
Abstract
Introduction:
Workplace-related traumatic lip injuries, particularly at the vermilion-cutaneous junction, are challenging due to functional impairment and visible scarring. While typically managed in specialized settings, some cases present in primary care clinics. This report details the successful management of a penetrating laceration at this junction using layered closure and MEBO for optimized healing, with postoperative scar massage therapy to enhance recovery.
Case presentation:
A 19-year-old male construction worker sustained a full-thickness laceration from the vermilion-cutaneous junction to the inner mucosa. The injury was repaired in a primary care clinic, where precise vermilion alignment was essential. Layered closure was performed using absorbable (5-0 Vicryl) sutures for mucosal, muscular, and dermal layers, and nonabsorbable (6-0 Prolene) sutures for the vermilion-cutaneous junction. MEBO, a plant-based ointment primarily used for burns, was applied postoperatively to promote healing, and reduce scarring. Scar massage therapy was initiated after wound healing. Follow-ups at 5 days, 1 week, 6 weeks, and 4 months showed excellent cosmetic outcomes, minimal scarring, and full functional recovery.
Clinical discussion:
6-0 Prolene was preferred over nylon sutures due to its superior biocompatibility. Simple interrupted sutures ensured tension-free closure for optimal healing. MEBO supported epithelial proliferation, moisture retention, and reduced inflammation—promoting faster tissue repair and superior scar remodeling compared to standard antibiotic ointments, petroleum jelly, or silicone gels. Postoperative scar massage further enhanced collagen remodeling, reduced fibrosis, and improved lip flexibility.
Conclusion:
This case highlights the feasibility of managing complex lip injuries in a primary care setting and emphasizes the importance of precise anatomical repair, proper suture selection, and novel interventions like MEBO and scar massage. Further research is needed to establish MEBO’s role in standard postoperative care for traumatic lip injuries.
Keywords
Introduction
Lip injuries are a common occurrence in both adults and children, often resulting from accidents, falls, or physical altercations in various settings such as the home, workplace, or school.1,2 These injuries are generally classified into 2 categories: lacerations and avulsions. Lacerations can often be managed in the emergency department, while more extensive avulsions may necessitate surgical intervention. 1 Among these, injuries involving the vermilion–cutaneous junction—the boundary between the mucosal tissue of the lip and the skin—pose distinct functional and esthetic challenges. This critical anatomical landmark plays a key role in facial expression, speech, and eating. Injury to this region and subsequent improper healing can lead to complications such as functional difficulties and cosmetic concerns, including scarring, asymmetry, or notching of the lip contour.3,4 The complexity of the vermilion–cutaneous junction stems from its dense vasculature, nerve supply, and the underlying orbicularis oris muscle. As a result, effective surgical repair demands precision in suture selection, tension control, and postoperative care to minimize long-term complications and optimize both functional and cosmetic outcomes.2-9
Historically, lip laceration repair focused on simple wound closure techniques. Over time, advances in surgical methods established layered closure as the preferred approach to restore both function and esthetics, with careful suture selection playing a critical role in optimal healing.1-3 Currently, the gold standard for repairing deep lip lacerations involves layered closure using absorbable sutures for deeper tissues and fine, nonabsorbable sutures (eg, 6-0 polypropylene or nylon) for the vermilion border, ensuring precise alignment and minimal scarring.2-6
Postoperative topical treatments such as antibiotic ointments, petroleum jelly, or silicone gels have traditionally been used to prevent infection and support wound healing.2,3,6 However, these conventional options often fall short in maintaining an optimal moist wound environment, reducing inflammation, and promoting epithelial regeneration—especially in cosmetically sensitive areas like the lips. MEBO addresses these challenges by accelerating epithelialization, enhancing moisture retention, minimizing scar formation, and demonstrating both safety and improved healing efficiency. 10
While most literature focuses on general guidelines for lip laceration repair,1-9 no studies have explored the use of MEBO for traumatic full-thickness lip lacerations, particularly those sustained in workplace accidents. Given its well-documented efficacy in burn management, its potential role in trauma care remains underexplored. To address this gap, we present a case of a 19-year-old construction worker who sustained a full-thickness upper lip laceration at the vermilion–cutaneous junction due to a workplace accident. The injury was successfully managed in a primary care clinic using meticulous suturing techniques followed by an innovative postoperative approach incorporating MEBO. This case highlights the feasibility of managing such injuries in primary care and underscores the potential of MEBO in promoting functional restoration, superior esthetic outcomes, and effective wound healing.
Case presentation
A 19-year-old Egyptian male construction worker presented to a primary care clinic with a traumatic upper lip injury sustained at his workplace after falling onto a brick. He arrived 50 minutes after the incident. He had no significant medical history, denied smoking or substance use, and had no known drug allergies.
On examination, he had a full-thickness upper lip laceration at the vermilion–cutaneous junction, penetrating from the external vermilion border to the inner mucosal surface (Figure 1). A horizontal 3 cm laceration along the vermilion-cutaneous junction separated the vermilion from the surrounding skin (Figure 1). The wound extended into the oral cavity, with a 1.5 cm intraoral mucosal tear adjacent to the upper left incisors (Figure 2A). There were no broken teeth or gum lesions. Although significant swelling was present, there was no active bleeding or evidence of facial nerve injury.

The initial injury to the upper lip shows a penetrating full-thickness wound, with a 3 cm laceration along the vermilion-cutaneous junction externally, extending to the inner mucosal surface of the lip. Forceps inside the wound highlight the separation of the vermilion from the surrounding skin, spanning the entire thickness of the upper lip. The patient is biting on a gauze pad to support the partially separated lip and control bleeding.

(A) The 1.5 cm mucosal laceration, representing the internal extension of the full-thickness wound from the vermilion-cutaneous junction to the inside of the mouth near the left upper incisors, was sutured first using simple interrupted absorbable sutures and (B) the upper lip after multilayered repair, with superficial suturing at the vermilion-cutaneous junction using simple interrupted non-absorbable sutures.
The patient was informed of the surgical procedure, risks, and potential complications and consented to proceed under local anesthesia. Given the nature of the injury and the patient’s healthy background, surgical repair was planned. The primary goals were to restore vermilion–cutaneous junction alignment and minimize scarring. Tetanus prophylaxis was administered, as the injury was caused by a brick, which could introduce tetanus spores into the wound.
The patient was placed in a comfortable supine position with appropriate sterile draping of the surgical site. A 2% lidocaine solution was used to perform an infraorbital nerve block for local anesthesia, ensuring pain relief during the procedure. Minimal local infiltration was also performed around the wound margin to ensure adequate anesthesia of both mucosal and cutaneous tissues. The wound was cleaned and debrided to remove any foreign debris or contaminated tissue. The closure of the deep laceration at the vermilion-cutaneous junction began with a layered closure technique. First, the mucosal tear was repaired intraorally using simple interrupted sutures with 5-0 polyglactin 910 (Vicryl), an absorbable suture material (Figure 2A). Next, the deeper dermal layer and orbicularis oris muscle were approximated and repaired using the same technique with 5-0 Vicryl sutures. Precise alignment of the vermilion–cutaneous junction was emphasized to prevent contour irregularities. Care was also taken to eliminate dead space to minimize the risk of hematoma formation, contracture, and excessive scarring.
Following this, the vermilion–cutaneous junction between the white zone of skin and the red zone of the lip was meticulously repaired using simple interrupted sutures with 6-0 polypropylene (Prolene), a nonabsorbable suture material (Figure 2B). The repair began at the midline of the upper vermilion border to ensure cupid’s bow integrity, then proceeded laterally. The sutures were placed approximately 5 mm apart to minimize tension on the wound. Special care was taken to preserve the natural alignment of the vermilion–cutaneous junction during skin closure, ensuring an even cosmetic contour despite the challenges of performing such a repair in a primary care clinic. Meticulous technique resulted in an optimal cosmetic outcome.
A thin layer of Moist Exposed Burn Ointment (MEBO) was applied externally and intraorally, followed by sterile dressing. The patient was prescribed a systemic antibiotic, amoxicillin-clavulanic acid (Augmentin) 1 g tablets, 1 tablet every 12 hours for 10 days, and an analgesics of Ibuprofen 400 mg tablets, 1 tablet every 6 to 8 hours as needed. The patient was advised to gently clean the wound with saline and apply a thin layer of MEBO 3 times daily. This approach aims to maintain a moist healing environment, prevent scab formation, facilitate suture removal, and support proper healing. Moreover, to achieve better healing and minimize the risk of scarring, the patient was instructed to refrain from activities that could strain the lip, such as intense facial expressions or smoking. Additionally, the patient was advised to follow a soft diet and avoid straws and spicy foods to prevent irritation to the healing wound, particularly in the initial weeks after surgery.
Follow-up appointments were scheduled at 5 days, 1 week, 6 weeks, and 4 months to monitor wound healing and evaluate both cosmetic and functional recovery. During follow-up visits, the wound was assessed for any signs of dehiscence or infection, and the progression of scar formation was evaluated to ensure that any potential complications were addressed promptly. At the 5-day follow-up, moderate swelling was noted on the left side of the upper lip, which delayed the removal of the nonabsorbable sutures (Figure 3). The swelling showed no signs of redness, heat, or tenderness. We instructed the patient to elevate his head while lying down, using 2 to 3 pillows to reduce blood flow to the area, promote healing, and minimize swelling. The patient was also prescribed an anti-inflammatory drug (Reparil 20 mg) to further reduce the swelling. By the 1-week follow-up, the swelling had subsided, and the wound edges had approximated well, allowing for suture removal (Figure 4). The patient was then instructed to continue applying a thin layer of MEBO to the wound 3 times daily. Scar massage was initiated 1 week after suture removal to promote collagen remodeling and prevent fibrosis. The patient was then instructed to continue the MEBO application and perform gentle circular massage motions for 3 to 5 minutes per session. During the 6-week follow-up visit, only minimal swelling was noted, and the vermilion-cutaneous junction remained well-defined (Figure 5). The patient reported satisfactory cosmetic results with no difficulties in eating or speaking. By the 4-month follow-up, the swelling had completely resolved, and the patient had fully resumed work without any functional impairments in speech or eating. Clinical evaluation confirmed excellent cosmetic and functional outcomes, with well-integrated scar tissue, preserved lip mobility, and no signs of hypertrophic scarring or contracture (Figure 6). The patient expressed high satisfaction with the esthetic outcome and demonstrated remarkable lip mobility.

The upper lip 5 days post-repair, showing moderate swelling.

The upper lip 1-week post-repair, after suture removal, showing mild swelling.
The upper lip 6-week post-repair, showing a significant reduction in swelling, a well-defined vermilion-cutaneous junction, and no noticeable scarring.

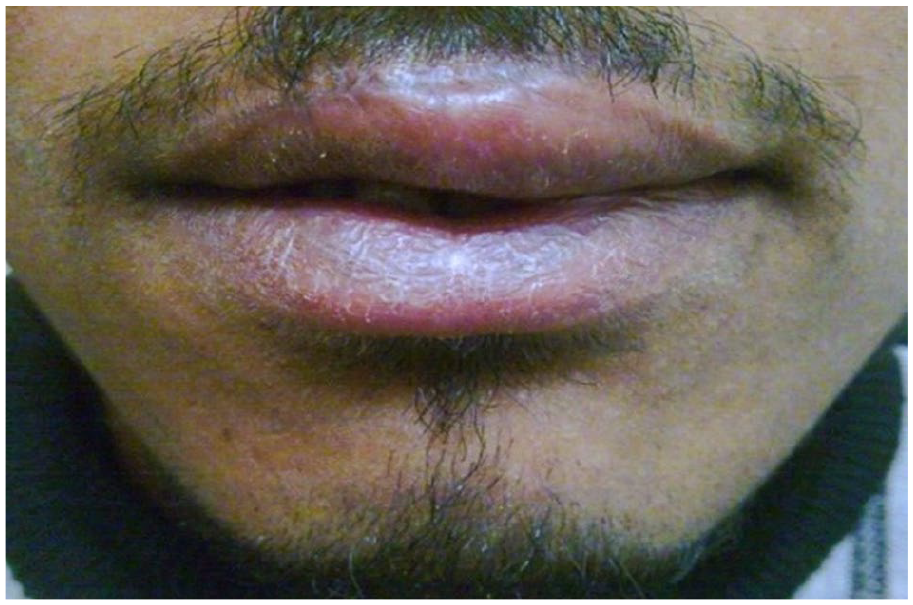
The upper lip at 4 months post-repair, showing good functional and cosmetic outcomes.
Clinical discussion
Lip injuries frequently present in emergency and oral maxillofacial settings,1,11-13 with lacerations involving the vermilion–cutaneous junction presenting unique functional and esthetic challenges.1,3,4,12 Anatomically, the lip consists of 3 layers: skin, muscle, and oral mucosa. Key features include the philtrum (the vertical groove above the upper lip), the commissure (where the upper and lower lips meet), and the vermilion (the border between the lip and surrounding skin). Sensory innervation of the upper lip and overlying skin is provided by the infraorbital nerve (a branch of the maxillary division of the trigeminal nerve), while the lower lip and gingiva are supplied by the mental nerve (a branch of the mandibular division of the trigeminal nerve).2,3,5,8 Given the complex anatomy, meticulous surgical repair—especially of the vermilion–cutaneous junction—is essential. Inadequate timely repair can lead to visible scarring, asymmetry, and functional impairments affecting speech, eating, and facial expression.1-4 Additionally, disruption of the underlying orbicularis oris muscle—essential for lip movement—may lead to lasting functional and cosmetic complications if not properly addressed.2,5-7
This report presents a rare and complex case of a penetrating full-thickness upper lip laceration sustained in a construction-related accident. The injury extended from the external vermilion–cutaneous junction through all layers of the lip into the oral mucosa, necessitating meticulous anatomical restoration. Unlike more common workplace injuries involving the extremities, head, or torso, deep lip trauma in construction settings is rarely documented. 14 Given the wound’s complexity, a layered closure technique was employed to optimize functional and esthetic outcomes. This discussion provides a detailed analysis of a layered closure technique, outlining the suturing procedure, including suture materials and techniques, as well as strategies for wound tension management, along with an innovative postoperative care approach incorporating Moist Exposed Burn Ointment (MEBO) and scar prevention strategies.
Suture materials and suturing techniques
In managing this penetrating full-thickness upper lip injury at the vermilion–cutaneous junction, selecting an appropriate closure technique was critical to achieving optimal functional and esthetic outcomes.15,16 Given the injury’s complexity—extending through all layers of the upper lip—a meticulous, multi-layered closure was necessary to restore anatomical integrity and optimize healing. 17
This approach allowed for separate repair of the mucosa, muscle, and skin, ensuring precise alignment of the vermilion–cutaneous junction, a critical feature for both lip function and appearance. A single-layer closure risked asymmetry, scarring, and disruption of the orbicularis oris muscle, which is essential for speech, eating, and facial expression.1-3,5-9,17-19 Multi-layered closure also ensured better tension distribution, reducing the likelihood of wound dehiscence and contour distortion3,5,6,9,11,18,19 Once this technique was established, the next essential step was selecting the appropriate suture materials and methods to support wound healing and long-term outcomes.
The choice of suture material is pivotal for ensuring that both functional recovery and esthetic restoration are optimized. 15 In this case, absorbable sutures (5-0 Vicryl) were used for the mucosal, muscular and deep dermal layers, whereas nonabsorbable sutures (6-0 Prolene) were selected for the vermilion-cutaneous junction. Absorbable sutures, such as Vicryl, are ideal for mucosal, muscular, and deep dermal layers because of their excellent tissue compatibility and the advantage of not requiring removal which minimizes patient’s discomfort and reduces the risk of infection.1-3,6-9,17-21 On the other hand, the choice between absorbable versus nonabsorbable for skin closure remains unclear. 22 Some studies recommend nonabsorbable sutures,1-3,6-9,18,19 while other studies recommend absorbable sutures for skin closure especially if the patient would not be able to return for suture removal.3,8,21,22 In 1997, Parlin 2 argued that absorbable sutures used for skin closure may dissolve before the wound is fully healed, potentially contributing to wound dehiscence. Additionally, the vermilion border, a high-tension area, requires nonabsorbable sutures due to their superior tensile strength, which offers better support for areas under increased tension, such as the upper lip. In contrast, in 2016, Xu et al 22 conducted a meta-analysis of 1748 patients across 19 randomized controlled trials, finding no significant differences between absorbable and nonabsorbable sutures in infection rates, scarring, wound dehiscence, or patient satisfaction. However, subgroup analysis suggested that intradermal absorbable sutures may offer slightly better cosmetic outcomes, though follow-up data were limited. The authors concluded that absorbable sutures are a viable alternative for skin closure but emphasized the need for longer-term studies to confirm esthetic benefits. Similarly, in 2018, Sheik-Ali and Guets 23 reviewed 25 randomized controlled trials involving 5,781 patients and found no significant difference between absorbable and nonabsorbable sutures in infection rates, complications, or the risk of wound dehiscence. The study concluded that absorbable sutures were not superior to nonabsorbable sutures in these outcomes. These findings were further supported by Malhotra et al, 21 who conducted a systematic review and meta-analysis of clinical, esthetic, and patient-reported outcomes comparing absorbable and nonabsorbable sutures for facial skin closure. This review, which included 9 randomized controlled trials with 804 participants, also found no significant differences between the 2 suture types in terms of infection rates, wound dehiscence, scarring, or patient satisfaction. While the findings of Xu et al, Sheik et al, and Malhotra et al suggest that absorbable sutures are a viable alternative for facial wound closure, Parlin’s earlier considerations regarding high-tension areas, such as the vermilion border, may still influence clinical decision-making in specific cases.
The most commonly used nonabsorbable sutures for skin closure are Prolene and nylon.15,21 Some studies recommend Prolene for skin and vermilion border closure,3,7 while others indicate that nylon is frequently used for skin closure.2,7,17,18,20 Both Prolene and nylon are widely used in lip repair, but their distinct properties influence suture selection. For the vermilion-cutaneous junction in our case, we selected 6-0 Prolene nonabsorbable sutures over nylon due to its superior tensile strength, flexibility, and minimal tissue reactivity.24,37 Prolene’s monofilament structure reduces bacterial adhesion, lowering the risk of postoperative infection. 24 Additionally, its smooth surface minimizes friction, helping to reduce scar formation and the risk of granuloma—a crucial factor in high-visibility areas such as the lip.3,24 Similarly, nylon, available in monofilament or braided forms, also exhibits low bacterial adhesion and good tensile strength. 19
In 1992, Moy et al 15 reviewed the characteristics of an ideal suture, emphasizing strength, ease of handling, secure knot formation, minimal tissue inflammation, and resistance to infection. The review also highlighted the importance of a suture’s ability to accommodate wound edema through slight elasticity, though no single suture type possesses all these properties. Thus, selecting the appropriate suture is essential for optimizing surgical outcomes in skin closure. Multiple studies have compared the characteristics of nylon and Prolene to guide optimal suture selection. In 2022, a systematic review by Faris et al 20 evaluated commonly used suture materials in oral surgery, with a focus on their inflammatory response, bacterial adhesion, and physical properties during oral wound closure. Among the materials studied, nylon stood out for its lower bacterial accumulation, good tensile strength, and ease of handling with secure knot formation. These properties make nylon a reliable choice for oral wound closure, particularly in minimizing infection risk and ensuring strong wound edges approximation. Similarly, in 2016, Selvi et al 24 evaluated the histopathological effects of 4 commonly used suture materials in oral surgery, including Prolene. Tissue healing was assessed based on cell density, necrosis, fibrosis, foreign body reaction, and signs of acute or chronic infection. The study found that Prolene induced the least tissue reaction among the materials tested, making it the preferred choice for high-tension areas such as the lip and vermilion border, where long-term support and minimal scarring are critical. Furthermore, in 1993, Chen et al, 25 compared 10-0 Prolene and 10-0 nylon monofilament sutures in microsurgical anastomosis procedures. The study concluded that while both suture types achieved favorable outcomes, Prolene outperformed nylon in handling, knot security, and biocompatibility, leading to fewer complications and shorter operative times. Additionally, in 2012, Fowler et al 26 investigated bacterial adherence in various suture materials using a methicillin-resistant Staphylococcus aureus (MRSA)-contaminated wound model. Their findings demonstrated that monofilament sutures exhibited significantly lower bacterial adherence than braided sutures. While nylon is typically monofilament, certain variations exist in braided form, which may influence its bacterial adhesion properties. In contrast, Prolene, a standard monofilament suture, may offer superior resistance to bacterial accumulation. Collectively, these studies highlight Prolene’s advantages over nylon, particularly in minimizing bacterial adhesion, reducing tissue reactivity, and providing superior handling in high-tension areas. These properties make Prolene a preferred choice for precise wound closure in cosmetically and functionally sensitive regions such as the lip.
While selecting the appropriate suture material is essential, the success of wound closure also depends on the suturing technique employed. Effective suturing methods play a critical role in achieving optimal cosmetic outcomes and preventing scarring or delayed wound healing. 15 In our case, we employed the simple interrupted suturing technique using 5-0 Vicryl absorbable sutures for the mucosal, muscular and deep dermal layers, and 6-0 Prolene for the vermilion-cutaneous junction.
The simple interrupted suture remains the gold standard for wound closure due to its precise wound edge approximation, reduced risk of dehiscence, and adaptability to high-tension areas. 17 Several studies support its use for both deep dermal layers and the vermilion–cutaneous junction.1-3,6-9,17-19 However, alternative techniques have been explored to optimize wound stability and cosmetic outcomes.
Some studies have suggested that horizontal mattress sutures may be beneficial in high-tension areas, and recommended this technique for deep dermal closure due to its ability to evert wound edges and reduce tension.1,19,27 In 2017, Acar et al 27 conducted a randomized split-mouth study involving 30 patients to compare horizontal mattress and simple interrupted sutures in oral and dental surgery. The results showed no significant differences in postoperative pain or swelling, but horizontal mattress sutures were associated with significantly lower rates of wound dehiscence, suggesting greater wound stability in select cases.
Another widely studied approach is subcuticular and intradermal suturing, which has been proposed for skin closure and scar minimization.2,22,28,29 In 2010, Onah et al 28 compared subcuticular versus nonabsorbable interrupted sutures in 117 patients undergoing cleft lip repair and found that subcuticular sutures resulted in shorter hospital stays while maintaining similar complication rates. Similarly, in 2014, Shin and Bordeaux 29 reviewed 24 studies—including 17 randomized controlled trials—and found that subcuticular sutures provided better esthetic outcomes than simple interrupted sutures, especially for trunk and extremity repairs. However, 9 of the 17 trials found no significant differences between techniques, highlighting the role of individual case considerations in technique selection. Further supporting the advantages of subcuticular closure, a more recent systematic review and meta-analysis by Luo et al, 30 analyzing 10 randomized controlled trials with 1181 participants, found that continuous sutures (subcuticular and transdermal) resulted in superior cosmetic outcomes compared to interrupted sutures. Patients and physicians reported higher visual analog scale (VAS) scores for cosmetic appearance, and continuous sutures were associated with lower wound dehiscence rates, although infection rates were comparable. These findings suggest that beyond cosmetic benefits, subcuticular closure may also shorten hospitalization, reduce anesthesia use, and lower costs, making it a viable alternative to traditional skin sutures in appropriate cases.
While certain techniques offer specific advantages, no single suturing method is universally superior. 31 In 1991, Moy et al emphasized that technique selection should be based on wound-specific factors such as tension, location, and the need for eversion. Mattress sutures provide better eversion and dead-space closure, whereas interrupted sutures ensure precise wound approximation but are more time-consuming. Subcuticular sutures minimize visible suture marks, making them particularly beneficial in cosmetically sensitive areas. Taken together, these findings highlight the need for a tailored suturing approach that balances wound tension, stability, and esthetic outcomes. While the simple interrupted technique remains the gold standard, alternative methods such as horizontal mattress and subcuticular sutures may offer advantages in specific clinical scenarios. Therefore, careful technique selection, guided by wound characteristics and patient needs, is crucial for optimizing both functional and cosmetic outcomes.
Wound tension management in lip repair
Beyond suturing technique, wound tension management is crucial for optimal healing and cosmetic outcomes. Excessive tension can impair circulation, delay healing, and increase the risk of ischemia, necrosis, dehiscence, and hypertrophic scarring.2,3,6,7,9,32 To prevent these complications, tension management techniques focus on minimizing strain on the wound edges, while maintaining healthy blood flow.3,7,8,18,32-35 Poor circulation not only impairs the delivery of oxygen and nutrients to the wound site, but also reduces immune cell recruitment—particularly neutrophils and macrophages—hindering the inflammatory and remodeling phases of healing, increasing the risk of infection, fibrosis, and poor scar formation.3,18,32,33,35 Therefore, optimizing wound tension is critical for both functional recovery and esthetic outcomes, particularly in high-mobility areas such as the lip.18,32 In our case of upper lip closure, multiple steps were taken to achieve this.
Wound preparation
Proper wound preparation is essential for even tension distribution and to minimize the risk of dehiscence. We thoroughly cleaned the wound and surrounding tissues to eliminate debris, as contaminated wounds are more prone to breakdown.2,3,18 This aligns with findings from Khan et al, 36 who conducted a randomized controlled trial in 2019 comparing continuous and interrupted mass closure techniques in pediatric transverse incisions. Among 350 patients aged 0 to 12 years undergoing emergency or elective surgery, no statistically significant difference in wound dehiscence was observed between the 2 methods. However, the study emphasized that dirty wounds had a higher risk of dehiscence regardless of suture type, reinforcing the critical role of preoperative wound preparation in preventing complications.
Suture selection for tension control
To balance wound stability and circulation, we used 5-0 Vicryl absorbable sutures for the mucosal, muscular, and deep dermal layers and 6-0 Prolene nonabsorbable sutures for the vermilion-cutaneous junction closure. This approach ensured secure approximation without excessive tension, reducing the risk of dehiscence and compromised healing. 35 Selecting the right suture material is essential for both functional recovery and optimal cosmetic outcomes in lip repair.
Suturing technique for tension control
To ensure even tension distribution and optimal wound healing, we employed simple interrupted sutures for both deep and cutaneous layers. This technique allows for controlled, adjustable tension at each stitch, reducing the risk of vascular compromise and promoting healthy blood circulation.37,38
Alternative techniques, such as horizontal mattress sutures, can help redistribute tension and evert wound edges, particularly in larger wounds or flaps. 39 However, they pose a higher risk of dermal plexus strangulation, which may impair cutaneous blood flow.33,39 In 2020, Marsidi et al 33 compared 5 suturing techniques using a standardized wound tension model and found that simple interrupted sutures required less force to approximate wound edges than horizontal mattress sutures. They concluded that the higher tension of horizontal mattress sutures may impair healing by compromising perfusion at wound margins. In contrast, subcuticular sutures, commonly used for tension-free skin closure, minimize strain on wound edges.15,30 However, in 2023, Azmat 37 found that simple interrupted sutures are more effective in preserving cutaneous microcirculation. Compared to mattress or subcuticular sutures they provide superior skin approximation, exert less tension on the wound, and pose a lower risk of vascular compromise. Given these factors, simple interrupted sutures remain the preferred technique for achieving optimal stability, circulation, and cosmetic outcomes in lip repair.
Layered closure for even tension distribution
To ensure even tension distribution and minimize strain on the epidermis, we employed a layered closure technique, suturing from the deep layers to the superficial skin layers. This method not only optimized wound healing but also preserved the vermilion–cutaneous junction and maintained a tension-free surface closure.3,7,8,17,18,32
To further reduce mechanical stress, we spaced sutures 5 mm apart, a strategy known to enhance blood flow, minimize tension on healing tissue, and prevent excessive scarring.16,40 This approach is particularly important in lip closure, where high mobility and the need for precise vermilion border alignment demand an even tension distribution to minimize the risk of hypertrophic scarring or wound dehiscence.
Recent research provides valuable insights into the impact of suture spacing on wound healing and scar esthetics, guiding best practices for optimal closure. In 2019, Stoecker et al 41 evaluated the effect of suture spacing on wound healing and scar esthetics by comparing high-density (5 mm) and low-density (10 mm) sutures. Their study found no significant differences in complications between the two techniques. However, at 3 months, scars from the 10 mm spacing appeared more esthetically favorable, though by 6 months, there was no noticeable difference. This suggests that while 5 mm spacing is effective, a 10 mm spacing may be a viable and more efficient alternative without compromising long-term outcomes. More recently, Pazyar et al 40 investigated the impact of 2-mm versus 5-mm suture spacing on the esthetic and functional outcomes of skin closures across age groups, assessing healing at 1 and 3 months using the Observer Scar Assessment Scale (POSAS). Younger patients (<50 years) showed better outcomes regardless of spacing. While 5 mm spacing was initially preferred by both patients and observers at 1 month, differences diminished by 3 months. These findings are consistent with prior research suggesting that moderately wider spacing (eg, 5 mm) supports efficient closure, short-term esthetic benefits, and reduced suture use. Given the lip’s high mobility and cosmetic importance, our use of 5 mm spacing reflects these principles. Additionally, our 19-year-old patient falls within the age group associated with optimal outcomes, further supporting this choice as a balance between efficiency, cosmetic outcomes, and functional healing.
Additionally, we employed a midline-to-lateral suturing approach, beginning at the vermilion–cutaneous junction and extending laterally. This technique allowed for precise alignment of vermilion–cutaneous junction, ensuring the preservation of the philtrum and Cupid’s bow.42,43
Gentle tissue handling to preserve circulation
Gentle tissue handling during suturing was crucial to preventing additional trauma that could compromise circulation and lead to necrosis. By carefully manipulating the tissues, we maintained vascular integrity, minimized excessive tension, and preserved blood flow, all of which are essential for optimal healing. 17
Thus, effective wound tension management is essential for ensuring a stable closure, minimizing complications, and optimizing both functional and esthetic outcomes in lip repair. By integrating proper suture selection, layered closure, and careful tissue handling, we maintained balanced tension and facilitated efficient healing. Once the wound was securely closed, postoperative care and follow-up became critical in preserving long-term tissue integrity and preventing complications.
Postoperative care with novel use of Moist Exposed Burn Ointment (MEBO) and scar prevention measures
While precise tension management during suturing is essential, optimal healing requires comprehensive postoperative care. This phase is crucial in preventing complications such as infection, excessive scarring, and suboptimal functional or esthetic outcomes.2,3,7-9 In our case, we implemented a moist wound healing protocol using normal saline and MEBO—a less commonly reported approach in traumatic lip injuries. MEBO has been shown to create an optimal moist environment that enhances keratinocyte migration, angiogenesis, and interaction with growth factors, facilitating tissue healing and reducing excessive scarring.10,44-50
Standard postoperative care typically involves wound cleansing with warm water or normal saline, along with topical antibiotics to reduce infection risk, prevent crusting, and ease suture removal.2,3,7 Other studies support the use of petroleum jelly (Vaseline) for its occlusive properties, which helps reduce trans-epidermal water loss, maintain moisture, and prevent scabbing. 51 Additionally, silicone-based therapies—such as silicone gel sheets and ointments—are widely recommended in the later stages of wound healing to enhance hydration, minimize fibrosis, and improve cosmetic outcomes.8,51 While these conventional approaches—topical antibiotics for infection control, petroleum jelly for moisture retention, and silicone therapies for scar management—each target a specific aspect of wound healing, MEBO provides a more comprehensive solution by simultaneously promoting tissue regeneration, reducing infection, maintaining hydration, and minimizing scarring.
Moist Exposed Burn Ointment (MEBO; Julphar, United Arab Emirates), is an oil-based ointment that was introduced in China over 2 decades ago and is now widely used for burn wound care across Asia and the Middle East.52,53 It contains sesame oil, beta-sitosterol, berberine, beeswax, and plant extracts, providing anti-inflammatory, antimicrobial, and regenerative benefits. Beta-sitosterol, the primary active ingredient, is known for its strong anti-inflammatory effects, while berberine provides antimicrobial benefits.52,54 Additionally, MEBO’s hyperosmolar properties help prevent bacterial proliferation, reduce toxicity of pathogens, and enhance immune response. 48 Studies report that MEBO accelerates wound healing, reduces pain, minimizes bacterial load, and decreases reliance on antibiotics and analgesics, all while promoting esthetically superior healing outcomes.10,44-46,55 Given these advantages, MEBO presents a promising alternative for postoperative wound management, particularly in cases requiring optimized healing and scar prevention.
In 2000, Al-Numairy 10 evaluated MEBO for open wounds across various surgical conditions, including burns, pressure sores, diabetic ulcers, and surgical wounds. The study highlighted MEBO’s cost-effectiveness, simplicity, safety, and consistent functional and esthetic outcomes. Similarly, in 2002, Atiyeh et al 45 assessed MEBO’s efficacy in treating cutaneous wounds and ulcers, reporting a rapid reduction in ulcer size while maintaining a clean wound environment. Importantly, MEBO did not promote antibiotic-resistant bacterial strains—an increasingly critical factor in wound management.
Comparative studies have also evaluated MEBO against topical antibiotics in wound healing and infection prevention. In 2000, Ang et al 56 compared MEBO and silver sulphadiazine in 115 patients with partial-thickness facial burns, randomly assigning them to either treatment and monitoring their progress until the wounds reduced by 75%. The study found that both treatments effectively promoted healing and prevented infection, with comparable clinical and histological outcomes. Similarly, in 2009, Jewo et al 57 compared the wound-healing effects MEBO and silver sulphadiazine in a rat model. Ten Sprague Dawley rats were divided into 2 groups, receiving either MEBO or silver sulphadiazine. Both treatments provided comparable infection protection and facilitated healing, with advanced wound recovery observed by day 8. Histological analysis further confirmed similar healing processes, leading the authors to conclude that MEBO is a viable alternative to silver sulphadiazine for partial thickness burn wounds.
However, MEBO offers distinct advantages over conventional topical antibiotics. It allows for easier dressing changes, clearer assessment of healing due to minimal sloughing, and fewer adverse effects. These benefits make MEBO a convenient alternative, particularly for facial wounds or cases where a more natural, less chemical-intensive treatment is preferred.56,57
Beyond its advantages over topical antibiotics, MEBO has also been compared to petroleum jelly, another widely used moist healing agent. While both create a protective barrier to maintain hydration and support healing, their mechanisms of action and therapeutic benefits differ significantly. MEBO is an active healing ointment containing herbal extracts, primarily beta-sitosterol, along with sesame oil and beeswax. Its antibacterial and anti-inflammatory properties make it effective for burns, ulcers, and deeper wounds.52,53 Unlike petroleum jelly, MEBO is partially absorbed into the skin, actively promoting epithelial regeneration and accelerating wound healing.44,45,49,50 In contrast, petroleum jelly is a passive healing agent composed entirely of petroleum-derived hydrocarbons. It forms an occlusive layer that locks in moisture but does not directly contribute to cellular activity during wound healing.51,58 While effective for minor cuts, scrapes, and chapped skin, petroleum jelly lacks antibacterial properties unless combined with other ingredients. 59
Comparative studies on MEBO demonstrate that it is more than just a moisture-retaining ointment—it actively promotes wound healing, tissue regeneration, and infection control, making it a valuable alternative to other moist healing therapies. In 2003, Atiyeh et al 46 compared MEBO to occlusive dressings like Tegaderm for partial thickness wound healing, evaluating healing time, trans-epidermal water loss (TEWL), moisture retention, and scar quality. Their findings showed that MEBO promoted faster healing and earlier restoration of the physiological barrier, as indicated by significantly lower TEWL measurements. Additionally, MEBO-treated wounds exhibited better scar quality, linking improved functional healing to superior cosmetic outcomes. The study also highlighted that MEBO is easier to apply than occlusive dressings, making it a practical choice for large wounds and burns. The findings suggest that MEBO’s benefits extend beyond passive moisture retention, potentially contributing to enhanced wound healing and tissue regeneration. More recently, Gong et al 49 investigated MEBO’s role in diabetes-related wound healing. Using a diabetic mouse model and in vitro studies, the researchers found that MEBO accelerated healing by promoting granulation tissue formation, collagen remodeling, and re-epithelialization. The study also observed increased expression of key epidermal regeneration markers, including Ki67 (a proliferation marker), cytokeratin 10 (CK10), and cytokeratin 14 (CK14), supporting the notion that MEBO enhances cellular recovery at the molecular level.
In contrast, in 2016, Czarnowicki et al 60 challenged the classification of petrolatum (petroleum jelly) as an ‘inert’ moisturizer, investigating its effects on skin barrier repair and antimicrobial responses. Their study on healthy individuals and atopic dermatitis patients found that petrolatum upregulated antimicrobial peptides, including S100A8, S100A9, and β-defensin 2, as well as innate immune genes such as interleukin-6 (IL-6), interleukin-8 (IL-8), and interleukin-1 beta (IL-1B), thereby enhancing the skin’s defense mechanisms. Additionally, petrolatum promoted epidermal differentiation, increased the expression of filaggrin and loricrin, and thickened the stratum corneum, ultimately strengthening the skin barrier. However, it does not actively promote wound healing at the cellular level.
Beyond their differing effects on wound healing, another critical distinction is their suitability for infected wounds. MEBO’s antimicrobial and anti-inflammatory properties make it suitable for mildly infected wounds.45,56,57 In contrast, petroleum jelly should not be applied to infected wounds unless combined with an antibiotic, as its occlusive nature may trap bacteria and increase infection risk.59,61
MEBO also demonstrates superiority in scar prevention due to its regenerative components and ability to regulate collagen remodeling.46-49,62 By contrast, petroleum jelly primarily functions as a hydration agent and does not actively influence collagen deposition, making it less effective in preventing hypertrophic scars and keloids.58,59 However, petroleum jelly’s affordability and accessibility contribute to its widespread use in postoperative wound care.59,63
Both MEBO and petroleum jelly are well-tolerated but differ in allergic potential. MEBO may pose a higher risk of allergic reactions due to its plant-based composition, particularly its sesame oil content. While sesame allergies were once considered rare, recent studies indicate a rising prevalence of IgE-mediated reactions. 64 However, documented cases of allergic reactions induced by MEBO are exceedingly rare in the literature. Studies have noted that allergic reactions to MEBO are uncommon.10,50,53,62 Notably, MEBO, with its natural plant-based ingredients such as sesame oil, has been found to be non-toxic and non-irritating to the oral mucosa, making it safe for oral use and accidental ingestion.10,50,65,66 In contrast, petroleum jelly consists entirely of purified petroleum-derived hydrocarbons, which are inert, hypoallergenic, and widely tolerated.60,61 However, rare complications have been reported, including cases of exogenous lipoid pneumonia from accidental aspiration.67,68 Although no direct comparative studies exist, MEBO’s bioactive components promote tissue regeneration, while petroleum jelly functions primarily as an occlusive barrier, maintaining hydration but not actively accelerating healing or scar prevention.
The regenerative potential of MEBO is further supported by clinical studies demonstrating its effectiveness in scar prevention and management.47,62,69 In 2003, Atiyeh et al 47 reported in 3 consecutive clinical studies that MEBO provided a prophylactic effect on both primary and secondary wound healing, resulting in superior scar quality. Similarly, in 2016, Majeed 62 evaluated the therapeutic effect of MEBO in preventing and treating post-operative scars in 90 patients undergoing elective surgery. The ointment was applied 3 times daily after suture removal, while the control group used warm saline. Scar quality was assessed over 120 days based on itching relief, skin texture, dystrophy, and color. MEBO was highly effective in 75% of patients, significantly improving scar appearance and cosmetic acceptability. The study concluded that early and consistent use of MEBO can prevent scar proliferation and disturbances, supporting its role in post-surgical scar management. More recently, Liu et al 69 evaluated MEBO in post-laser wound management, comparing it to chlortetracycline hydrochloride ointment in patients with immature, red hypertrophic scars treated with pulsed dye laser and fractional CO2 laser. MEBO-treated patients experienced less pain within the first 3 days and faster wound healing than the control group. After 3 months, they showed improved scar outcomes, including lower Vancouver Scar Scale (VSS) scores and reduced pigmentation. The study concluded that MEBO enhances scar healing, reduces pain, and minimizes pigmentation, making it a beneficial therapy for improving scar outcomes.
In addition to MEBO’s demonstrated efficacy in scar management, silicone-based therapies, particularly silicone gel sheeting, have long been established as effective interventions for hypertrophic scar prevention. While randomized controlled trials have demonstrated the effectiveness of silicone gel sheeting in treating and reducing the incidence of scarring, 70 other studies confirm its role in preventing hypertrophic scars by promoting epidermal hydration, which suppresses fibroblast metabolism and reduces collagen deposition. 71
Comparative research on MEBO and silicone gel for scar prevention is limited. However, in 2021, Basson et al 72 conducted a study comparing MEBO and Kelo-cote silicone-based gel in the treatment of skin scarring, focusing on their transdermal delivery, effects on collagen remodeling, and overall scar maturation. Using Raman Spectroscopy (RS) and High-Performance Liquid Chromatography (HPLC), the researchers confirmed that MEBO’s linoleic acid—derived from sesame oil—penetrated deep into scar tissue, whereas Kelo-cote remained on the surface, forming a protective silicone barrier. MEBO actively modulated collagen structure, shifting the amide I peak (1667-1656 cm⁻¹), indicating collagen remodeling. It also regulated the collagen I/III ratio and reduced elastin levels, promoting controlled scar maturation. In contrast, Kelo-cote did not alter collagen or elastin structure, suggesting a primarily preventative rather than regenerative mechanism. Histological analysis showed a significant increase in mature collagen (Collagen I) in MEBO-treated scars by week 12 (P < .0001), with a corresponding decrease in elastin (P < .05), supporting proper scar formation. Optical Coherence Tomography (OCT) imaging revealed that MEBO initially reduced excessive collagen at week 4 but promoted controlled deposition by week 16 (P < .05), while Kelo-cote had no such effect. The study suggests that MEBO is particularly effective for scars requiring active regeneration—such as burns, surgical wounds, and atrophic scars—due to its deep tissue penetration, delivery of bioactive compounds, and promotion of structured scar maturation. In contrast, Kelo-cote is better suited for preventing hypertrophic scars and keloids by maintaining hydration and limiting excessive collagen deposition. Unlike silicone-based treatments, which primarily act as barriers, MEBO actively modulates scar architecture at the molecular level. A sequential approach using MEBO during the early healing phase followed by Kelo-cote for long-term management may yield optimal scar outcomes.
Age, ethnic, and racial factors significantly influence scar formation.16,73,74 Younger patients—particularly those between 11 and 30 years of age—are more prone to hypertrophic scarring due to increased epidermal turnover and heightened collagen production. 75 Additionally, individuals with darker skin tones (Fitzpatrick skin types IV–VI) are at greater risk of developing hypertrophic scars and keloids, which can also carry psychological burdens. 73 Our patient, a 19-year-old Egyptian male with dark skin (likely Fitzpatrick type IV), falls within this high-risk group. Studies have shown that certain North African populations, including Egyptians, may have a genetic predisposition to abnormal scar formation. 75 These risk factors guided early scar prevention using MEBO.
In our case, follow-up images showed optimal healing, with scars becoming nearly unnoticeable and a well-defined vermilion border and cupid’s bow, yielding highly favorable cosmetic outcomes. These results highlight the importance of consistent postoperative monitoring in optimizing healing. To further enhance scar outcomes, the patient was advised to perform gentle circular scar massage with MEBO for 3 to 5 minutes per session, beginning 1 week after suture removal. Scar massage has been shown to enhance circulation, improve tissue elasticity, and reduce fibrosis, which in turn helps minimize swelling, stiffness, and scarring while preserving or enhancing mobility—outcomes also observed in our patient.76-79 In 2022, Scott et al 78 conducted a scoping review of 25 studies involving 1515 participants, concluding that scar massage improves scar texture and appearance and may enhance mobility by reducing pain and stiffness.
Beyond scar management, effective postoperative care requires regular follow-ups to monitor healing progress, address complications, and optimize outcomes. The importance of scheduled follow-up visits—typically at 5 days, 1 week, 6 weeks, and 4 months—cannot be overstated. As previously discussed, postoperative care involved multiple follow-ups to facilitate timely intervention for complications such as infection, swelling, scarring, or tension-related issues.2,3,6,7,9,34 During follow-ups, careful assessment ensured that the dressing remained intact, maintained appropriate moisture, and minimized mechanical stress on the healing wound.
At the 5-day follow-up, the patient exhibited moderate swelling but showed no signs of infection or dehiscence. Swelling is a common inflammatory response in lip injuries due to the region’s rich blood supply.2,80,81 While it is often concerning, this condition typically resolved with appropriate monitoring and intervention, including a prescription for Reparil 20 mg, an enteric-coated tablet containing amorphous aescin, known to reduce capillary permeability and inhibit edema formation following injury. 80 Notably, this swelling was unlikely to be related to the simple interrupted suturing technique used. In 1979, Speer 38 compared interrupted sutures to other techniques in pig skin wounds and found that interrupted sutures provided 30% to 50% greater tensile strength, reduced edema, and improved microcirculation at the wound margins. These findings suggest that interrupted sutures may offer significant advantages, particularly in cases where early mechanical stress on the wound is expected or when healing capacity is compromised. Thus, the moderate swelling did not indicate a flaw in the chosen technique but rather underscored the importance of vigilant postoperative monitoring. To mitigate potential complications such as wound dehiscence or infection, suture removal was delayed by 2 days—a decision supported by multiple studies.82-84 This phase of follow-up also facilitated dressing adjustments to maintain optimal moisture balance while preventing excessive wound tension. MEBO was applied to sustain a moist healing environment, prevent infection, reduce scabbing, and minimize scar formation. Regular monitoring allowed for the early detection of ischemic or necrotic changes, such as increased redness, swelling, or temperature fluctuations, enabling timely intervention to prevent further tissue damage and optimize healing. It is well-established that proper postoperative care—particularly strategies aimed at reducing wound tension—has been shown to enhance healing outcomes and minimize scarring.34,85
Despite the successful restoration of form and function, important considerations remain. Early swelling delayed suture removal, emphasizing the need for close monitoring, as timely removal helps minimize scarring. 17 Although no long-term complications occurred, such lip injuries can cause permanent scarring or subtle contour changes that may restrict mobility and affect speech or expression.1,2,4,5 The psychological impact of visible scars, especially on the lips—a key feature of identity and social interaction—is significant, 6 particularly for younger patients like ours. This case highlights the necessity of timely, well-managed intervention and consistent follow-up to address potential complications promptly.
In summary, layered closure was chosen to preserve lip anatomy and function while optimizing esthetic outcomes. Combined with tension management and MEBO-based postoperative care, this approach supported effective healing and minimized long-term scarring. Though MEBO is primarily used in burn care, its success in this traumatic lip injury highlights its potential as an adjunctive treatment. Its regenerative, antimicrobial, and scar-modulating properties warrant broader consideration in surgical wound care. Further research is needed to explore its molecular mechanisms—specifically its effects on growth factors, extracellular matrix components, signaling pathways, and gene expression related to fibroblast activation—particularly in chronic wound management, scar modulation, and regenerative medicine. Finally, this case demonstrates that with proper technique and follow-up, complex lip injuries can be effectively managed in primary care, expanding access to high-quality care beyond specialized settings.
Conclusion
This report presents a complex case of a full-thickness penetrating upper lip injury at the vermilion–cutaneous junction following a construction workplace accident. Despite the cosmetic and functional significance of this region, successful repair was achieved in a primary care clinic using a layered closure with simple interrupted sutures, ensuring precise anatomical alignment and tension-free healing.
Postoperative management was key to optimizing outcomes. MEBO application and scar massage supported healing and minimized scarring, resulting in excellent functional and esthetic recovery. Tailoring care to patient-specific factors, such as age and skin type, was crucial in preventing adverse scarring. This case highlights that complex lip and facial injuries can be effectively managed in primary care with proper skills and advanced wound care. Expanding training in these techniques can enhance timely access to quality care, especially in resource-limited settings without immediate specialist availability.
The patient successfully regained both form and function, returning to work and social activities without psychological distress. While long-term follow-up remains essential, further well-controlled studies are needed to establish MEBO’s efficacy and its potential role in standard postoperative care for traumatic lip and facial wounds.
Footnotes
Acknowledgements
I would like to thank Dr. Ahmad N. Abdel-Fattah for his assistance with manuscript editing and proofreading.
Ethical Considerations
The ethical committee approval was not required given the article type (case report).
Consent for Publication
The patient himself provided written informed consent for the publication of his clinical details and/or images. A copy of the consent form is available for review by the editor of this journal.
Author Contributions
Hana Abualadas: Performed the surgical repair and postoperative care, and was involved in writing, reviewing, and editing the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data are included in the manuscript.