
Abstract
This case report presents a rare instance of chronic rib osteomyelitis in a 23-year-old female from Darchula, an underserved rural area in Nepal. Rib osteomyelitis is uncommon and often diagnosed late due to its subtle presentation. The patient initially presented at a primary care center with a 2-week history of a protruding bony mass in the right upper back, accompanied by foul-smelling discharge and low-grade fever. She was referred to a tertiary hospital, where a CT scan, surgical excision, and biopsy confirmed chronic rib osteomyelitis. This case highlights the diagnostic challenges of rare conditions in rural settings and emphasizes the essential role of community-based healthcare in early identification and referral. It underscores the need for accessible diagnostic facilities, community health education, and a multidisciplinary approach to support patients in resource-limited environments.
Introduction
Osteomyelitis is an inflammatory condition of bone due to infection from various microorganisms. 1 This condition commonly follows trauma, bone surgery, or vascular insufficiency. 2 Osteomyelitis can be acute, which presents with rapid symptom onset over days, or chronic, which often takes months to years of prolonged infection. 1 Acute osteomyelitis can be either suppurative or non-suppurative. 2 Chronic osteomyelitis is particularly marked by persistent low-grade inflammation, necrotic bone (sequestrum), new bone formation, and fistulous tracts, which frequently necessitate surgical debridement and long-term antibiotic therapy.2,3
Rib osteomyelitis, however, is an exceptionally rare form, with diagnosis frequently delayed due to nonspecific symptoms and limited awareness. The rarity of rib involvement underscores the need for increased vigilance among healthcare providers, especially in rural and resource-limited settings where access to diagnostic facilities may be limited.
Case Report
A 23-year-old female from Darchula, a rural district in Nepal, presented to our primary healthcare center with complaints of a bony protrusion on her right upper back with a dirty, thick, purulent, foul-smelling discharge, persisting for 2 weeks. She reported a low-grade fever on/off since 1 month but denied any history of trauma, pain, or significant family history. Notably, she had a history of a right-sided subcutaneous anterior chest wall abscess 2 years prior, which had been managed conservatively with oral antibiotics and local wound care, without surgical drainage. There was no comorbidity or immune-deficiency states.
Upon examination at the primary center, the patient appeared conscious and in good general condition, with no pallor, icterus, lymphadenopathy, cyanosis, clubbing, or edema. Her vital signs were within normal limits. Physical examination revealed a bony protrusion in the right upper back region, corresponding to the sixth and seventh ribs, covered with purulent discharge. (Figure 1) On palpation, the protrusion was found to be a detached bony segment approximately 3 × 2 cm in size (Figure 2). No other musculoskeletal abnormalities were detected.

Mass from the right upper back region on first inspection.

Piece of bone detached from the swelling with purulent discharge.
Basic laboratory workup at the primary center indicated an elevated white blood cell (WBC) count of 14 000 cells/cumm (normal range: 4500-11 000 cells/cumm) and a C-reactive protein (CRP) level of 19.49 mg/dl (normal range: 0.8-1 mg/dl), suggestive of an inflammatory process. Given the findings and concerns about a possible bone infection, the patient was referred to a tertiary care hospital for further imaging and specialized assessment.
Diagnostic Assessment and Interpretation at Tertiary Center
At the tertiary care hospital, a computed tomography (CT) scan was performed, which revealed destruction of the postero-lateral portion of the right seventh rib with an elongated bony structure measuring 3.2 × 1.3 cm protruding from the skin surface, consistent with a sequestrum (Figure 3). Under local anesthesia, the sequestrum was excised and sent for histopathological examination, which confirmed the diagnosis of chronic rib osteomyelitis.
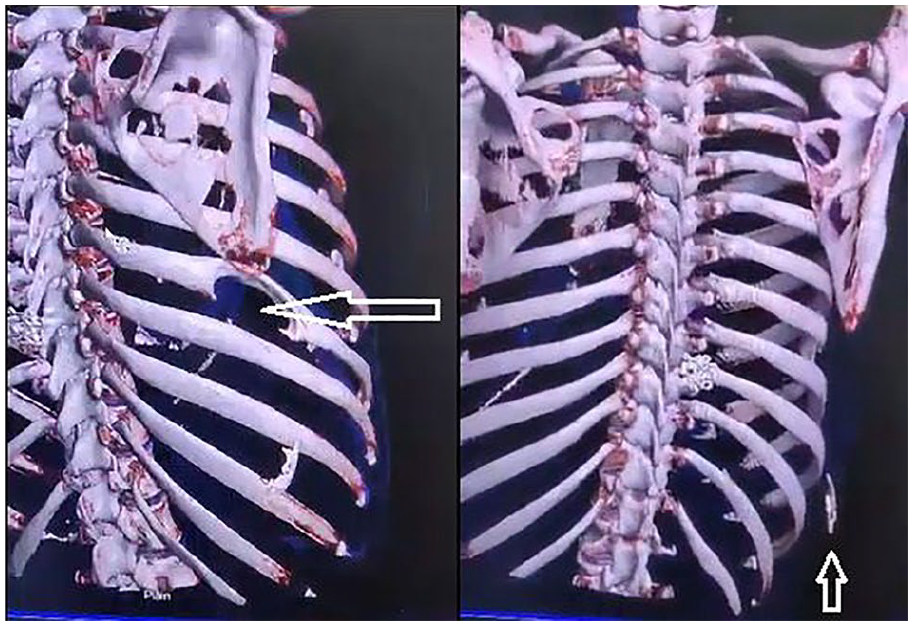
CT scan revealing destruction of seventh rib with a piece of sequestrum in the inferior aspect respectively.
Therapeutic Intervention
The sequestrum was excised under local anesthesia (2% lidocaine infiltration), and the remainder of the rib was preserved to maintain structural integrity. The patient was discharged with oral antibiotics and analgesics. The pus culture and biopsy reports confirmed chronic rib osteomyelitis, ruling out tubercular or other infections.
Follow-Up and Outcomes
The patient was initially followed up after 1 week at the outpatient department of the tertiary hospital’s orthopedic unit. She reported improvement in symptoms, and the surgical site appeared healthy with no signs of new infection. The wound was dressed, and the sutures were removed during her second follow-up 2 weeks later. She was advised to attend weekly follow-ups for 6 weeks, followed by follow-ups at 3 months, 6 months, and 1 year. At her most recent follow-up, the patient remained asymptomatic with a well-healed incision site.
Discussion
A retrospective study in Nepal on chronic osteomyelitis cases found that the condition predominantly affects males (63%) and young individuals under 30 years of age, with the femur and tibia being the most commonly involved bones. 4 Osteomyelitis in adults is generally uncommon, typically involving the vertebrae and pelvis when it does occur.5,6 In contrast, osteomyelitis is more common in children, where it usually affects the metaphysis of long bones like the tibia and femur. 6 Studies found chronic osteomyelitis in 19% of cases in children among 163 osteomyelitis cases with rib involvement in just 1 case which signifies involvement of ribs is extremely unusual. 7 Also, the higher prevalence of chronic osteomyelitis in males as shown by many studies makes this case of female particularly uncommon.8,9
The higher prevalence of chronic osteomyelitis in males further highlights the rarity of this case in a female patient. While chronic osteomyelitis is commonly reported in adults, reports involving young adults are limited. A similar case of rib osteomyelitis in an 18-year-old male was reported by Altaf et al, 7 but no cases have been reported in young adult females to date, highlighting this case exceptionally rare.
The usual symptoms of rib osteomyelitis include chest pain, fever, and elevated inflammatory markers. 7 In our patient, findings such as elevated WBC count and CRP levels, pain and discharging sinus over the affected site were typical of rib osteomyelitis. 10 Empyema thoracis and blunt chest trauma are major causes of rib osteomyelitis; however, neither was associated with our patient. 7
Chronic osteomyelitis is often marked by the presence of necrotic bone or sequestrum, a feature also observed in this case.2,3 Hematogenous spread is the most common route for osteomyelitis, typically affecting metabolically active regions of bones rich in blood supply, like the costochondral junction anteriorly and the costovertebral angle posteriorly. 7 However, in this case, the infection was localized to the postero-lateral region of the seventh rib, which is an atypical site, suggesting a possibility of an alternative etiology, such as a prior subclinical infection, localized trauma, or hematogenous spread, which may have contributed to the unusual presentation.
Staphylococcus aureus is the most commonly isolated pathogen in osteomyelitis cases.1,8 However, the biopsy in our patient did not reveal any organisms, including Acid-Fast Bacilli (AFB), nor were there atypical cells, which ruled out bacterial and tubercular osteomyelitis. The clinical history, findings and lab parameters in this case are suggestive of Chronic Osteomyelitis with infective etiology.
Treatment of rib osteomyelitis typically involves a combination of surgical debridement and prolonged antibiotic therapy. In the absence of culture findings, an empirical antibiotic regimen was initiated in our case, considering the common pathogens associated with rib osteomyelitis. The patient was treated with a second-generation cephalosporin that is cefuroxime, chosen for its high bone penetration, to cover potential infections despite negative culture results.
Strength and Limitations
This case report documents one of the earliest cases of chronic rib osteomyelitis in a young adult female from Western Nepal. By sharing this case, we aim to raise awareness of rare presentations like this, which may otherwise go undiagnosed in resource-limited settings.
Conclusion
This case illustrates the importance of considering chronic rib osteomyelitis in differential diagnoses for adult females presenting with atypical symptoms and rib abnormalities. Due to its nonspecific presentation and rarity, rib osteomyelitis may often be misdiagnosed, highlighting the need for a high index of suspicion among clinicians.