
Abstract
Chilaiditi’s sign is a rare radiological finding characterized by colonic interposition between the liver and the right hemidiaphragm. It is a cause of pseudopneumoperitoneum which is often mistaken for true pneumoperitoneum. In this article, we present the case of a 73-year-old female with a previous history of pulmonary tuberculosis, who reported to our hospital with progressive abdominal distension associated with early satiety, bipedal swelling, generalized weakness, worsening fatigue, and weight loss. Following evaluation, she was diagnosed with liver cirrhosis and chronic lymphocytic leukemia. Her chest radiograph also incidentally showed air under the right hemidiaphragm with haustral folds consistent with Chilaiditi’s sign. Since she did not have signs of peritonitis, she was eventually treated for liver cirrhosis and chronic lymphocytic leukemia without undergoing any surgical intervention. This case report seeks to create awareness among clinicians about this rare radiological sign in order to prevent misdiagnosis leading to unnecessary surgical procedures.
Keywords
Introduction
Chilaiditi’s sign refers to a rare radiological finding characterized by interposition of the bowel, usually colon, between the liver and the right hemidiaphragm. 1 It was first described in 1910 by a Greek radiologist called Demetrius Chilaiditi. 2 The hepatic flexure and proximal transverse colon are the most frequently interposed bowel segments. Small bowel involvement rarely occurs. 3
Chilaiditi’s sign is discovered incidentally on chest or abdominal radiographs. 3 It is a cause of pseudopneumoperitoneum 1 and may occur permanently or sporadically. 4 Globally, its incidence ranges from 0.025% to 0.28% 5 and predominantly occurs in males with a male-to-female ratio of 4:1. 6 It is also commonly seen in persons older than 60 years. 3 Although the exact etiology of Chilaiditi’s sign is not fully understood, 3 several predisposing factors associated with the occurrence of this rare entity have been described. Most of the predisposing factors are diaphragmatic, hepatic or colonic in origin. 7 This radiological anomaly is benign and tends to present asymptomatically. 8 Occasionally, hepatodiaphragmatic interposition of the colon may present with symptoms such as abdominal pain, nausea, vomiting, anorexia, constipation, respiratory distress, and retrosternal chest pain. When this occurs, it is referred to as Chilaiditi’s syndrome.3,7,8
It is worth noting that Chilaiditi’s sign can easily be misdiagnosed as true pneumoperitoneum, resulting in unwarranted surgical interventions. 9 Other important differential diagnosis for pseudopneumoperitoneum are basal linear atelectasis, pneumomediastinum, pseudo-Rigler sign, diaphragmatic undulation, fat within the subphrenic space and biliary, portal vein, or bowel wall gas. 10 In this article, we discuss an elderly patient with a previous history of pulmonary tuberculosis who was incidentally found to have Chilaiditi’s sign during evaluation for liver cirrhosis and chronic lymphocytic leukemia.
Case Presentation
A 73-year-old non-alcoholic female reported to the emergency unit of Methodist Hospital, Wenchi, Ghana with a complaint of gradually progressive abdominal distension which started about a month prior to presentation. This was associated with early satiety, bipedal swelling, generalized weakness, worsening fatigue, and weight loss. However, she did not have yellowish discoloration of the eyes, melena, hematemesis, reversed sleep pattern, itchiness, dark urine, or pale stools. There was also no constipation, vomiting, anorexia, abdominal pain, fever, drenching night sweats, exertional dyspnea, orthopnea, or paroxysmal nocturnal dyspnea. She sought medical attention at a health center and also took oral herbal preparation but her symptoms did not improve. She was a hypertensive patient on nifedipine 30 mg daily and had previously been treated for pulmonary tuberculosis more than 20 years ago. She had no previous history of abdominal surgery. There was no family history of liver disease or hematological malignancy. She was neither a cigarette smoker nor an intravenous drug user.
On physical assessment, she was mildly cachectic, afebrile (36.3°C), anicteric, not pale, and not dyspneic. Her oxygen saturation was 95% on room air. She had bipedal pitting edema up to mid-shin but there was no peripheral lymphadenopathy, palmar erythema, or finger clubbing. Her Glasgow Coma Scale score was 15/15 with no flapping tremors. Pulse and blood pressure were 104 beats per minute and 132/75 mmHg respectively. Jugular venous pressure was not raised and precordial examination was normal. Respiratory assessment revealed respiratory rate of 18 cycles per minute, tracheal deviation to the left side and minimally reduced air entry in the left lung zones with vesicular breath sounds. Her abdomen was grossly distended, soft and mildly tender in the epigastrium. There was however, no guarding or rebound tenderness. She had a liver span of 5 cm and splenomegaly of 8 cm below the left costal margin. Fluid thrill was positive with normal bowel sounds on auscultation.
Laboratory investigations showed markedly elevated white cell count with lymphocytosis. Also noted were anemia, neutropenia, and thrombocytopenia (Table 1). Subsequent peripheral smear examination demonstrated small, mature-appearing lymphocytes with condensed chromatin and smudge cells (Figure 1). Serum uric acid and lactate dehydrogenase levels were high. However, renal function and serum electrolytes were normal. Flow cytometric immunophenotyping was not done because this service is unavailable in the part of our country where the patient was hospitalized. She had elevated international normalized ratio with deranged liver biochemistries and also tested positive for hepatitis B surface antigen. Her random blood sugar and serum ascites albumin gradient (SAAG) were 10.5 mmol/l and 1.3 g/dl respectively. Table 1 captures the results of all relevant laboratory tests of the patient. Abdominal ultrasonography showed a shrunken liver with coarse parenchymal echotexture and irregular margins. There was massive ascites and splenomegaly (15.9 cm) with homogeneous echotexture. The calculated Child-Pugh score was 11. Resting 12-lead electrocardiogram revealed sinus tachycardia (Figure 2). Plain chest radiographs taken on the first and third days of admission showed air under the right hemidiaphragm with the appearance of haustral folds within the air. Also noted were left tracheal deviation and reduced left lung volume (Figure 3) which were suggestive of pulmonary fibrosis. Upon consultation with a general surgeon and further discussion with a radiologist in another hospital via telephone, there was consensus that the presence of haustra within the air under the right hemidiaphragm in the absence of signs of peritonitis was consistent with Chilaiditi’s sign. Upper gastrointestinal endoscopy was done later which showed grade 2 esophageal varices (Figure 4). Computed tomography (CT) scan and pulmonary function test for further evaluation of the pulmonary fibrosis were requested but the patient could not afford.
Initial laboratory results of the patient.

Abbreviations: ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma glutamyl transferase; HIV, human immunodeficiency virus; INR, international normalized ratio.

Peripheral blood smear showing small, mature-appearing lymphocytes with condensed chromatin (yellow arrow). Also present are smudge cells (red arrow).
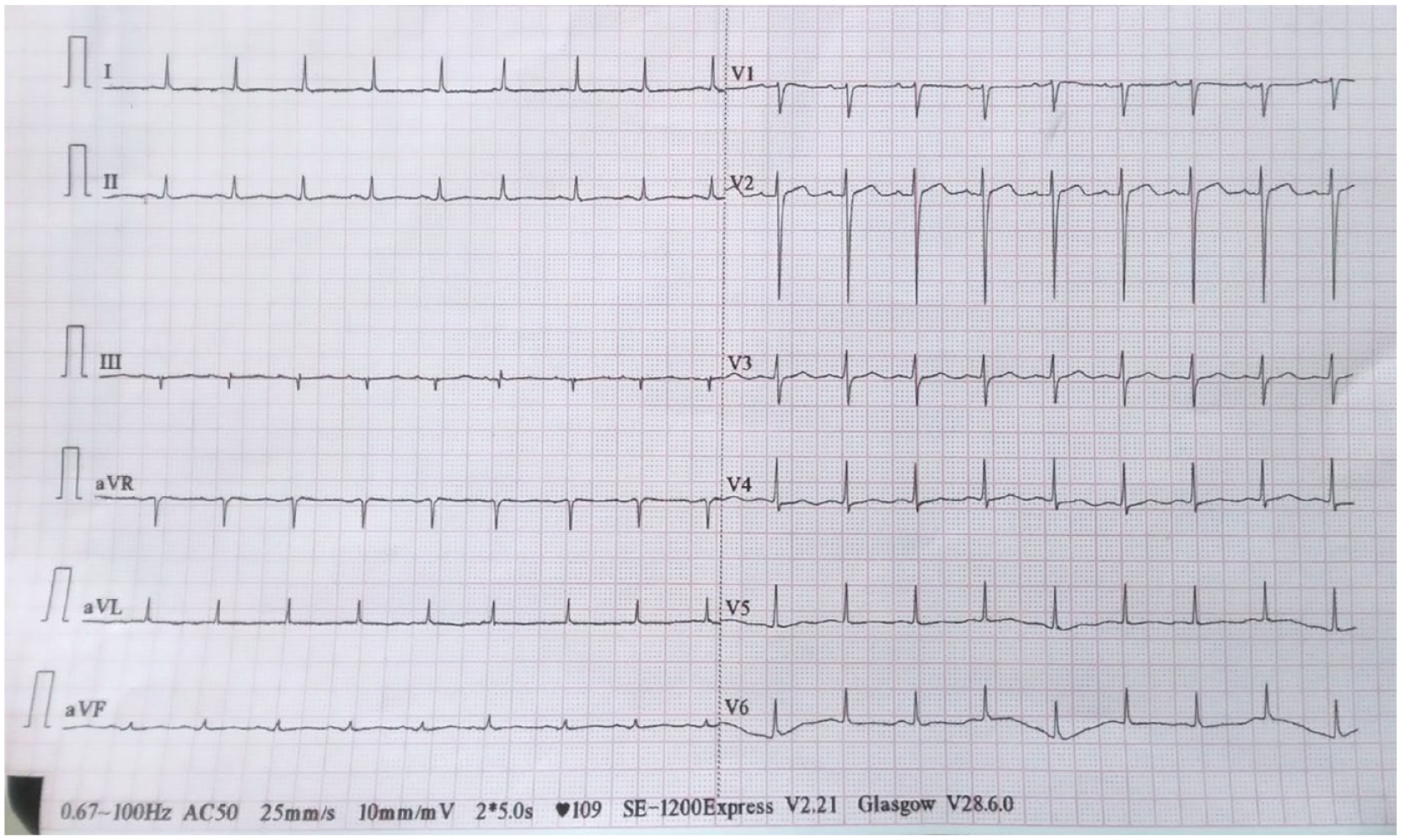
Resting 12-lead electrocardiogram showing sinus tachycardia.
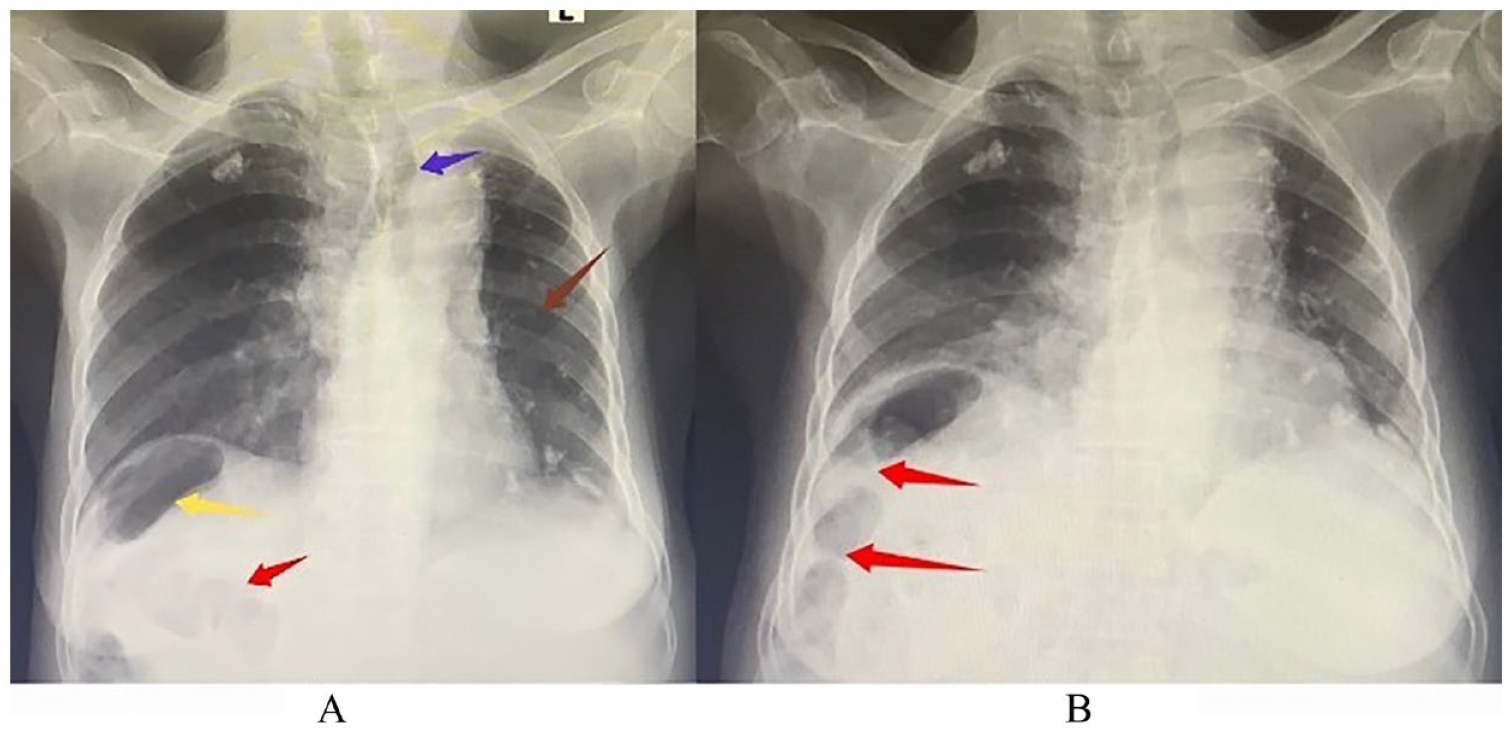
(A) Plain chest radiograph taken on the first day of admission. It demonstrates air under the right hemidiaphragm (yellow arrow) with the appearance of haustral folds within the air (red arrow). There is tracheal deviation to the left (blue arrow) as well as reduction of left lung volume (brown arrow). (B) Chest radiograph repeated on day 3 of admission still showing haustra within the air under the right hemidiaphragm (red arrow). This indicates the air is within the bowel lumen and not free (Chilaiditi’s sign).

Endoscopic image of the patient showing grade 2 esophageal varices.
Based on the above, the patient was diagnosed with liver cirrhosis (Child-Pugh C) secondary to chronic hepatitis B viral infection complicated by portal hypertension, gross ascites, and esophageal varices. Additional diagnoses were Rai stage IV chronic lymphocytic leukemia (CLL), post-tuberculosis pulmonary fibrosis and Chilaiditi’s sign. The hyperuricemia associated with CLL was treated with adequate intravenous hydration and febuxostat 40 mg daily. Urethral catheterization was done to monitor her urine output which was adequate throughout the period of admission. Therapeutic abdominal paracentesis, diuretic therapy (furosemide 40 mg daily and spironolactone 100 mg daily) and restriction of daily salt intake to <2 g were instituted to treat the gross ascites. Her weight was monitored daily till a targeted loss of 1 kg per day was achieved since she had gross ascites together with bipedal edema. She was also started on tenofovir disoproxil fumarate 300 mg daily and carvedilol 3.125 mg twice daily. She did not undergo any surgical intervention because Chilaiditi’s sign is a benign radiological finding. After 10 days of hospitalization, her general condition had improved. The bipedal edema completely resolved with significant reduction of the ascites. Repeated serum uric acid was normal (169 umol/l). Following discharge, she was referred to a tertiary center for endoscopic variceal ligation as we currently do only diagnostic endoscopy in our hospital. She was also referred to see a hematologist for further assessment and possible initiation of chemotherapy.
Discussion
Under normal circumstances, suspensory ligaments and fixation of the colon prevent entrapment of the colon between the liver and the right hemidiaphragm. 11 Alterations in the anatomic relationship between these 3 organs can lead to hepatodiaphragmatic interposition of the colon5,11 which manifests radiographically as Chilaiditi’s sign.
There are several predisposing factors for Chilaiditi’s sign. Cirrhosis and hepatectomy reduce the size of the liver. This enlarges the right subphrenic space, making it easier for colonic interposition to occur. Laxity of the falciform ligament also predisposes to Chilaiditi’s sign. 12 Phrenic nerve palsy and congenital absence of muscular fibers of the diaphragm result in elevation of the right hemidiaphragm. Again, this widens the right subphrenic space, thus increasing the risk of colonic interposition. 7 In individuals with abnormally long large intestine (dolichocolon), the extra length of colon can be entrapped between the liver and the diaphragm. Congenital absence or elongation of the suspensory ligaments of the transverse colon may also cause Chilaiditi’s sign. 13 Other predisposing factors include ascites, obesity and post-operative intra-abdominal adhesions.12,14,15 Additionally, hepatodiaphragmatic interposition of the colon has been reported in association with acute cholecystitis. 16 To the best of our knowledge, this is the first case report associating Chilaiditi’s sign with the simultaneous occurrence of liver cirrhosis and CLL. Our patient’s predisposing factors were liver cirrhosis and gross ascites. The most plausible explanation for the occurrence of Chilaiditi’s sign in our patient is that, ascites increases intra-abdominal pressure which can cause migration of the colon into the enlarged subphrenic space created by the cirrhotic liver. 12 In a study that examined chest radiographs of patients, the prevalence of Chilaiditi’s sign among those with liver cirrhosis was reported to be 22%. The majority of these individuals with cirrhosis had moderate to massive ascites 17 as was observed in our case. Also, her age (73 years) falls within the at-risk age group (ie, >60 years). 3
Chilaiditi’s sign is asymptomatic and detected incidentally.3,8 Our patient’s symptoms were mainly attributable to liver cirrhosis and CLL. Chest radiograph findings that are suggestive of Chilaiditi’s sign include elevation of the right hemidiaphragm, air under the right hemidiaphragm and inferior displacement of the liver below the level of the left hemidiaphragm. 13 The presence of haustra within the air is an indication that it is within the bowel and not free. 1 Also, a change in a patient’s position does not alter the position of the air in Chilaiditi’s sign as opposed to true pneumoperitoneum. 12 On abdominal ultrasound, Chilaiditi’s sign is seen as gas echo. Changing the position of a patient does not change the location of the gas echo. 13 CT scan is indicated if chest radiograph and abdominal ultrasound findings are inconclusive.1,13 Our patient’s chest radiograph showed the classic appearance of haustral folds within the air under the right hemidiaphragm. This radiologic finding in the absence of signs of peritonitis or bowel obstruction was in keeping with Chilaiditi’s sign and obviated the need for abdominal CT scan.
The differentiation between Chilaiditi’s sign and true pneumoperitoneum is critically important as the 2 entities are treated differently. Recognizing Chilaiditi’s sign in cirrhotic patients as in our case, can prevent iatrogenic bowel injury during percutaneous transhepatic procedures like liver biopsy. 18 Also, performing colonoscopy in a patient with Chilaiditi’s sign is associated with a high risk of bowel perforation. 18 Nevertheless, prompt and accurate distinction between these 2 entities can be challenging, particularly in resource-constrained settings as pertains to most district hospitals in Ghana.
Unlike true pneumoperitoneum which is a surgical emergency that requires immediate surgical intervention, Chilaiditi’s sign is benign and does not warrant any treatment.3,7,9 For this reason, we concentrated on treating the liver cirrhosis and CLL without subjecting the patient to any surgical procedure. For patients who develop Chilaiditi’s syndrome (ie, Chilaiditi’s sign plus symptoms), conservative management often leads to resolution of symptoms. The conservative approach consists of bed rest, intravenous fluids, bowel decompression, and the use of laxatives. Surgical intervention is indicated only in those who do not respond to conservative management and those who develop complications like bowel wall ischemia, bowel perforation, and intestinal obstruction.3,5,13
Conclusion
Chilaiditi’s sign is a rare radiological finding which is detected incidentally. It is often misdiagnosed as true pneumoperitoneum, leading to unnecessary investigations and surgical procedures. It is therefore, critically important for clinicians to be aware of this radiological sign and be able to differentiate it from true pneumoperitoneum.
Limitations
Further evaluation of the pulmonary fibrosis with high resolution CT scan and pulmonary function test could not be done because the patient was financially constrained.
Footnotes
Acknowledgements
The authors are grateful to the patient for consenting to the publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Abbreviations
CT - computed tomography
CLL - chronic lymphocytic leukemia
Data Availability
All data generated or analyzed are included in this published article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Consent
Written informed consent was obtained from the patient for her information to be published in this article.