
Abstract
Paeniclostridium sordellii, a spore-forming anaerobic Gram-positive rod commonly found in soil samples, is rarely associated with human disease. The authors report a rare case of P. sordelli osteomyelitis of the left distal femur in a young male patient, which is the first reported case of P. sordelli from Pakistan. A 21-year-old male, laborer by profession, presented with low-grade fever, fatigue and lethargy since more than a month, which progressed in severity over the last 2 weeks. On CT scan, abnormal thickening of the cortical bone along with encroachment of the medullary cavity was observed in the left distal femur. A diagnosis of acute osteomyelitis was made and surgical intervention was performed to remove infected bone and soft tissue, which were sent for culture to the Microbiology laboratory. Bone and soft tissue cultures yielded no growth after 72 hours of aerobic incubation. However, bacterial growth was observed after anaerobic incubation, in bone culture, which was identified as P. sordellii using Vitek® 2 automated system. Penicillin, piperacillin-tazobactam, meropenem, vancomycin and metronidazole were susceptible whereas, clindamycin was resistant in the isolate. The patient was started on metronidazole and after he remained stable with a clean surgical wound and symptomatic management, was discharged on regular follow-up as an out-patient. Since, P. sordelli is rare and highly fatal in most cases, prompt reporting and insights from treated infections could pave the way for successful management.
Keywords
Introduction
Paeniclostridium sordellii, a spore-forming anaerobic Gram-positive rod commonly found in soil samples, is rarely associated with human disease. An estimated 70% of cases of infection result in death, and these cases are primarily associated with trauma, intravenous drug abuse, and gynecological procedures.1,2 Some of the prominent signs and symptoms of infection include leucocytosis, hemoconcentration, and refractory hypotension and it presents similarly to the toxic shock syndrome (TSS). 3 Gas gangrene, myonecrosis, and necrotizing fasciitis have also been reported as manifestations of P. sordelli infection.4,5 Here we report a case of P. sordelli osteomyelitis of the left distal femur in a young male patient.
Case Presentation
A 21-year-old male of low socioeconomic background and laborer by profession, had a history of giant cell tumor of the left distal femur for which surgical removal and bone grafting was performed in September 2022. He presented to the out-patient department in January 2024, with complaints of undocumented low-grade fever, fatigue and lethargy since more than a month, which progressed in severity over the last 2 weeks. The patient has been involved in physical labor work at a construction site and reported minor injuries to his lower legs on 2 separate occasions over the past 6 months. On general physical examination the patient was febrile (39.3°C), tachycardic (160 bpm), tachypneic, and sick looking. No wounds were visible on the lower legs at the time of examination. Patient was admitted in high dependency unit (HDU) for further workup and management.
On CT scan, abnormal thickening of the cortical bone with sclerotic changes along with encroachment of the medullary cavity was observed in the left distal femur. A diagnosis of acute osteomyelitis was made on clinical and radiological grounds and empirical treatment with vancomycin and ceftriaxone was initiated. Surgical intervention was performed and the involved area was debrided with wide margins in order to remove the entire necrotic bone and soft tissue, which were sent to the clinical laboratory for microbiological assessment along with 2 sets of blood culture.
Bone and soft tissue cultures yielded no growth after 72 hours of aerobic incubation. However, growth of bacterial colonies was observed after anaerobic incubation, in 2 out of 3 bone samples. Colonies were flat, opaque and gray colored with serrated borders (Figure 1A). Gram stain of colonies revealed gram-positive rods with box-car shaped morphology. Identification of the isolate was confirmed using Vitek 2 ANC card – Vitek® 2 automated system, which was identified as Paeniclostridium sordellii. Antimicrobial susceptibilities were performed by Disk Diffusion method and interpreted using the European Committee on Antimicrobial Susceptibility Testing (EUCAST) clinical breakpoint table v 14.0 6 (Figure 1B). Penicillin, piperacillin-tazobactam, meropenem, vancomycin and metronidazole were susceptible whereas, clindamycin was resistant in the isolate. Minimum Inhibitory Concentration (MIC) of the antibiotics were also determined via the E-test method and was interpreted in accordance with the clinical breakpoints mentioned in the Clinical & Laboratory Standards Institute (CLSI) M100 guidelines 7 (Table 1). Moreover, both sets of blood culture were reported as negative. The patient was started on metronidazole and after he remained stable with a clean surgical wound and symptomatic management, was discharged on regular follow-up as an out-patient. Patient showed further improvement in systemic symptoms over 1 month following discharge from the hospital and hence, metronidazole was stopped after approximately 6 weeks of parenteral therapy.
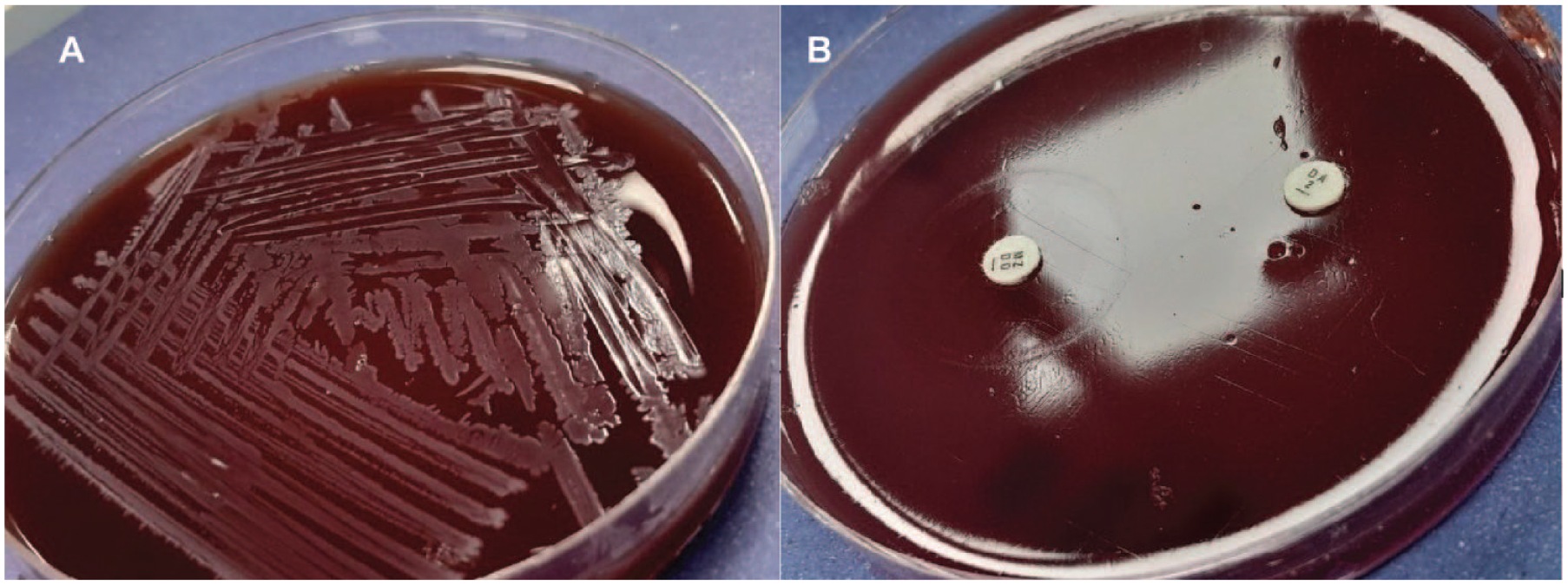
(A) Colonies of P. sordelli on 5% Sheep Blood Agar and (B) antimicrobial susceptibility performed by disk diffusion method.
Minimum inhibitory concentration (MIC) of antibiotics against P. sordelli using E-test method.

Abbreviations: S, sensitive; R, resistant.
Discussion
P. sordellii is commonly found in soil and in the gastrointestinal tract of animals, and human disease is associated with intravenous drug use, medical abortion, and childbirth. 2 A group of 45 P. sordellii infections had an overall mortality of 69%, according to a case review by Vidor et al. 3 Additionally, mortality was noted in all cases of spontaneous, medical, and childbirth abortions. Most fatal cases (80%) had deaths within 2 to 6 days of initial presentation, with the typical clinical course being a rapidly progressing infection.3,8 Even though most infections are fatal, the organism’s pathogenicity is mostly dependent on the presence of its 2 main toxins, lethal toxin (TcsL) and hemorrhagic toxin (TcsH). 3 Similarities exist between TcsH and TcsL and the A and B toxins of Clostridium difficile, which lead to cytoskeletal structural disruption. This direct toxicity effect impairs the adhesion of cells to one another, which in turn causes a significant loss of intravascular fluid and consequent peripheral edema. Clinically, many infections present with a TSS-like presentation, which is caused by intravascular depletion. 8 A French case series found 15 non-fatal P. sordellii foot infections despite a high mortality rate; all isolates lacked the TscL gene. 9 A favorable outcome and lack of TSS-like presentation in these cases are probably explained by the absence of TscL. The documented survival of a patient with bacteremia and cholangitis in a case of a TscL gene negative infection provided additional evidence that the presence of the TscL gene leads to increased pathogenicity. 10
A number of factors, including the site and nature of infection, immunocompromised state, and antimicrobial resistance, are significant in determining the overall prognosis in addition to the presence of TcsL. An analysis of recent research suggests that infections linked to intravenous drug misuse have comparable mortality rates, despite the historical notion that gynecological infections had the highest rate. 2 Early treatment with culture-sensitive antibiotics appears to be key elements in better outcomes for non-lethal infections with TcsL-positive P. sordellii. 8
Research on antibiotic resistance to date indicates that many species are susceptible to penicillins, metronidazole, and clindamycin.1,3 Treatment for septic shock should involve early initiation of broad-spectrum antibiotics, hemodynamic support with vasopressors if necessary, and aggressive therapy with volume resuscitation.
Unfortunately, for a comprehensive pathological assessment, the TcsL assay was unavailable in our laboratory. Since, our patient got better with surgical debridement and symptomatic management, other methods of assessment were not pursued as it was not likely to impact clinical management.
In our case, the patient was a laborer and was regularly involved in digging at construction sites with frequent contact with soil. Though, patient’s clinical history suggested that he encountered minor injuries on 2 separate occasions, the nature and depth of the resulting wounds could not be ascertained as the patient cannot recall the exact details during history taking and also there were no visible wounds on the lower legs during physical examination. The authors hypothesize that P. sordelli spores might have been introduced at the infection site as a result of traumatic inoculation during manual labor work. With subsequent maturation, the organism elaborated an array of virulence factors allowing it to burrow deep in to the soft tissue ultimately leading to osteomyelitis.
Conclusion
We presented a rare case of osteomyelitis caused by P. sordelli in a young male patient, which according to the best of our knowledge is the first reported case of P. sordelli from Pakistan. Since, it is rare and highly fatal in most cases, prompt reporting and insights from treated infections could pave the way for successful management.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MK – Bench work and Writing – Original draft. SSK – Bench work and Writing – Review and editing. SZ – Writing – Review and editing.
Consent
Informed consent was obtained from the patient regarding publication of the case.