
Abstract
Background:
Takayasu arteritis (TA) is a rare chronic vasculitis primarily affecting the aorta and its major branches, often presenting diagnostic challenges due to nonspecific symptoms, particularly in adolescents. This case highlights a rare adolescent-onset TA with unique vascular findings in Pakistan.
Case presentation:
A 17-year-old female presented with a 1-year history of fever, 40 kg weight loss, and vague abdominal discomfort. Physical examination revealed absent left arm pulses, vascular bruits, and asymmetric blood pressure. Laboratory tests showed anemia, elevated inflammatory markers (ESR 62 mm/h, CRP 66 mg/L), and hyperferritinemia. CT angiography confirmed thoracic aortic mural thickening, left subclavian artery occlusion, vertebral steal syndrome, and nonbifurcating carotid arteries. The diagnosis of TA was established using modified Ishikawa and 1990 ACR criteria.
Management and outcomes:
The patient received pulse methylprednisolone, monthly cyclophosphamide, and antihypertensives. Symptoms resolved within 3 months, with normalized inflammatory markers and stable vascular status at 1-year follow-up.
Conclusion:
This case underscores the importance of considering TA in adolescents with constitutional symptoms and pulse deficits. Early imaging and immunosuppressive therapy led to favorable outcomes. Vertebral steal syndrome and nonbifurcating carotid arteries add educational value, emphasizing clinical vigilance in resource-limited settings.
Introduction
Takayasu arteritis (TA) is a rare, idiopathic, chronic granulomatous vasculitis that predominantly affects the aorta and its major branches. It typically presents in young females under the age of 40, with the highest prevalence reported in South and East Asia.1,2 First described by Mikito Takayasu in 1905 in a Japanese woman with characteristic retinal arteriovenous anastomoses, the disease was later understood to involve systemic large-vessel inflammation and is now formally classified by the Chapel Hill Consensus Conference as large-vessel vasculitis involving granulomatous inflammation of the aorta and its major branches.3,4
The global incidence of TA is estimated at 1.2 to 2.6 cases per million annually, with a marked female predominance ranging from 8:1 in Japan to approximately 3:1 in Western populations.5,6 However, epidemiological data from Pakistan remain sparse, particularly for adolescents. Although the exact etiology remains elusive, a combination of infectious triggers (notably Mycobacterium tuberculosis), autoimmunity, and genetic susceptibility—such as associations with HLA-B*52 and other class I and II alleles—has been implicated.6,7
Clinically, TA follows a biphasic course: an initial nonspecific systemic phase marked by fever, malaise, arthralgias, and weight loss, often leading to diagnostic delay, followed by a chronic vascular phase characterized by arterial bruits, limb claudication, pulse deficits, and blood pressure discrepancies due to stenosis or occlusion of major arteries. 2 The most commonly involved vessels are the subclavian, common carotid, and renal arteries, leading to neurological symptoms, renovascular hypertension, and end-organ ischemia. 8
Early diagnosis is critical yet challenging because of its variable presentation and often subtle early manifestations. Advanced imaging modalities such as contrast-enhanced CT angiography and color Doppler sonography (eg, the “macaroni sign”) are pivotal in identifying vessel wall thickening and luminal stenosis even before clinical signs appear. 9 Laboratory markers such as an elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are helpful, although nonspecific.
Here, we present the case of a 17-year-old female who presented with constitutional symptoms and was initially suspected to have a hematological malignancy. The diagnostic turning point was the absence of peripheral pulses and the presence of vascular bruits, which, combined with other findings in investigations, led to a diagnosis of TA. The purpose of reporting this case is to highlight an adolescent-onset presentation of TA with the rare coexistence of vertebral steal syndrome and bilateral non-bifurcating carotid arteries. While each of these findings has occasionally been reported in isolation, their simultaneous occurrence in a young patient is exceptionally rare and, to our knowledge, has not been previously described in the South Asian context.10,11 This case underscores the importance of clinical vigilance and the importance of considering the TA in the differential diagnosis of young patients with constitutional symptoms and asymmetric pulses, especially in underrepresented geographic regions.
Case History
A 17-year-old female presented to the medical ward of Benazir Bhutto Hospital, Rawalpindi, with a 1-year history of intermittent low-grade fever (up to 101°F), generalized body aches more prominent at night, progressive weight loss totaling approximately 40 kg, and vague abdominal discomfort not localized to a specific quadrant. She also reported a reduced appetite and irregular menstrual cycles with hypomenorrhea. She denied any history of cough, chest pain, or dyspnea. There was no history of headache, blurred vision, or jaw claudication. She also reported no bowel habit changes, urinary complaints, or neurological deficits. Similarly, there was no history of dizziness, syncope, or blurred vision associated with upper limb activity such as combing hair. Her medical history was unremarkable, with no known comorbidities. She had received a single packed red cell transfusion 1 year prior for microcytic anemia but had not been previously hospitalized for other complaints.
On physical examination, she appeared chronically ill, lean, and pale. Her vital signs revealed a pulse rate of 110 bpm and a blood pressure of 140/70 mmHg in the right arm; however, blood pressure could not be measured on the left arm. Pulses were absent in the left brachial and radial arteries. Auscultation revealed bruits over both common carotid arteries, the abdominal aorta, and the left renal artery. Cardiorespiratory and abdominal exams were otherwise unremarkable, and she was neurologically intact.
Laboratory tests revealed anemia (Hb: 8.4 g/dL; reference: 12-16 g/dL), elevated inflammatory markers (ESR: 62 mm/h; reference: <20 mm/h; CRP: 66 mg/L; reference: <5 mg/L), leukocytosis (WBC: 15.2 × 10³/µL; reference: 4-11 × 10³/µL), and elevated serum ferritin (1505 ng/mL; reference: 13-150 ng/mL). The serum iron concentration was low (22.6 µg/dL; reference: 50–170 µg/dL), with an increased total iron-binding capacity (398 µg/dL; reference: 240–450 µg/dL). Liver and renal function panels were within normal limits. Serologies for HIV, hepatitis B, and hepatitis C were negative.
Methods
Given the constellation of constitutional symptoms, anemia, and increased inflammatory markers, a hematological malignancy was initially suspected. However, the absence of upper limb pulses and the presence of vascular bruits prompted further vascular evaluation.
Transthoracic echocardiography revealed mild left ventricular systolic dysfunction (ejection fraction 45%-50%) with hypokinesis of the septal wall but no valvular abnormalities. Carotid Doppler ultrasound demonstrated circumferential thickening of the common carotid arteries, which was consistent with the “macaroni sign.” Abdominal ultrasound revealed bilateral mild renal fullness without evidence of hydronephrosis or a mass.
CT angiography of the thorax and abdomen demonstrated circumferential mural thickening with luminal narrowing of the thoracic aorta, along with complete non-opacification of the proximal left subclavian artery. However, no abnormalities were noted in the abdominal aorta or renal arteries. Collateral circulation was observed through the ipsilateral vertebral artery, confirming the presence of vertebral steal syndrome (Figure 1). Additional findings included segmental narrowing of the left axillary and brachial arteries, as well as bilateral non-bifurcating common carotid arteries, a rare anatomical variant (Figure 2).

CT angiogram demonstrating circumferential mural thickening of the arch of aorta and descending thoracic aorta with left subclavian artery occlusion and vertebral steal phenomenon.

CT angiogram revealing bilateral non-bifurcating common carotid arteries.
Based on these radiological findings, together with the clinical presentation, a diagnosis of Takayasu arteritis was established. The diagnosis was supported by the Modified Ishikawa criteria (major criterion: left subclavian artery lesion; minor features: constitutional symptoms and pulse deficit) and by fulfilling the American College of Rheumatology 1990 classification criteria (age < 40 years, pulse deficit, blood pressure discrepancy > 10 mmHg, vascular bruits, and angiographic abnormalities).12,13 The lesion was classified as a Type 2b lesion according to the Numano and Kobayashi classification for Takayasu arteritis. 4
Conclusion and results
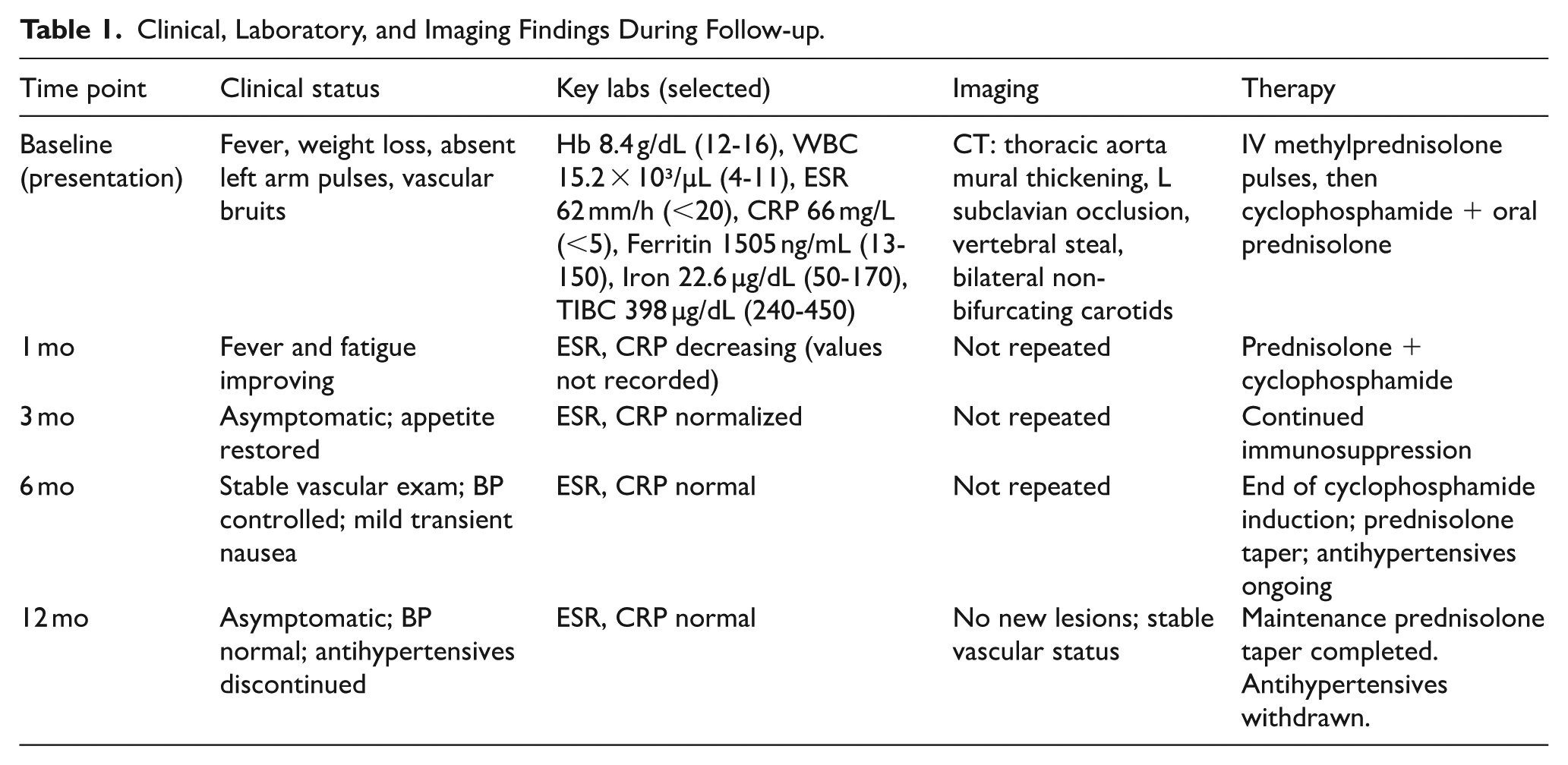
Following diagnosis, the patient received 3 days of intravenous pulse methylprednisolone (1 g daily), followed by monthly intravenous cyclophosphamide (1 g per NIH protocol) and mesna for uroprotection. Oral prednisolone was initiated and gradually tapered over the subsequent 6 months. Concurrently, newly diagnosed hypertension was managed with a combination of amlodipine (5 mg) and valsartan (80 mg) once daily.
Constitutional symptoms, including fever, fatigue, and appetite loss, began improving within the first month and fully resolved by the third month. Inflammatory marker levels normalized, and vascular examination revealed stable pulses and blood pressure. Aside from mild, transient nausea following cyclophosphamide infusions, no significant adverse effects were reported.
By the end of the 6-month induction phase, the patient was maintained on a tapering dose of oral prednisolone. With sustained blood pressure control, antihypertensives were gradually withdrawn under clinical supervision. At the 1-year follow-up, the patient remained asymptomatic, with normal inflammatory marker levels and a stable vascular status. She continues to be monitored closely for signs of relapse. The summary of the clinical status can be seen in Table 1 below:
Clinical, Laboratory, and Imaging Findings During Follow-up.
This case represents a rare adolescent presentation of Takayasu arteritis from Pakistan, which was diagnosed during the vascular inflammatory phase before irreversible vascular damage occurred. The presence of vertebral steal syndrome and nonbifurcating carotid arteries provides additional diagnostic and educational value. Early recognition, facilitated by clinical suspicion and timely imaging, enables effective immunosuppressive therapy with favorable short-term outcomes.
Discussion
TA is a rare, chronic large-vessel vasculitis that typically affects women under 40 years of age and is characterized by granulomatous inflammation of the aorta and its major branches. The disease is often underdiagnosed in its early stages, particularly in adolescents, where the presentation may be nonspecific and constitutional in nature.13,14 This case illustrates the importance of early recognition, the diagnostic challenges posed by nonclassical symptoms, and the impact of timely immunosuppressive therapy on long-term outcomes.
Diagnostic Delay and Clinical Complexity
TA progresses through a biphasic course: an initial pre-pulseless or systemic inflammatory phase, often marked by fever, weight loss, arthralgias, and anemia, followed by a chronic occlusive phase manifesting with vascular symptoms such as claudication, pulselessness, and bruits. 14 The delay in diagnosis, often exceeding 1 year, is a well-documented problem, with misdiagnosis rates ranging from 30% to 60% globally.15-17 In our case, the initial suspicion of hematological malignancy exemplified this challenge, emphasizing the need for awareness of TA in the differential diagnosis of prolonged febrile illness with systemic inflammation in adolescents.
Key vascular signs, the absence of peripheral pulses, asymmetric blood pressures, and audible bruits should raise suspicion for large vessel vasculitis, particularly when constitutional symptoms coexist with elevated inflammatory markers. In this patient, prompt vascular imaging confirmed aortic and branch vessel involvement, including the left subclavian and carotid arteries.
Imaging and Vascular Findings
CT angiography is the gold standard for assessing luminal stenosis, wall thickening, and aneurysms in the TA. It plays a vital role in both diagnosis and disease monitoring.18,19 The identification of the “macaroni sign” on carotid Doppler, characteristic of circumferential arterial wall thickening, combined with mural thickening of the thoracic aorta and subclavian occlusion on CT angiogram confirmed the diagnosis.
Importantly, this case featured 2 rare vascular findings:
Differential Diagnosis and Similar Cases
In adolescent females with fever, weight loss, and anemia, the differential diagnosis is broad and often includes hematologic malignancies, infectious diseases such as tuberculosis, and systemic autoimmune conditions. 20 A comparative table is included for educational value (see Table 2).
Differential Diagnosis in Adolescents with Systemic Symptoms and Anemia.

Previous case reports of Takayasu arteritis with vertebral steal syndrome have highlighted the potential for neurological symptoms such as syncope, dizziness, or visual disturbance. 10 Similarly, non-bifurcating carotid arteries have been described as rare congenital variants that can complicate angiographic interpretation. 11 However, to our knowledge, no prior report has documented the simultaneous occurrence of both vertebral steal syndrome and bilateral non-bifurcating carotid arteries in an adolescent with TA. Table 3 summarizes selected published cases that reported either vertebral steal syndrome or non-bifurcating carotid arteries in association with Takayasu arteritis, allowing comparison with the present case.
Reported Cases of Takayasu Arteritis with Vertebral Steal Syndrome or Non-bifurcating Carotid Arteries.

Therapeutic Strategy and Outcomes
The cornerstone of TA treatment is high-dose corticosteroids to control vascular inflammation. However, monotherapy is associated with high relapse rates (40%-70%), necessitating early use of steroid-sparing agents in moderate to severe disease.21,22 In this case, induction therapy with pulse methylprednisolone followed by monthly cyclophosphamide for 6 months, combined with mesna for uroprotection, aligns with the National Institutes of Health protocol for severe TA. 23
The addition of cyclophosphamide was justified by the extent of vascular involvement, and this approach has been shown to achieve remission in approximately 60 to 80% of patients with major vascular lesions. 24 Our patient achieved full symptom resolution within 3 months, normalization of inflammatory markers, and sustained clinical remission at 1 year.
Hypertension is a common complication of TA and is often related to renal artery stenosis, arterial stiffness, or systemic inflammation. 25 The blood pressure normalization observed in our patient following disease control and eventual withdrawal of antihypertensives suggests that vascular inflammation, rather than fixed stenosis, was the likely driver. Nonetheless, this finding must be interpreted cautiously, as TAs are prone to relapse, and vascular remodeling may still occur. 20
Disease Monitoring and Relapse Risk
Assessing disease activity in TAs remains challenging. Conventional inflammatory markers such as the ESR and CRP lack specificity and may normalize despite active vessel inflammation. 21 Imaging techniques, including CT angiography, MRI, and PET-CT, provide more reliable markers of disease activity and are recommended for follow-up, particularly in the tapering phase. 14
Even in clinically quiescent patients, relapse rates remain significant, with a 5-year flare-up risk approaching 50% in some cohorts. 14 Long-term follow-up is thus essential. Our patient’s remission at 1 year is promising, but continued monitoring is warranted.
Educational and Regional Significance
This case represents one of the few adolescent-onset TA reports from Pakistan. This contributes to the limited regional epidemiological data and demonstrates that early diagnosis, even in resource-limited settings, can lead to favorable outcomes. This finding also reinforces the need to include TA in the differential diagnosis of adolescents with constitutional symptoms and asymmetrical pulses.
Footnotes
Acknowledgements
None.
Ethical Considerations
Ethical approval was not required for case report.
Consent to Participate
Informed, written consent was taken from the parents for the collection of data.
Consent for Publication
Informed, written consent was taken from the parents for the publication of anonymized details in a journal.
Author Contributions
Maryam Mukhtar: Conceptualization; Data Curation; Writing – original draft. Maha Iftikhar: Data Curation; Methodology; Writing – original draft. Saba Shafiq: Writing – review and editing; Methodology. Abdur Rehman: Supervision; Writing – review and editing. Rahmat Gul Omarzai: Project administration, Writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from authors upon reasonable request.