
Abstract
Background:
Cerebral infarct associated with varicella-zoster virus (VZV) has been reported in the literature, while isolated central dizziness due to lateral medullary infarct (LMI) following VZV infection is rarely reported.
Case report:
We report the case of a 65-year-old man who presented to the neurology department because of herpes zoster on the right trigeminal nerve distribution. At 12 hours after admission, he developed transient vertigo along with nausea and unsteady walking and left-sided spontaneous horizontal nystagmus, gaze-evoked nystagmus, and upbeat nystagmus. The other usual signs of LMI including Horner syndrome, dysarthria, swallowing difficulty, and hemibody sensory change were absent. Video head impulse indicated decreased head impulse gain of the vestibulo-ocular reflex for the bilateral horizontal, anterior, and posterior semicircular canals with abnormal saccade waves. Suppression head impulse paradigm showed few downward saccades reflecting anti-compensatory saccades after the end of the head impulse back to the head-fixed target and decreased vestibulo-ocular reflex gain values of bilateral semicircular canals. Brain magnetic resonance imaging (MRI) showed a small infarct in the far dorsolateral portion of the left rostral medulla. The cerebrospinal fluid was positive for VZV DNA.
Conclusions:
In patients with VZV infection who develop dizziness, the possibility of cerebral infarct should be considered. Patients with facial herpes zoster and neurological symptoms always be screened for stroke using MRI and lumbar puncture should be performed and acyclovir administered empirically.
Keywords
Introduction
Herpes zoster is a reactivated VZV infection. Initial infection with VZV is manifested as a varicella or latent infection, and the virus lingers in the dorsal root ganglion of the spinal cord. As the function of the immune system decreases, the virus is reactivated, leading to herpes zoster. Herpes zoster is thought to rarely cause cerebral infarcts. However, in recent decades, herpes-induced vasculitis, and stroke have been increasingly reported after the reactivation of VZV. 1 Cerebral infarct associated with varicella-zoster virus (VZV) has been reported in the literature. 2 In this paper, we present a rare case of isolated transient central dizziness due to a lateral medullary infarct (LMI) following VZV infection.
Case Report
The paper reports the case of a 65-year-old man who presented right upper orbital pain, persistent throbbing pain, herpes on the forehead, and ocular redness without obvious cause. The symptoms improved with over-the-counter oral pain medication. Four days later, the herpes range and degree of pain worsened, resulting in the patient being hospitalized. The patient is thin and vegetarian with no disease history of diabetes or hypertension and no alcohol intake or tobacco use. The patient showed paresthesia allodynia and painful vesicles on the right trigeminal distribution (V1); no other abnormalities were observed upon physical examination at admission. The general physical examination results were as follows: body temperature, 36.5°C; pulse, 83 beats/minutes; respiration, 19 beats/minutes; systolic blood pressure, 109 mmHg; and diastolic blood pressure, 78 mmHg. Thoracic CT scan, electrocardiogram, and laboratory investigations including complete blood count, biochemistry (renal/liver function, electrolytes, uric acid, and lipids) were normal. The patient was admitted on intravenous antiviral therapy with acyclovir along with Pregabalin capsules (150 mg/day)for neuralgia control.
At 12 hours after admission, the patient experienced dizziness unrelated to postural changes along with nausea and unsteady walking. No other local neurological signs including headache or neck pain, photophobia, phonophobia, auditory symptoms, weakness and numbness of the limbs, diplopia, dysarthria, dysphagia, or ataxia were found. At first, the herpes virus was thought to have invaded the peripheral vestibular nerve. The bedside video nystagmus recording showed left-sided spontaneous horizontal nystagmus, gaze-evoked nystagmus, and upbeat nystagmus. Video head impulse (vHIT) showed that the gain values of the 6 semicircular canals on bilateral sides were reduced, and abnormal saccade waves were observed. Notably, suppression head impulse paradigm (SHIMP) further confirmed the decreases in the gain values of the bilateral semicircular canals (Figure 1). Temperature test and VEMP are normal. The nystagmus signs (gaze-evoked nystagmus, and upbeat nystagmus) indicated that the isolated vertigo might be caused by central lesions; thus, lumbar puncture (2022-01-13) was performed. Cerebrospinal fluid biochemistry (2022-01-13 13:46) indicated a trace total protein content of 752 mg/L. Cerebrospinal fluid routine (2022-01-13 12:03) indicated a white blood cell count of 4 × 106/L with clear fluid and increased lymphocyte ratio. These results suggest the presence of viral encephalitis. Meanwhile, head MR was performed, indicating left medulla oblongata DWI high signal, low ADC signal (Figure 2), and no obvious abnormality on MRA. According to these imaging findings, the patient was considered to have left medulla infarction.
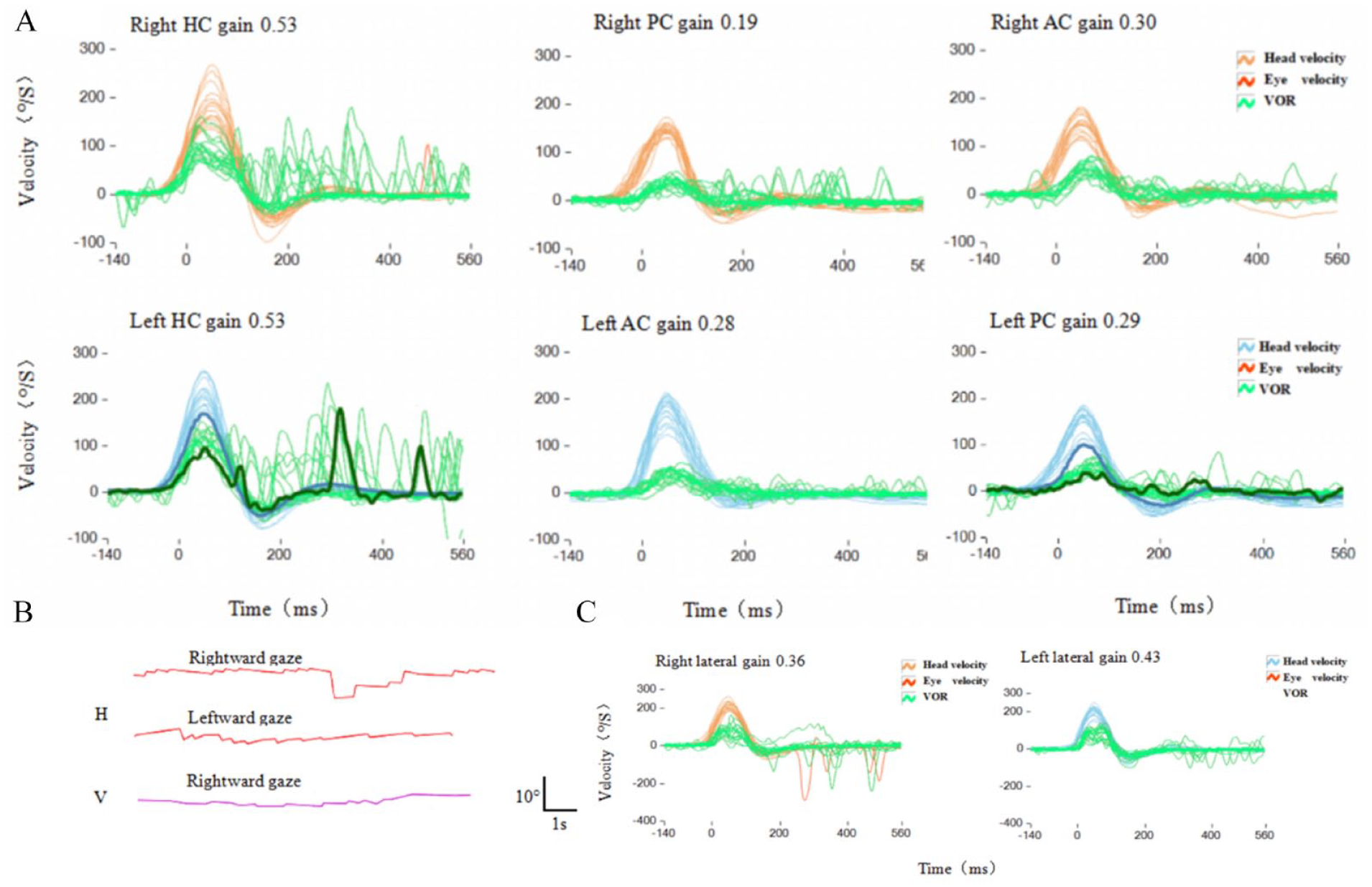
(A) During vHIT (2022-01-13 19:20), shows decreased abnormal saccade waves and head impulse gain of the vestibulo-ocular reflex for the horizontal, anterior, and posterior semicircular canals. (B) Figure shows bilateral gaze-evoked nystagmus and upbeat nystagmus. (C) During SHIMP (2022-01-13 19:25), shows only very few downward saccades reflecting anti-compensatory saccades after the end of the head impulse back to the head-fixed target and decreased vestibulo-ocular reflex gain values of the bilateral semicircular canals.

Fiugre shows left medulla oblongata DWI high signal (A), low ADC signal (B).
The next morning, the dizziness subsided, and neurological tests revealed no obvious local symptoms. The patient was then treated with antiviral therapy(acyclovir 500 mg every 8 hours for 14 days), neurotrophic therapy, antiplatelet aggregation (aspirin 100 mg/day, patients stop the drug on their own after 14 days), lipid regulation, and plaque stabilization. Nine days after the above treatment, the total protein content in the cerebrospinal fluid was determined as 557 mg/L. The cerebrospinal fluid was also positive for VZV DNA, indicating that the virus had invaded the brain. 4
Discussion
Epidemiology
Herpes zoster infection increases the risk of stroke. A study by the National Institutes of Health in Taiwan showed a 30% increased risk of stroke within 1 year after zoster infection. A Danish study showed a 126% increase in stroke risk within 2 weeks after zoster infection, a 17% increase within 2 weeks to 1 year after infection, and a 5% increase within 1 year after infection. Importantly, according to the UK Health Improvement General Practice Database, 3 zoster infection increases the risk of transient ischemic attacks by 1.15 times and the risk of myocardial infarction by 1.10 times.
Diagnosis
VZV infection of cerebral arteries is a cause of ischemic and hemorrhagic stroke. Patients with a recent history of herpes zoster, transient ischemic attack, stroke, chronic headache, or altered consciousness should be suspected of VZV vascular disease. Supporting diagnoses include mononucleosis in cerebrospinal fluid and MRI showing ischemic or hemorrhagic lesions. Detection of anti-VZV IgG antibodies is the best diagnostic method because although viral DNA can be detected by polymerase chain reaction (PCR) in early stages of the disease, there is an average delay of 4.2 months from herpes zoster to neurological symptoms and signs, and VZV DNA is frequently absent in cerebrospinal fluid. Importantly, the diagnosis of this treatable cause of stroke is often overlooked because one-third of patients with virologically-confirmed VZV vascular disease did not have a previous rash. 4
In this case, the ischemic stroke was related to herpes zoster for the following reasons: (1) Caloric test and VEMP test was normal, without facial paralysis, earache, hearing impairment, which can eliminate Ramsay-Hunt syndrome and other peripheral vestibular diseases; (2) the presence of VZV DNA in the cerebrospinal fluid along with the high white blood cell count and protein level in the cerebrospinal fluid indicate the presence of VZV infection, but was without meningeal irritation sign,viral meningoencephalitis can be ruled out; (3) and the cranial MRI features indicate medullary infarction,without others abnormality and excluded inner ear disease, intracranial space occupying lesion and demyelinating lesion. At present, the following mechanism is the most likely: herpes zoster directly infects the cerebral arteries and venous sinuses from the cranial and peripheral nerve ganglia via axons, leading to inflammatory and non-inflammatory changes including thrombosis, necrosis of the vascular wall, dissection, and aneurysmal disease, leading to cerebrovascular diseases. 5
Since the disease progressed to vertigo after VZV infection, Ramsay-Hunt syndrome, for which peripheral vertigo is a symptom, was first considered in the clinic. The unique aspect of this case is that the physical examination of the patient showed central vertigo, and vertigo and the related neuro-otological signs lasted only more than 10 hours, which may be related to the small cerebral infarct lesion. Notably, the above condition is easily misdiagnosed or missed clinically. Moreover, the eye movement, vHIT, and SHIMP characteristics of the patient were recorded in this case, which is not typical in patients with post-herpes zoster infarcts. The patient also presented with gaze-evoked nystagmus and upbeat nystagmus. When eccentric gaze is used under normal conditions, tonic extraocular muscle contraction is necessary to overcome the elastic strength of orbital contents and maintain the stability of the eyeball. Tonic extraocular muscle contraction requires that the cerebellar flocculus, paraflocculus, and medial vestibular nucleus (MVN)-nucleus prepositus hypoglossi (NPH) control the neural integration center consisting of the implanted nucleus. The MVN-NPH integrate the horizontal velocity signals of eye movement and convert them into a position signal, a continuous positional voltage signal maintains the eyeball in the eccentric position. The flocculus and paraflocculus mediate the correction of speed and location signals in the eyeball. 6 Upbeat nystagmus (UBN) is considered to be associated with basal ventrolateral, dorsal pons, or caudal medulla injuries. We speculate that it may be related to the previa of the NPH underlying nucleus intercalatus and the nucleus of roller (NR) injury. When the NR itself or the surrounding area is damaged, the medulla oblongata NR-flocculus inhibitory tract is blocked. The loss of inhibition of the flocculus leads to the overexcitation of the inhibitory flocculus-vestibular tract, which leads to the over-inhibition of the entire downstream pathway and results in UBN. 7 Therefore, the lesions in this patient were considered to invade MVN-NPH and related areas to elicit the aforementioned symptoms. In contrast to peripheral vestibular lesions, in unilateral vestibule nuclei lesions, the gain of the head impulse vestibulo-ocular reflex (VOR) can be reduced in both directions, which may be an adaptive mechanism to reduce the contralateral VOR gain. Notably, it is possibly caused by the action of inhibitory interneurons in the vestibulum. 8
Treatment
The appropriate treatment for VZV vasculitis is still unclear and has not been extensively discussed. Generally, patients with VZV vasculitis receive 10 to 15 mg/kg intravenous acyclovir for 14 days of treatment. According to the hypothesis of the pathogenesis of inflammation, prednisone is usually given at a dose of 1 mg/kg body weight 5 days before the 14-day acyclovir course of treatment. 9 But David G Partridge’s authors’ opinion is that treatment of zoster aims to reduce the severity of acute symptoms, but more importantly to prevent the development of complications, especially post-herpetic neuralgia in elderly patients and eye damage from trigeminal shingles. Over the past 30 years, several studies have shown that acyclovir, if given within 72 hours of rash onset, is superior to placebo in rash healing rates, reduces acute zoeter-related pain, and reduces viral shedding and returns to normal activity; Topical corticosteroids can be used as adjunctive therapy when herpes zoster ophthalmia is complicated by ocular inflammation, and systemic steroids can be used when VZV reactivation is accompanied by motor weakness, the latter is not conclusive evidence. 10 Our patient has small lesions and short duration of symptoms, considering the side effects of glucocorticoids, hormone therapy has not been given. The role of antiviral combination corticosteroids or antiplatelet drugs and antiviral therapy alone in the risk of stroke associated with varicella zoster is not clear and needs to be studied in large-scale clinical trials. It is not recommended to use corticosteroids without antiviral therapy. 11
Prognosis
The results of a meta-analysis published by Lu et al in 2023 showed that the risk of stroke increased after VZV infection, and the risk of stroke was highest within 14 days and lasted for 1 year. The prognosis of most patients is better, and the frequency of continuous vascular progress is lower. 11
Conclusion
In conclusion, we have reported a case of herpes zoster medullary infarction with isolated vertigo with transient nystagmus without other symptoms of neurological deficit. Detailed vHIT and SHIMP recordings were made of the patient’s nystagmus; these recordings have rarely been reported. The patient’s isolated central vertigo may have been caused by a VZV infection-triggered stroke. VZV infection may increase stroke risk, and the mechanism is considered to be the direct invasion of blood vessels, leading to stenosis or embolization of the vascular wall. Therefore, the treatment is antiviral therapy and antithrombotic or antiplatelet therapy combined with stroke mechanistic therapy.
Footnotes
Acknowledgements
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of China (No. 82104155), Key Research and Development Program of Shaanxi (2020ZDLSF04-03 and 2021SF-096), and Xi’an Science and Technology Planning Project (21YXYY0038, 21YXYJ0035, and 21YXYJ0004).
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contribution
Ning Zhao: concept, image interpretation, and writeup of manuscript. Yong Zhao: image interpretation and preparation. Gejuan Zhang: image interpretation and preparation. Mingze Chang: critical revision for intellectual content. Other authors contributed to the revision and refinement of the article, ensuring clarity, coherence, and accuracy of the article. We would like to thank each author for their professionalism, hard work, and valuable contributions to this article.
Ethical Approval
Written informed consent was collected from the patient for the anonymized publication of this report.