
Abstract
Amyloidosis is a broad category of diseases characterized by the extracellular accumulation of misfolded fibrillar proteins, which disrupt organ architecture and causes cellular toxicity. This ultimately results in vascular compromise and progressive organ dysfunction. Despite advances in serum free light chain assays and imaging modalities, diagnostic delays persist due to the underestimation of early signs and the need for multidisciplinary correlation. Our case report highlights a unique case of a patient with systemic AL amyloidosis involving the gastrointestinal (GI) system, who initially presented with chronic diarrhea and profound weight loss. We emphasize the diagnostic challenges in recognizing multiorgan amyloidosis, underscore the role of histopathology and advanced imaging in confirming systemic spread, and discuss the clinical implications of concurrent GI disease. In this piece, we also discuss the therapeutic treatment of amyloidosis including chemotherapy and supportive care for the major presenting symptom, diarrhea. The key lesson of our case is the importance of having a high clinical suspicion of amyloidosis in patients with unexplained GI symptoms, especially diarrhea.
Learning Points
AL amyloidosis is a complex and multisystem disorder with profound implications for patient health.
Its pathogenesis, characterized by the misfolding and aggregation of immunoglobulin light chains, leads to the formation of amyloid fibrils that cause widespread organ dysfunction.
Patient will present with non-specific symptoms that can be attributed to other GI disorders.
This case emphasizes that early and thorough workup, through the use of advanced biomarkers, imaging, and histological techniques, is crucial for diagnosis and improving outcomes.
The management of AL amyloidosis involves a comprehensive approach that targets both the underlying plasma cell dyscrasia and the systemic effects of amyloid deposition.
Introduction
Amyloidosis is a diverse group of disorders marked by extracellular deposition of misfolded fibrillar proteins, leading to progressive organ dysfunction through disruption of organ architecture and cellular toxicity. 1 Although the primary (AL) amyloidosis type is the most frequent in developed countries, it remains a rare disease with an incidence of only 14 cases per million person-years in the US. 2 AL amyloidosis usually originates from monoclonal plasma disorders that produce amyloidogenic monoclonal light chains, most commonly lambda (λ) subtypes. 3 These deposits can affect multiple organ systems. The involvement of the cardiac, renal, and gastrointestinal (GI) systems can lead to high morbidity and mortality due to a delayed diagnosis and narrow therapeutic windows. 4
We present a unique case of a patient with stomach-related systemic AL amyloidosis first presented with severe weight loss and persistent diarrhea. We address the clinical consequences of concomitant GI illness, stress the diagnostic difficulties in identifying multi organ amyloidosis, and highlight the importance of histology and imaging in diagnosis.
There is a wide differential diagnosis for subacute significant weight loss and chronic diarrhea in elderly patients. This includes celiac disease, inflammatory bowel disease, amyloidosis, eosinophilic gastroenteritis, and malignancy. This presentation requires a thorough clinical investigation to identify the etiology.
Case Presentation
A 64-year-old male smoker, known to have chronic obstructive pulmonary disease and gastroesophageal reflux disorder, presented to our clinic complaining of diarrhea and unintentional weight loss of 13 kg over a duration of 4 months. He denied any episodes of fever, night sweats, abdominal pain, nausea, vomiting, chest pain, cough, hematochezia, or melena.
On physical examination, the patient had a cachectic appearance. Pulmonary auscultation was significant for mild bilateral bibasilar crackles. Abdominal examination revealed a soft abdomen with epigastric tenderness and normal bowel sounds.
After the initial presentation, an esophagogastroduodenoscopy (EGD) and colonoscopy were planned and performed together with a basic laboratory workup as a primary investigation for our patient’s symptoms (Table 1). The endoscopic evaluation aimed to rule out organic causes of chronic diarrhea including (celiac disease, gastric and colorectal malignancy, inflammatory bowel disorder, eosinophilic gastroenteritis, microscopic colitis, and amyloidosis). Colonoscopy was unremarkable with normal mucosal appearance throughout the colon, the EGD showed a normal-appearing esophagus, accompanied with marked gastric nodularity and a friable mucosa at the gastric fundus (Figure 1) from which several biopsy specimens were taken. While awaiting biopsy results and in the absence of evidence for infectious diarrhea, the patient was started on supportive therapy with oral diosmectite for symptomatic relief, along with hydration and dietary adjustments. Pathology revealed mild chronic active gastritis with extensive deposition of amorphous material displaying apple-green birefringence with Congo red staining, consistent with amyloid.
Initial Laboratory Results for Diarrhea and Weight Loss Investigation. CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ALT, alanine aminotransferase; γ-GT, gamma-glutamyl transferase; TSH, thyroid stimulating hormone.


An EGD image demonstrating marked gastric nodularity and mucosal friability of the gastric fundus. This image shows irregular, raised and clustered nodules in the gastric fundus with surrounding erythema and mucosal friability. The background mucosa appears edematous, lacking the usual normal smooth surface.
Accordingly, an extensive workup was done to further investigate the findings on pathology and identify the type of amyloidosis. These included serum calcium, high-sensitivity troponin T, N-terminal pro-B-type natriuretic peptide, urine, and serum protein electrophoresis, immunofixation electrophoresis that turned out to be consistent with primary AL amyloidosis.
Imaging was done to assess organ involvement, including a PET-CT scan, a CT of the chest, abdomen and pelvis, and an echocardiogram. Results (Table 2) were significant for myocardial involvement.
Radiologic and Laboratory Tests for Amyloidosis Classification. EGD, esophagogastroduodenoscopy; PET-CT, positron emission tomography-computed tomography.
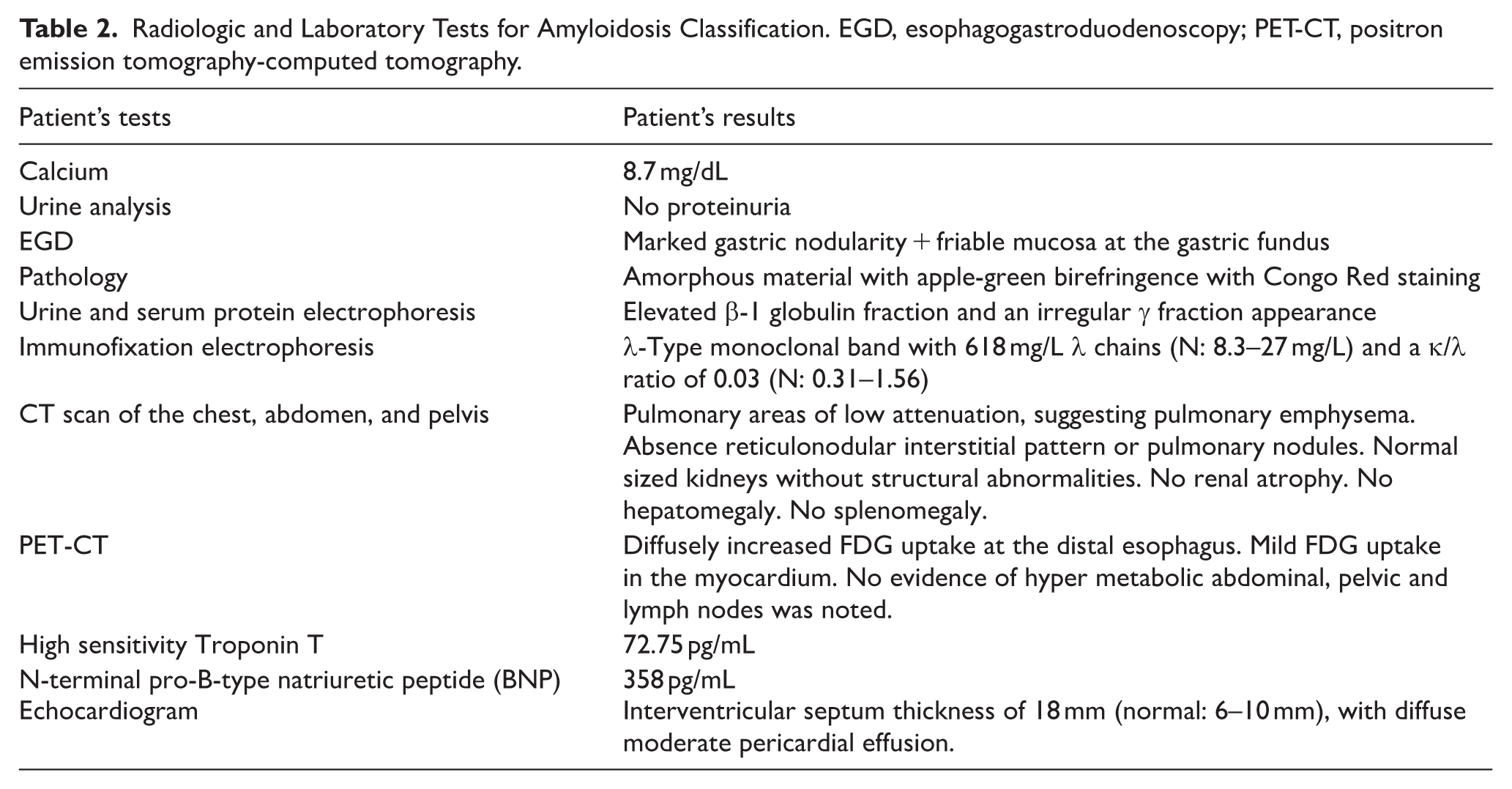
Therefore, the patient was diagnosed with primary AL amyloidosis with gastric and cardiac involvement. In the light of cardiac and gastric AL amyloidosis with pericardial effusion, this case was classified as a case of advanced disease with a poor prognosis. Accordingly, 6 cycles of DaraCyBorD (daratumumab, cyclophosphamide, bortezomib, dexamethazone) were planned as a treatment course. A followup echocardiogram was scheduled pre-chemotherapy initiation for pericardial effusion monitoring. Unfortunately, the patient passed away just before treatment initiation due to cardiac arrest secondary to pericardial effusion.
Discussion
AL amyloidosis is a rare but devastating systemic disease characterized by the deposition of amyloid fibrils formed from misfolded immunoglobulin light chains. The pathogenesis of AL amyloidosis is intricately linked to plasma cell dyscrasias, particularly monoclonal gammopathies such as multiple myeloma. Although not all patients with plasma cell disorders develop amyloidosis, the overproduction of monoclonal light chains remains a critical determinant in the pathogenesis of the disease. 3 These amyloid fibrils accumulate in a variety of tissues and organs resulting in a wide range of clinical manifestations and often significant morbidity and mortality. 1 In our case, a gastric biopsy positive for amorphous material with apple-green birefringence with Congo Red staining was the key for amyloidosis diagnosis. However, ruling out other underlying plasma cell dyscrasia and identifying amyloidosis subtype is essential. Therefore, serum calcium, high-sensitivity troponin T, urine and serum protein electrophoresis, immunofixation electrophoresis that turned out to be consistent with primary AL amyloidosis.
Organ involvement is a hallmark of AL amyloidosis, with the heart, kidneys, and gastrointestinal system being most commonly affected. 5 The patient usually presents with nonspecific signs and symptoms, hence, the suspicion index for AL amyloidosis should remain high. A thorough testing including advanced biomarkers, imaging and histologic testing, should be carried out in order to pinpoint AL amyloidosis as early as possible to ensure better, both treatment and management outcomes. In our case, myocardial and an uncommon gastric involvement was found, manifesting as diarrhea and weight loss.
Cardiac involvement is often the most challenging and life-threatening manifestation. Amyloid deposits in the heart lead to restrictive cardiomyopathy, characterized by stiffening of the myocardium, which impairs diastolic filling and causes heart failure. Early diagnosis of cardiac involvement is crucial, as heart failure due to amyloid infiltration can progress rapidly, significantly affecting patient survival. 6 Diagnostic strategies focus on biomarkers such as troponin, which was significantly elevated in our case, and N-terminal pro-B-type natriuretic peptide (BNP), 7 as well as echocardiographic findings, including the characteristic “sparkling” appearance of amyloid deposits in the myocardium. 8 Moreover, other findings can be seen on the echocardiogram, such as a diffuse pericardial effusion and thickening of the interventricular septum, which were seen in our patient. These diagnostic modalities, when used early, can help identify cardiac amyloidosis before irreversible cardiac damage occurs, providing an opportunity for timely therapeutic intervention.
Gastrointestinal involvement, though less frequently discussed, is an important and often debilitating manifestation of AL amyloidosis. It can present in numerous ways; some cases reported involuntary weight loss, nausea and vomiting, 9 some presented with bloating and epigastric discomfort, 10 some with diarrhea. Others presented with more serious symptoms like occlusion, malabsorption, 5 and GI bleeding. 11 In our case, the patient only had diarrhea and unintentional weight loss.
In primary amyloidosis, amyloid fibrils infiltrate the lamina propria and submucosa, mechanically altering the mucosal surface and reducing capillary blood flow. This hinders the natural physiologic nutritional absorption. This structural change is manifested as diarrhea and weight loss. Moreover, gastrointestinal dysmotility may be brought on by amyloid invasion of the muscular propria and enteric nervous system. This causes disturbed gastric emptying and intestinal transit delay.
Misdiagnosis can happen in the case of GI involvement mainly because of these non-specific symptoms. Diarrhea and bloating, especially after eating, can be considered as IBS, 12 regurgitations can be mistaken for gastroesophageal reflux disease, and early satiety can be mistaken for gastroparesis.
The variability of endoscopic findings in these patients also leads to misdiagnosis. Some EGD usually show nonspecific mucosal changes, like submucosal nodules or thickening, similar to the ones seen in our patient. Some lesions are often mistaken for neoplasia 13 or inflammatory processes. 14 A case report also described mesenteric nodules and peritoneal adhesions. 15 Therefore, our index of suspicion should remain high and look for other possible organ involvement in order to obtain a diagnosis and appropriately treat the patients. 16
Although clinical manifestations and imaging can help in patients with suspicion of AL amyloidosis, the diagnosis can only be done by visualizing the amyloid accumulation on tissue biopsy with Congo Red staining displaying an apple-green birefringence. 17
Because of the nonspecific symptoms and endoscopic findings, our index of suspicion should remain high in order to diagnose and manage any GI involvement.
The management of AL amyloidosis remains complex, requiring a multidisciplinary approach to address both the underlying plasma cell disorder and the systemic effects of amyloid deposition.
Plasma cell dyscrasia is typically managed with a combination of chemotherapy agents, notably proteasome inhibitors such as bortezomib and immunomodulatory drugs like lenalidomide. 18 These drugs reduce the production of monoclonal light chains, thereby preventing further amyloid deposition. High-dose chemotherapy followed by autologous stem cell transplantation has demonstrated significant efficacy in improving survival, particularly in patients with less advanced disease. Moreover, the use of monoclonal antibodies such as daratumumab, which target specific components of amyloid fibrils, offers a promising therapeutic strategy to treat AL amyloidosis by directly interfering with amyloidogenesis and potentially reducing the amyloid burden in affected organs.
The prognosis of AL amyloidosis is closely linked to the extent of organ involvement, 19 particularly in the heart and kidneys; patients with severe cardiac or renal dysfunction have a significantly worse prognosis. However, advances in diagnostic techniques, including the use of biomarkers and imaging modalities, along with novel therapeutic agents, have improved survival rates, particularly in patients diagnosed at earlier stages. Early diagnosis and prompt intervention remain key factors in improving prognosis and preventing irreversible organ damage. The development of targeted therapies and the refinement of treatment protocols have allowed for more effective management, which can significantly enhance quality of life and survival for patients with AL amyloidosis. 20
Conclusion
AL amyloidosis is a complex and multisystem disorder with profound implications for patient health. Patients will present with non-specific symptoms, therefore, this case emphasizes that early and thorough workup, through the use of advanced biomarkers, imaging, and histological techniques, is crucial for improving outcomes. Our index of suspicion should always remain high as well. The management of AL amyloidosis involves a comprehensive approach that targets both the underlying plasma cell dyscrasia and the systemic effects of amyloid deposition. With continued advancements in therapeutic strategies, particularly through the use of novel agents and personalized treatment regimens, the prognosis for patients with AL amyloidosis is steadily improving . Nonetheless, timely intervention remains critical in ensuring the best possible outcomes for affected individuals.
Footnotes
Acknowledgements
We would like to thank Dr. Abdul Fattah El Kheir (Department of Hematology and Oncology, Nini Hospital) for his expertise in diagnosing and contributing to the management of amyloidosis.
Consent to Participate
A written informed consent was signed by the patient before submitting the manuscript.
Author Contributions
Tya Youssef, MD: Data collection, data analysis, clinical management of the patient, writing of the original draft, literature review, and manuscript review. Karim Zodeh, MD: Data analysis, writing of the original draft, and manuscript review. Karim Hoyek, MD student: Clinical management of the patient, manuscript editing. Anthony Bedran, MD student: Clinical management of the patient, manuscript editing. Anthony Bayeh, MD: Data analysis, literature review, manuscript revision, and providing guidance on amyloidosis treatment protocols. Philippe Attieh, MD: Literature review, manuscript revision. Karam Karam, MD: Supervision, manuscript review, and critical analysis of data. Mahmoud Othman, MD: Data curation, manuscript writing and editing, revision of the manuscript after peer review, submission and handling of correspondence with the journal, and final approval of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.