion and should prompt psychiatric assessment after acute care.1,12
This patient’s presentation exemplifies overlapping toxidromes. APAP toxicity is initially often asymptomatic except for gastrointestinal upset; delayed hepatic injury appears after ~24 hours. 4 By 24 hours this patient indeed had RUQ pain and coagulopathy. The combination of tremor/rigidity (suggestive of drug-induced Parkinsonism/dystonia) with dysarthria and ataxia, in this case, suggested a contribution from metoclopramide and metronidazole (Table 3). Dystonic reactions to metoclopramide can be mistaken for seizures or tetanus if unrecognized. 7 Indeed, Malakian et al noted such reactions are easily misdiagnosed unless the drug history is known. 8 We acknowledge hepatic encephalopathy as an important differential for the transient confusion; however, the absence of asterixis, only modest hepatic dysfunction, and the rapid neurological recovery in this patient made HE less likely, although it cannot be definitively excluded without ammonia measurement or additional testing.3,4 Neuroimaging, if performed, excludes acute stroke or cerebellar infarct. 14 Serum studies can aid diagnosis: a toxic APAP level can confirm risk of hepatic injury and guide NAC therapy. 5 In our setting, serum APAP measurement was not available, so management was guided by the reported ingestion history and clinical risk factors. No rapid “blood level” exists for metoclopramide or metronidazole; their diagnosis is clinical.3,7 Electrolytes, ammonia, and other toxin screens were likely used to rule out alternative causes of encephalopathy. 6 Overall, recognizing the overlapping features and knowing that metoclopramide can cause dystonia. 8 Metronidazole can cause cerebellar signs3,14 was key to diagnosis.
Summary of Each Ingested Drug With Mechanism, Expected Toxicity, and Key Management Considerations.

Abbreviations: APAP, acetaminophen; NAC, N-acetylcysteine.
Management of this polydrug overdose followed standard principles. For acetaminophen toxicity, prompt antidote therapy is critical. 6 Guidelines recommend NAC for any ingestion >200 mg/kg or >10 g in a single dose.5,6 In this case, ingestion of 12 g (exceeding the toxic threshold) mandated treatment. 5 NAC was given orally on a 72-hour regimen, as intravenous NAC was not available. Activated charcoal should be given within 4 hours of ingestion to reduce absorption of APAP6,15; it was too late for this patient at 24 hours. During APAP overdose, coagulopathy often develops (elevated INR); vitamin K and fresh frozen plasma (FFP) can be used for supportive correction if bleeding risk is high. 19 In this case, FFP was used to correct the INR prior to invasive procedures. For metoclopramide-induced dystonia. Diphenhydramine 25 to 50 mg IV or IV benztropine are first-line treatments.7,8 Benzodiazepines (eg, diazepam) may also relieve muscle spasms and anxiety. 16 In our patient, IV diphenhydramine and diazepam were given, leading to rapid improvement of rigidity and tremor. For metronidazole neurotoxicity, the primary intervention is drug discontinuation, and no specific antidote exists.3,14,17 Supportive care and withdrawal typically lead to recovery. 17 Some reports have used steroids or antioxidants, 17 but evidence is limited. In severe cases, plasmapheresis has been suggested,14,17 though we did not need it. In this patient, treatment included oral NAC for hepatic protection, supportive care, intravenous diphenhydramine and diazepam for dystonia and tremor, and general ICU support. Psychiatric and social interventions were arranged after stabilization.
The prognosis in this case was favorable, consistent with literature. Acetaminophen-induced liver injury is usually reversible if NAC is given promptly.4,6 In cohorts, early NAC reduces the risk of liver failure to <10%. 6 Our patient’s liver enzymes peaked by 48 to 72 hours and then normalized, avoiding acute liver failure or the need for transplantation. 4 Neurologically, extrapyramidal symptoms from metoclopramide resolve quickly once treated; most acute dystonias abate within hours of anticholinergic therapy. 8 Metronidazole neurotoxicity also tends to be fully reversible. 17 In a series of cases, >90% of patients had complete or near-complete symptom resolution after stopping metronidazole, and symptoms usually improve over 2 to 14 days. 14 This patient’s dysarthria and ataxia began improving over 48 hours. There is little evidence of chronic sequelae if patients recover acutely. 18 Overall, timely recognition and management led to full recovery by 72 hours, without long-term hepatic or neurologic damage.
Conclusion
This polydrug overdose case highlights several lessons for emergency and toxicology practice. First, clinicians should suspect multiple co-ingestants when features span different toxidromes, especially in intentional overdose. Second, management must address each agent: NAC for acetaminophen toxicity, decontamination if indicated, and symptom-directed therapy (anticholinergics/benzos for extrapyramidal symptoms). Finally, outcomes are good if therapy is rapid and appropriate. In this case, early NAC likely prevented liver failure, and withdrawal of metoclopramide/metronidazole plus supportive care allowed neurologic recovery. Emergency physicians should maintain a high index of suspicion for uncommon toxicities and use targeted treatments to optimize prognosis.
Footnotes
Acknowledgements
We thank the patients and their families for agreeing to give their consent to publish their clinical records for this series.
Author Note
All authors conducted the work at Addis Ababa University, Addis Ababa, Ethiopia.
Ethical Considerations
IRB review and approval were waived for this case report.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
AAW writing—original draft, conceptualization, data curation. BTM conceptualization and writing—original draft. CTM visualization, writing—review and editing. AG resources, data curation. SAW visualization, writing—review and editing. EAA supervision. SMB resources, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying the results presented in this work are available within the manuscript.