
Abstract
Background:
Kartagener’s syndrome, a rare autosomal recessive genetic disorder, is characterized by primary ciliary dyskinesia (PCD), resulting in defective cilia function in the respiratory tract and fallopian tubes.
Case presentation:
This case report discusses a 23-year-old female with Kartagener’s syndrome, bronchiectasis, and cardiac involvement, who presented with shortness of breath, cough, and syncope. Notably, she received home oxygen therapy but became exhausted, leading to loss of consciousness. Clinical examination revealed prominent heart sounds and abnormal lung findings. Laboratory results indicated leukocytosis, and an ECG confirmed dextrocardia and cardiac abnormalities. Doppler studies identified mitral and tricuspid regurgitation along with severe pulmonary arterial hypertension. Antibiotics were administered for coagulase-negative Staphylococcus infection. The patient improved with a treatment regimen, including oxygenation and nebulization. Regular follow-up and patient education were emphasized.
Conclusion:
This case underscores the complexity of Kartagener’s syndrome and the importance of a multidisciplinary approach in managing its respiratory and cardiac manifestations.
Keywords
Introduction
A rare ciliopathic, autosomal recessive genetic condition known as Kartagener’s syndrome is characterized by a “clinical triad” of chronic sinusitis, bronchiectasis, and situs inverses syndrome. 1 Kartagener’s syndrome results due to primary ciliary dyskinesia (PCD) which causes a defect in the action of the cilia lining the respiratory tract and fallopian tube. 2 An estimated 1 in 30,000 live births are affected by it and both males and females are equally impacted. 3 It results in progressive symptoms such a productive cough, wheezing, and shortness of breath. It also increases the susceptibility of the respiratory system to infection. 4 Bronchiectasis can progress to end-stage lung failure, and lung transplantation might be the only effective treatment. 5 Cardiovascular involvement is characterized by situs inversus (Kartagener’s syndrome in PCD) and other congenital cardiovascular abnormalities, such as bilateral superior vena cava, inferior vena cava drainage site abnormality, Tetralogy of Fallot, transposition of the great arteries, aortic coarctation, subpulmonic stenosis, atrial isomerism, atrial septal defect, common atrium, atrioventricular septal defect.6,7 Here in we presented a case of 23-years old women with known case of Kartagener’s syndrome complicated by bronchiectasis with tricuspid and mitral valve regurgitation.
Case Presentation
A 23-year-old non-smoker female known case of bronchiectasis, asthma and situs inversus presented to the outpatient department with complain of SOB, dyspnea and cough for 1 day. The patient experienced SOB on lying down with productive cough containing sputum. The sputum was green in color, copious in amount, progressive in nature and sticky in consistency associated with chest pain and difficulty in breathing. There were no associated symptoms of fever and hemoptysis. No history of nausea vomiting and diarrhea. O2 therapy was also given at home via nasal cannula (2 L per minute) but she became so exhausted that she lost consciousness due to excessive respiratory effort.
On arriving hospital, her vital signs were: RR 45 per min, Blood pressure 100/60, Oxygen saturation 68% on 5 L of oxygen, Temperature was 98 F. These findings underscore the severity of her respiratory compromise. General examination revealed no remarkable findings. Cardiovascular examination showed that the apex beat was prominent in the left fifth intercostal space 1 cm lateral to the midclavicular line. On auscultation, bilateral coarse crackles with rhonchi were heard upon inspiration. Heart sounds were more pronounced at the right sternal border.
Complete blood workup was performed. Her laboratory work-up was unremarkable except for mild leukocytosis. The details are provided in Table 1. PT, INR and electrolytes were normal. An ECG was also performed demonstrated in Figure 1, which showed dextrocardia, dilation of right ventricle while other chambers were normal in dimension. Depressed LV systolic function was interpreted while the size of LV was normal. No significant segmental wall motion abnormality was noted. There was no left ventricle hypertrophy seen. Normal RV function. No clot and no vegetation seen. No pericardial effusion seen. No intra cardiac shunt seen. Doppler studies showed mitral regurgitation and tricuspid regurgitation with severe Pulmonary Arterial Hypertension (PAH). CT findings Figure 2, computed tomography of the lung demonstrated severe bilateral basilar bronchial wall thickening and bronchiectasis. Bronchiectasis were varicose and cystic with intrinsic air-fluid levels. Situs inversus totalis was confirmed with a tri-lobed left lung, a bi-lobed right lung, dextrocardia, right-sided spleen and left-sided liver. History, clinical signs, and imaging studies proved the diagnosis of Kartagener’s syndrome.
Complete blood workup.

Abbreviation: HCT, hematocrit; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; RBC, red blood cells; WBC count, white blood cells count; INR, international normalized ratio.

ECHO (Echocardiogram).
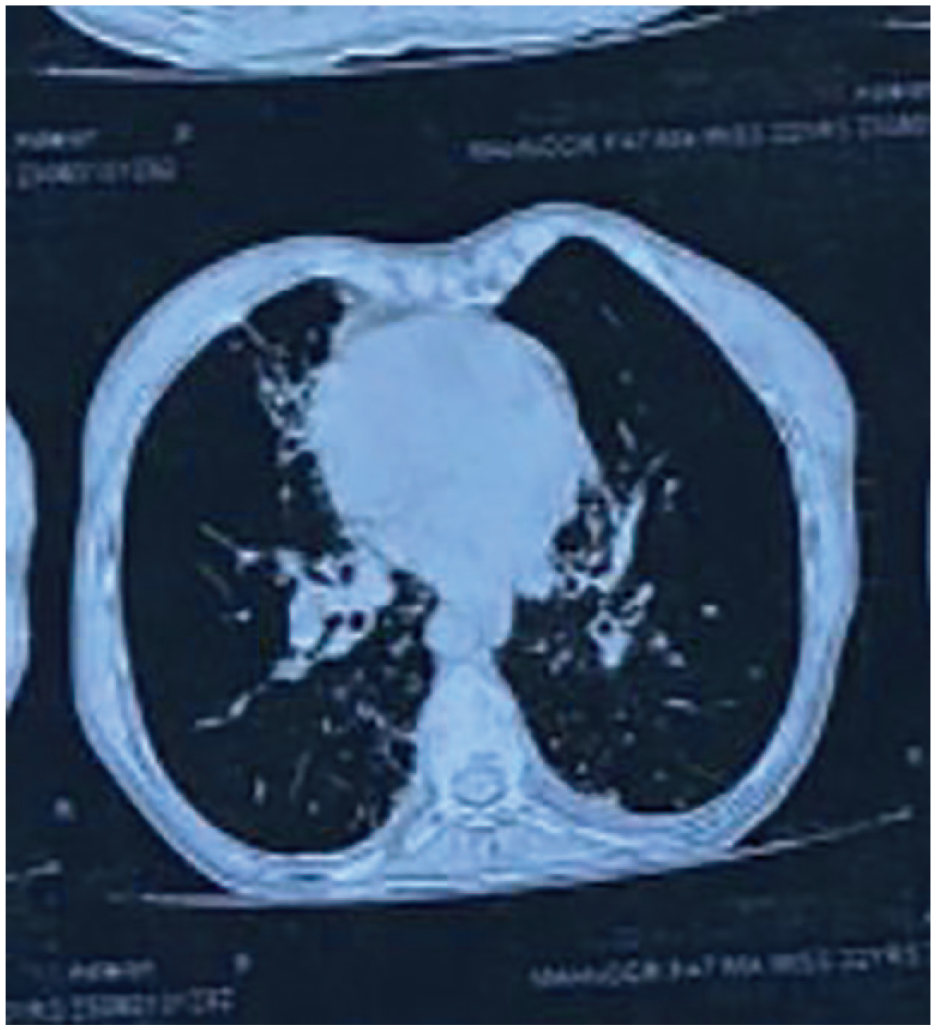
CT (Computed Tomography of chest).
Patient was positive was for coagulase negative staphylococcus species on culture for which antibiotics were advised. She was treated with piperacillin and tazobactam, azithromycin and gentamycin. Further regimen of oxygenation and nebulization with hypertonic solution were planned for her. Patient followed up a week later with improvement in symptoms. The nature of her disease and importance of regular follow-up was explained to patient.
Discussion
To our knowledge, this is the first case report of simultaneous occurrence of Kartagener’s syndrome complicated by bronchiectasis with tricuspid and mitral valve regurgitation in an adolescent patient. Ciliary motility disorders can be inherited or acquired. Normal ciliary function is critical for respiratory tract host defense, sperm motility, and normal visceral orientation during embryogenesis. Recurrent bronchitis, pneumonia, and sinusitis are the 3 clinical symptoms that occur most frequently. In 50% of those with dyskinetic cilia syndrome, situs inversus is present. 8 The condition known as Kartagener syndrome occurs when situs inversus, chronic sinusitis, and bronchiectasis co-occur. 2
Though the majority of individuals exhibit symptoms from birth or infancy, but the diagnosis is often delayed. Lack of diagnosis results in bronchiectasis that leads to progressive and permanent lung destruction owing to obstruction of the airways with secretions and subsequent infection.9,10 Our patient reported symptoms of shortness of breath (SOB), dyspnea, and a productive cough, which is typical for patients with Kartagener’s syndrome. The presence of chest pain and difficulty breathing is alarming and indicates the severity of her condition.
Defects in left-right lateralization, such as situs solitus (dextrocardia only) or situs inversus totalis, where thoracic and abdominal organs are observed transposed, are caused by impaired ciliary motion during development. 11
Imaging findings revealed bronchiectasis, dextrocardia, and situs inversus, which met the diagnostic criteria for KS in our patient. Treatment of Kartagener syndrome includes daily chest physiotherapy, antibiotics with good pseudomonal coverage, and supportive pulmonary care. 2
Conclusions
This case underscores the complex nature of Kartagener’s syndrome, a rare genetic disorder affecting ciliary function and leading to severe respiratory and cardiac complications. In this particular patient, the combination of bronchiectasis and valvular regurgitation contributed to significant respiratory distress and severe PAH. Effective management includes a multidisciplinary approach, with a focus on treating respiratory infections, addressing cardiac issues, and providing patient education on the importance of regular follow-up. It is crucial to tailor treatment plans to the individual patient’s needs and to monitor their progress over time. This case report adds to our understanding of the challenges faced by individuals with Kartagener’s syndrome and highlights the potential for successful management and improved quality of life with appropriate care and intervention.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent Statement
The patient gave informed consent and patient anonymity was preserved.