
Abstract
A case of spontaneous bilateral internal carotid artery dissection (ICAD) in a 36-year-old male, potentially linked to COVID-19, is reported. Initially presenting with excessive daytime sleepiness, an atypical symptom for ICAD, the patient lacked focal neurologic deficits. Diagnostic evaluation revealed severe stenosis and dissecting aneurysms in both carotid arteries. Treatment included anticoagulation, corticosteroid therapy, and subsequent endovascular stent placement. This case underscores the importance of considering ICAD as a potential complication of COVID-19, especially in patients with atypical symptoms. Further research is needed to understand the underlying mechanisms and optimize treatment strategies.
Keywords
Case Presentation and Treatment
A 36-year-old male, presented to the emergency department with chief complaints of excessive daytime sleepiness, beginning a week prior. His symptoms included increased sleepiness and reduced communication, without focal neurologic deficits.
The patient experienced classical symptoms of COVID-19 1 month previously including Fever, Muscle or joint pain, and an influenza-like illness. The patient tested positive for antibodies specific to Coronavirus-2 (SARS-CoV-2). He had no significant past medical history, and no family history of genetic diseases. There was also no history of neck trauma, including manipulation or vigorous exercise, and the patient had no history of smoking or alcohol consumption.
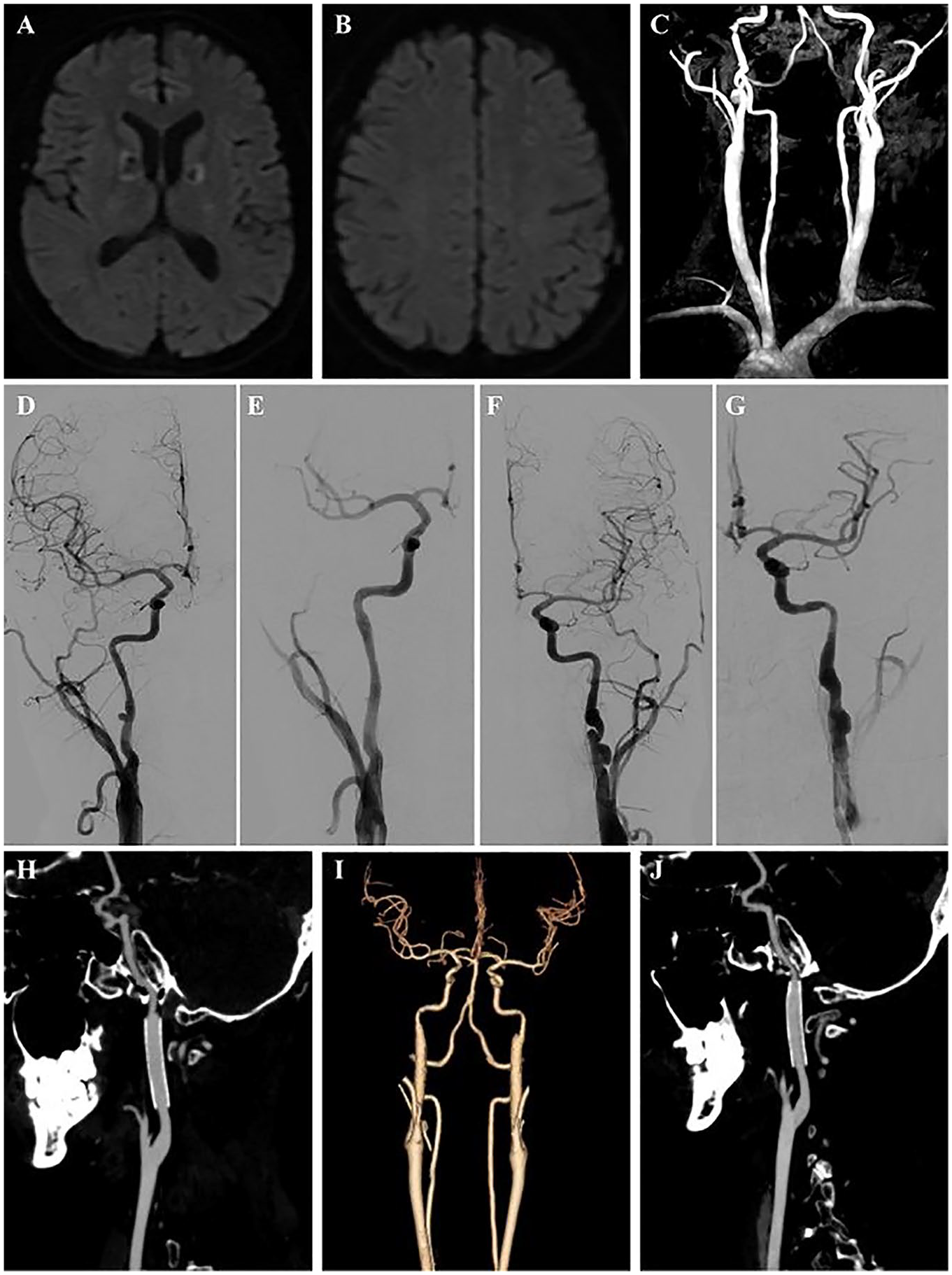
Initial clinical examination showed normal results with no neurological signs. The patient’s Glasgow Coma Score was 15. Initial CT imaging at presentation revealed low-density lesions in the bilateral basal ganglia and mild lung inflammation. Routine blood, urine, and stool tests were normal. Comprehensive testing, including liver and renal function, blood glucose, and autoimmune markers, showed no abnormalities. Furthermore, a lumbar puncture was also performed, which was negative for any pathologic condition. The brain Magnetic resonance imaging (MRI)-diffusion-weighted imaging (DWI) revealed scattered areas of restricted signals in various regions (Figure 1A and B), while MR angiography (MRA) showed no intracranial vessel abnormalities (Figure 1C). MRI findings suggested a watershed infarct type of ischemic stroke, leading to a digital subtraction angiography (DSA). DSA revealed severe bilateral internal carotid artery (ICA) stenosis with dissecting aneurysms (Figure 1D and E). High-resolution MRI confirmed this, showing a ‘double lumen’ and ‘pearl-and-string’ sign, indicative of vascular wall pathology (Figure 1F and G). To rule out large vessel vasculitis and hereditary factors, abdominal vascular ultrasound and a CT angiogram (CTA) on the patient’s brother were performed, both yielding normal results.

Initial diagnostic neuroimaging findings. MRI-brain DWI showing bilateral basal ganglia (A) and left frontal and parietal lobe diffusion restriction (B). MRA revealing normal intracranial blood vessels (C). DSA demonstrated segmental narrowing and aneurysm formation at the bilateral ICAs (D and E). High-resolution MRI of vessel walls demonstrated intramural hematoma in bilateral ICAs (F and G).
The patient, diagnosed with spontaneous bilateral ICAD and watershed infarctions, initially received rivaroxaban treatment. However, by the fourth day, a marked decline in cognitive functions was noted, characterized by symptoms such as flattened affect, disorientation, impaired memory, and unsteady gait. The Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA) are used to assess cognitive changes in the patients, with scores of 10 and 15, respectively. Given the potential association with a prior COVID-19 infection, a decision was made to initiate a course of steroids (prednisone, 60 mg/day) following expert consultation. Substantial cognitive improvement was observed within a month, with both MMSE and MoCA scores increasing to 30. Follow-up MRI/MRA showed improved patency in the carotid arteries, mild residual stenosis, and no new infarctions (Figure 2A and B). Nevertheless, the development of entrapment aneurysms in both ICAs, especially on the left side (Figure 2C), necessitated the implantation of Carotid stents in both arteries. Specifically, Precise Pro Rx stents measuring 7 × 40 mm were deployed under local anesthesia. The patient was maintained on dual-antiplatelet therapy for 3 months, with subsequent follow-up CTA confirming the patency of the ICA and the resolution of dissecting aneurysm (Figure 2H–J).
Post-treatment follow-up neuroimaging findings. MRI-brain DWI reveals no new cerebral infarctions, while MRA indicates improved lumen patency in the bilateral ICAs at 3 months (A–C). DSA revealed improved ICA stenosis compared to 3 months prior, but a localized dissecting aneurysm had formed. Following stent implantation, blood flow became unobstructed, and the aneurysm disappeared (D–G). Three-Month Follow-up CTA showed unobstructed lumen post-stenting (H–J).
Discussion
Carotid artery dissection (CAD) is a primary stroke cause in individuals under 50. 1 It typically manifests as unilateral head, facial, or neck pain, sometimes with partial Horner’s syndrome, leading to cerebral or retinal ischemia. To the best of our knowledge, although there have been previous reports of internal capsule infarction that resulted in isolated abulia without motor weakness, they have all been limited to unilateral cases.2,3 The genu of the internal capsule, anterior to the thalamus and nourished by the internal carotid artery, plays a critical role in brain connectivity. An infarct here disrupts thalamocortical fibers, potentially causing cognitive and behavioral changes like amnesia and apathy, due to thalamocortical disconnection syndrome affecting cortical-subcortical-frontal loop. 4 The severe bilateral stenosis of the ICA and resultant watershed infarction may lead to similar changes via global cerebral hypoperfusion, highlighting the need for deeper understanding of cognitive impacts associated with bilateral internal capsular genu infarcts.
The etiology of spontaneous bilateral ICAD is not fully understood, with a mix of genetic and environmental factors implicated. 1 This includes a small percentage of cases with heritable connective tissue disorders like fibromuscular dysplasia, Marfan syndrome, and Ehlers-Danlos syndrome. Risk factors such as hypertension, hypercholesterolemia, smoking, and oral contraceptive use are also known. Notably, our patient lacked significant medical history, trauma, or family history of connective tissue disorders, and no definitive cause was found despite thorough evaluation. The patient reported symptoms indicative of COVID-19 a month before presentation, suggesting that COVID-19 could be the cause. A 2022 review indicates an increased incidence of ischemic stroke in COVID-19 patients, with distinct clinical features specific to strokes related to the virus. 5 Notably, recent case reports have presented evidence suggesting a potential association between COVID-19 infection and CAD,6,7 with some suggesting that COVID-19 might directly affect vascular tissues via ACE2 receptors, leading to endothelial dysfunction and thrombosis. 8 Additionally, a recent systematic review highlights the significance of COVID-19 as an independent risk factor for ischemic heart disease. 9 While primarily impacting the respiratory system, COVID-19 also manifests substantial cardiovascular effects, including myocardial damage, arrhythmias, and thromboembolic events. However, to comprehensively elucidate the potential role of COVID-19 infection in the pathogenesis of CAD, further rigorous investigations are warranted.
Given the lack of established guidelines for CAD management, individualized treatment plans are crucial. Our patient received first-line anticoagulation therapy, aligning with evidence suggesting similar efficacy of novel oral anticoagulants with vitamin K antagonists in CAD. 10 However, the patient’s condition deteriorated during hospitalization, prompting the addition of corticosteroid therapy, beneficial in large vessel vasculitis and certain inflammatory CAD cases. 11 This approach resulted in significant cognitive improvement, consistent with similar cases. 3 Post-treatment, follow-up MRA revealed marked improvement in bilateral internal carotid artery stenosis, but also the emergence of bilateral internal carotid artery dissection aneurysms, leading to endovascular stent placement, a recognized method for treating aneurysmal CAD. 12 However, the optimal timing, technique, and long-term efficacy of endovascular stent placement for CAD remain to be defined. While our patient showed clinical improvement with an individualized treatment approach involving anticoagulation and corticosteroid therapies, it is noteworthy that the ICAD and the damage to the internal capsule both possess some degree of inherent self-repair capability, which complicates the determination of the precise extent to which pharmacotherapy contributed to the patient’s convalescence.
Conclusion
In summary, this case highlights the complexities in the diagnosis and management of bilateral ICAD, particularly when confronted with nonspecific or asymptomatic manifestations, such as isolated volitional extinction. While the potential connection between COVID-19 infection and spontaneous bilateral ICAD is intriguing, it is currently supported only by limited and largely circumstantial evidence. Consequently, it is crucial to consider a patient’s recent COVID-19 history alongside other potential causative factors, albeit with cautious interpretation. Extensive research is therefore essential to fully understand these links and to develop personalized and effective therapeutic strategies that optimize patient outcomes.