
Abstract
Calcifying odontogenic cyst, also known as Gorlin cyst is a rare benign cystic lesion primarily found in the jawbones, accounting less than 1% of odontogenic cysts. It can be associated with odontogenic tumors such as odontomas. We report a rare case of COC associated with complex odontoma in a young patient and discuss its clinical features, diagnosis, and treatment options. An 18-year-old female patient presented with a painless radiopaque lesion of the right mandibular bone at Oral Medicine and Oral Surgery department. Radiographs revealed irregular tooth-like structures in the canine-premolar area. The lesion was surgically removed, and histopathology confirmed COC with a complex odontoma. As of the World Health Organization’s 2022 definition, COC is a developmental odontogenic cyst characterized by calcified ghost cells. It typically affects individuals during their second and third decades of life, with no gender preference, almost equally in the maxilla and the mandible. The main treatment is total enucleation, with a generally favorable prognosis. Histopathology is essential for diagnosis due to its mimicry of other jaw conditions. Long-term follow-up is needed to prevent recurrences.
Introduction
Calcifying odontogenic cyst (COC), also known as Gorlin’s cyst, is an uncommon benign developmental cystic lesion primarily found in the maxillary and mandibular bones, first described as a likely analog of the “calcifying epithelioma of Malherbe” in 1962.1,2 It accounts for less than 1% of all odontogenic cysts. 3 It typically occurs in individuals during their second and third decades of life, almost equally in the maxilla (strong predilection for the anterior), and the mandible. The frequency in men and women is similar with no gender predilection. 4 The classification of this lesion as either neoplastic or cystic has raised questions. In the past, this entity was known as a calcifying cystic odontogenic tumor. However, in both the WHO 2017 and 2022 classifications of odontogenic tumors, it has been reclassified as a developmental cystic lesion.4,5 About 33% of COCs occur concurrently with various types of odontogenic tumors such as odontomas. 6 The aim of this report is to present a case of COC associated with complex odontoma of mandibular bone and to discuss its clinical features, diagnosis, and treatment options.
Case Report
An 18-year-old female patient was referred to Oral Medicine and Oral Surgery department due to the presence of a painless radio opaque lesion of the right mandibular bone. The patient’s medical history did not reveal any specific medical conditions. The extraoral examination was normal, with a normal range of mouth opening. Upon intraoral examination, no abnormalities were observed, and the teeth exhibited vital signs. The mucosa appeared healthy with a normal color and texture. Specifically, the posterior right mandibular teeth were found to be vital. Additionally, there was no evidence of bone deformity. However, radiographic assessments (panoramic radiograph and cone beam computed tomography) disclosed a well-defined, unilocular radio opaque lesion, containing irregular tooth-like structures in the right mandibular canine and first premolar area, located lingually to the teeth. No signs of buccal or lingual cortical bone expansion or thickening, adjacent teeth displacement or root resorption were observed (Figures 1 and 2).
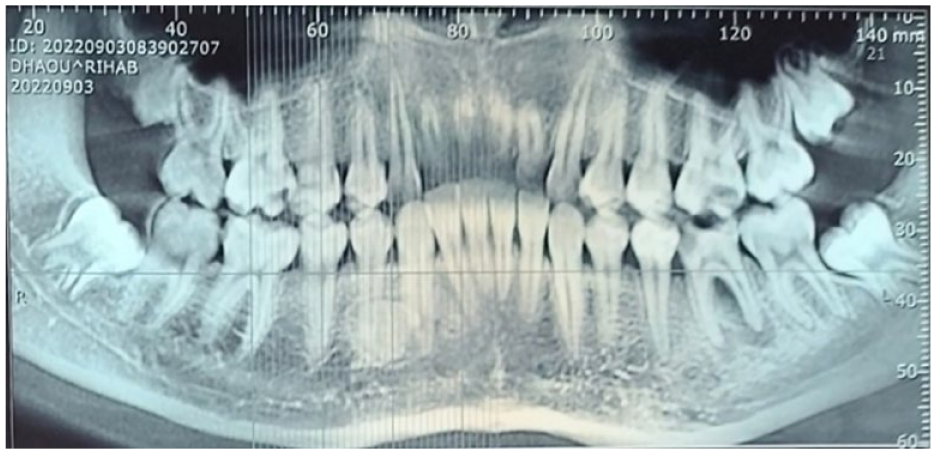
Radiographic examination: panoramic view on cone beam computed tomography disclosed a well-defined, unilocular radio opaque lesion, containing irregular tooth-like structures in the 43-44 area, without tooth displacement. There was no evidence of displacement or root resorption of adjacent teeth.

Radiographic examination: sagittal slices on cone beam computed tomography disclosed a well-defined, unilocular radio opaque lesion, containing irregular tooth-like structures in the 43-44 area, located lingually to the teeth, and No signs of buccal or lingual cortical bone expansion or thickening, adjacent teeth displacement or root resorption were observed.
The diagnosis of COC and complex odontoma has been considered based on clinical and radiological findings. Supporting arguments include the presence of a well-defined, radiopaque lesion with irregular tooth-like structures in the right mandibular canines and first premolars region. The lingual location relative to the affected teeth has also been noted. Additionally, the absence of buccal and lingual cortical bone expansion or thickening, as well as the lack of displacement of adjacent teeth, further supports the diagnosis. Furthermore, no root resorption has been observed. These consistent findings strongly suggest the presence of a COC. The following steps were taken in the surgical removal of the lesion under local anesthesia, employing a lingual flap approach, and performing bone resection to access it. The lesion was easily enucleated by dissecting along the cleavage plane, revealing a cystic lining and a mass of calcified tissues within the lumen (Figure 3).

The lesion was surgically removed under local anesthesia, employing a lingual flap approach, and performing bone resection to access it. The lesion was easily enucleated by dissecting along the cleavage plane.
Subsequently, the specimen was submitted for histopathological examination, which confirmed the diagnosis of complex odontoma for the hard tissue component. The soft tissue specimen revealed a cystic lining composed of ameloblast-like basal cells with reverse polarity and stellate reticulum-like cells. Additionally, the lining contained ghost cells, characterized by their pale, anucleate appearance and distinct outlines, with areas showing calcification. These histopathological features were consistent with the diagnosis of a COC associated with a complex odontoma. After the surgical procedure, the patient was prescribed analgesics (Paracetamol) for pain relief and antibiotics (Amoxicillin) to prevent infection. The patient’s postoperative recovery was smooth and uneventful. A 1-month follow-up examination showed excellent healing at the surgical site, and the neighboring teeth displayed signs of being vital.
Discussion
As of the latest World Health Organization (WHO) definition in 2022, COC is “a developmental odontogenic cyst characterized histologically by ghost cells, which often calcify.” The classification no longer includes the term “ameloblastoma-like epithelium.” 7 COC presents a range of diverse biological characteristics and displays various clinicopathological features. This diversity has led to uncertainty and ambiguity in its nomenclature and classification over time. It has been referred to by different terms, including calcifying cystic odontogenic tumor, calcifying ghost cell odontogenic cyst, and Gorlin’s cyst, among others. 8 The first classification was proposed in 1981, categorizing COC into 2 main types: type I: cystic type, type II: neoplastic type. He further subdivided the cystic variant (Type I) into 3 distinct types: (a) simple unicystic type, (b) odontoma producing type, and (c) ameloblastomatous proliferating type. 8 The WHO’s stance on this entity has evolved over the years. In 1992, it was considered as a tumor, 9 and in 2005, it was referred to as calcifying cystic odontogenic tumor. 10 However, the more recent WHO Classification of Head and Neck Tumors in 2022 has designated it as COC. Under the current WHO classification, COC is used for cystic lesions and dentinogenic ghost cell tumor for the neoplastic entities. 7 COC is rare, accounting for less than 1% of all odontogenic cysts. It typically occurs in individuals during their second and third decades of life with no gender preference, almost equally in the maxilla (strong predilection for the anterior), and the mandible. 11 It has been associated with β catenin (CTNNB1) mutations. 7 Its most common presentation involves typically a painless, firm swelling in the jawbone, which gradually expands. In our patient, although the radiographic image indicated a radiopaque lesion, implying a relatively prolonged evolution and maturity of the lesion, there were no discernible clinical signs, neither mucosal nor dental were observed. Less commonly observed symptoms include tooth discoloration and pain if there is a secondary infection. Initial lesions are found incidentally on a routine radiographic examination. 8 Radiographs reveal a well-defined radiolucent lesion, often appearing unilocular and may have a scalloped border. Tooth displacement and root resorption are common. Additionally, about half of all cases exhibit varying amounts of calcified tissue or an associated odontoma, as in the case we discussed earlier.8,11 COCs present unique challenges in differential diagnosis due to their varied clinical and radiographic features. The differential diagnosis of COCs varies with their stages of maturity. In the early, typically radiolucent stages, consideration should be given to dentigerous cysts, developing ameloblastomas and odontogenic keratocysts (OKCs). These conditions share overlapping clinical characteristics but differ significantly in their management and prognosis.
Ameloblastomas are benign but locally aggressive odontogenic tumors that require precise diagnosis and treatment planning. Recent studies highlight their epidemiology and management across various centers in Europe. For instance, a multicenter study by Boffano et al examined the epidemiology and management of ameloblastomas, emphasizing the need for a thorough diagnostic workup to differentiate them from other odontogenic cysts and tumors, including COCs. 12 OKCs, now classified as keratocystic odontogenic tumors (KCOTs), also pose diagnostic challenges due to their aggressive behavior and high recurrence rates. Another European multicenter study by Boffano et al focused on the epidemiology and management of OKCs, highlighting the importance of distinguishing them from COCs through histopathological examination and imaging techniques. 13
As the lesion matures, it amy present with similar radiographic features to calcifying epithelial odontogenic tumors and adenomatoid odontogenic tumors. However, it is important to emphasize that at mature stages, COCs often become radiopaque. In this stage, differential diagnoses could include odontomas, cementoblastomas, and cemento ossifying fibromas.14,15
This diagram summarizes the differential diagnosis of COCs based on their stage of maturity and radiographic appearance (Figure 4).

Differential diagnosis of calcifying odontogenic cysts based on their stage of maturity and radiographic appearance.
The mainstay of treatment for COC is total enucleation followed by curettage. 16 Its microscopic features are epithelial basal lining arranged in a cuboidal/columnar fashion and simulate that of ameloblasts. In the suprabasal layers, a cellular pattern reminiscent of the stellate reticulum of the enamel organ is commonly observed. Ghost cells represent the distinctive histopathological feature of COC, appearing as eosinophilic cells devoid of a nucleus. Over time, these ghost cells may become calcified. 8 The essential histological diagnostic criteria for COC, according to the WHO 2022 classification, include the presence of a cystic architecture and the observation of numerous ghost cells. 7 Recurrences of COC are quite rare and are primarily influenced by the thoroughness of cyst removal during the surgical procedure. 17 The prognosis for individuals with COC is generally favorable.
To contextualize our findings, we compared our case with similar case reports from the literature (Table 1). This table summarizes key aspects of each case, including patient demographics, clinical presentation, radiographic and histopathological findings, treatment provided, and outcomes.
Comparison of similar case reports in the literature.
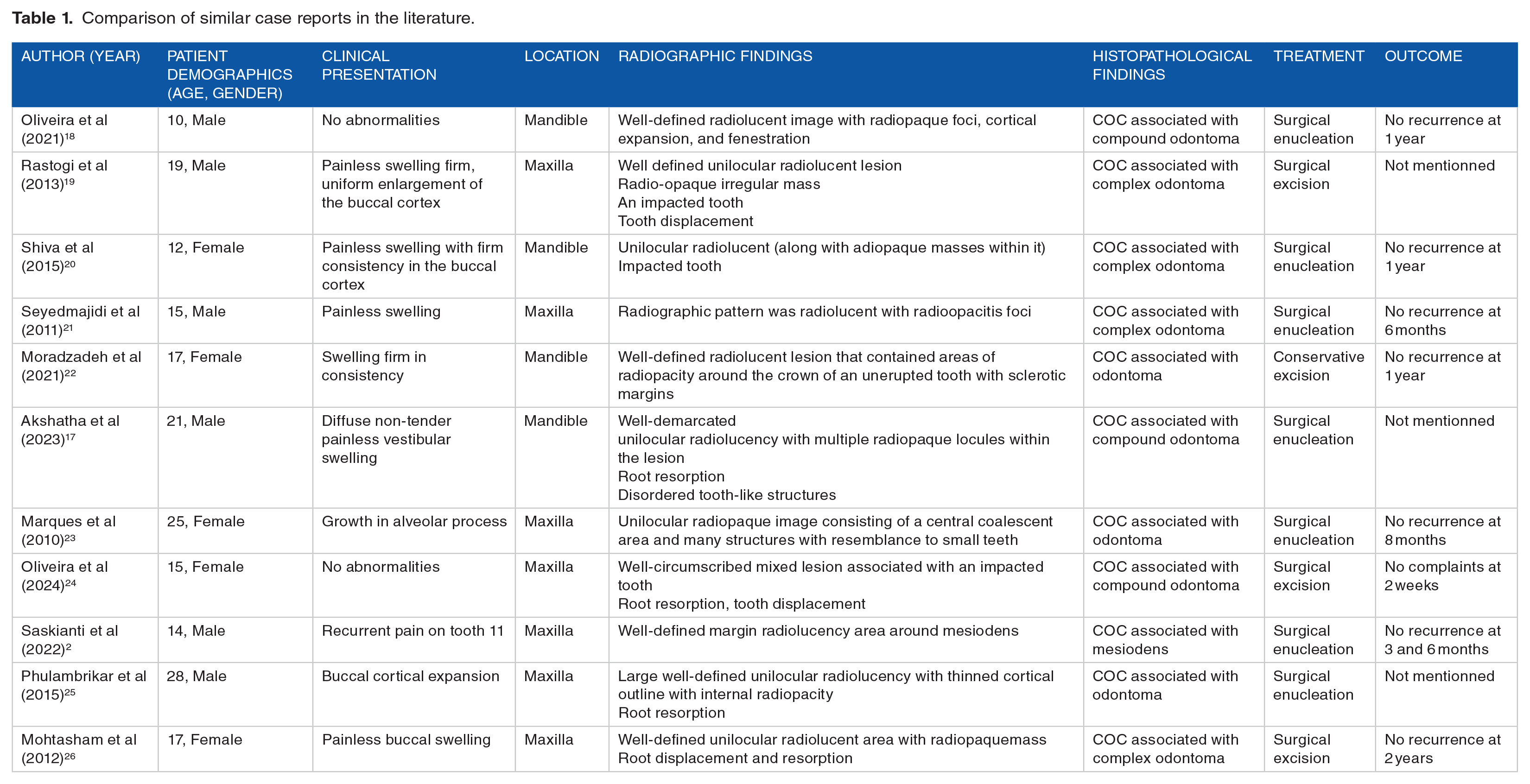
Our case shares common features with previously reported cases, such as the young age of the patient and the histopathological confirmation of a COC associated with a complex odontoma. However, our case is unique due to the presence of radiopaque lesion without any associated bone deformity.
The presence of a COC associated with a complex odontoma has significant clinical implications. its variable radiographic appearance, which ranges from radiolucent in early stages to radiopaque in mature stages, necessitates careful differential diagnosis to distinguish it from other odontogenic lesions. Accurate diagnosis requires a multidisciplinary approach, involving clinical examination, imaging, and histopathological analysis. Surgical management through excision or enucleation, is crucial to minimize recurrence risk, with a generally favorable prognosis when the lesion is completely removed. Although malignant transformation is rare, continuous follow-up is recommended to monitor for any signs of malignancy and promptly address complications. In summary, while COCs associated with complex odontomas demand careful diagnosis and management, the prognosis is positive with appropriate surgical intervention and diligent follow-up.
Conclusion
COC is an unusual developmental odontogenic cyst that often presents clinical and radiological features like other more common jaw conditions. The lesion has always been a topic of ambiguity and has resulted in various nomenclature and classifications over time. Given its varied clinical and imaging presentations, histopathological interpretation remains the key for diagnosis. Long‑term follow‑up is recommended to monitor and prevent recurrences.
Footnotes
Acknowledgements
We would like to thank the LR12SP10 Research Laboratory, University of Sousse for their invaluable support and resources in conducting this study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
IA: data collection, conceptualization, and writing—original draft preparation. LO: supervision, validation, and critical review of the manuscript. RBC: supervision, validation, and critical review of the manuscript. SBY: formal analysis, validation, and critical review of the manuscript.
Informed Consent
A written informed consent for patient information and images to be published was provided by the patient.