
Abstract
Hirschsprung’s disease is a congenital disorder characterized by the absence of nerve cells in the colon muscles, leading to difficulties in evacuating stool. This case report describes a newborn patient presenting with typical symptoms of the disease, including abdominal distension, constipation, diarrhea, and fever. The patient’s initial laboratory investigations revealed anemia (Hb: 9.80 g/dL), low RBC count (3.50 million/cu mm), elevated RDW (16.70%), increased WBC count (11 000/cu mm), and raised platelet levels (891 000/µL) along with an elevated CRP (3.22). The baby received a comprehensive treatment regimen, including blood transfusion, Syp. MVBC, Enterogermina, Inj. Pan, Inj. Metro, Inj. Piptaz, Inj. Vancomycin, Calcium gluconate, and Inj. Aminoven. Following this treatment and necessary surgical intervention, the patient demonstrated significant improvement in frequent bowel movements and alleviation of other symptoms. This case highlights the importance of prompt diagnosis and multidisciplinary management for favorable outcomes in infants with Hirschsprung’s disease.
Background
In 1886, Harald Hirschsprung identified Hirschsprung disease (HSCR) in older children. 1 Hirschsprung disease (HRSD), also known as aganglionic megacolon, is characterized by a deficiency of intrinsic ganglion cells in the myenteric (Auerbach) and submucosal (Meissner) plexuses of the gastrointestinal tract. Constipation and enterocolitis are common side effects, causing a functional obstruction of the colon. 2 Approximately 1 in 5000 live babies are thought to be affected by HRSD,3,4 with a higher prevalence among boys, often reported as 4:1.2,5 It is a congenital condition associated with various heritable conditions, including trisomy 21, single gene mutations, syndromes, and inflammatory bowel disease.2,6
Symptoms may range from neonatal intestinal blockage to chronic, increasing constipation in older children. In the first few months of life, over 80% of patients exhibit growing abdominal distention, poor feeding, and problematic bowel movements. Hirschsprung’s illness affects up to 90% of newborns who are unable to pass meconium within the first 24 hours of life.4,7 Medical professionals diagnose Hirschsprung disease by combining imaging studies, anorectal manometry, and rectal biopsies. Doctors frequently employ rectal biopsies to confirm or disprove a Hirschsprung disease diagnosis.8,9 Hirschsprung’s illness is typically treated surgically by removing or bypassing the section of the intestine lacking nerve cells. Two procedures can be used to accomplish this: pull-through surgery and ostomy surgery. 10
During a pull-through procedure, the lining of the colon’s diseased portion is removed, and the typical part is then connected to the anus after being drawn through the colon from the inside. In the ostomy surgical procedure, the upper, healthy piece of the colon is attached to a hole the surgeon makes in the child’s belly after the aberrant portion of the colon is first removed. Stool subsequently exits the body through the incision in the abdomen, collected in a bag attached to the end of the intestine (stoma). This allows the colon’s lower portion time to recover. A second treatment is performed to close the stoma and join the healthy section of the intestine to the rectum or anus once the colon has had time to recover. Patients with serious illnesses often require ostomies. 10
In this study, we will discuss a rare instance of Hirschsprung’s illness in a female infant that was successfully identified and treated within the first few months of life to prevent life-threatening consequences.
Case Presentation
A 4-month-old female infant from Pune, Maharashtra, weighing 5.9 kg and measuring 63 cm in height, presented with a history of not passing stool within the first 24 hours after delivery. Following the administration of a suppository, she eventually passed stool. However, after 15 days, her mother observed abdominal distention and difficulty in passing stool. Hirschsprung’s disease was subsequently diagnosed through abdominal X-ray (Figure 1), colon X-ray (Figure 2), ultrasound (USG), and rectal biopsy.

Simple abdominal X-ray showing diffuse air distention of bowel loops.

Barium colon enema showing swollen colon with shrunken rectum.
To address the stool passage issue, a colostomy was performed. The patient’s family history was unremarkable. Following the initial colostomy, the infant was readmitted to the hospital on February 10, 2023, after 3.5 months, for additional surgical procedures. The decision to postpone the pull-through surgery post-colostomy was motivated by the intention to allow the infant adequate time for growth. This strategy aims to better prepare the child for the subsequent, more intricate pull-through surgery and to minimize the associated surgical risks.
During the physical examination, the infant exhibited weakness, noncooperation, and abdominal distension, while her vital signs remained within normal limits.
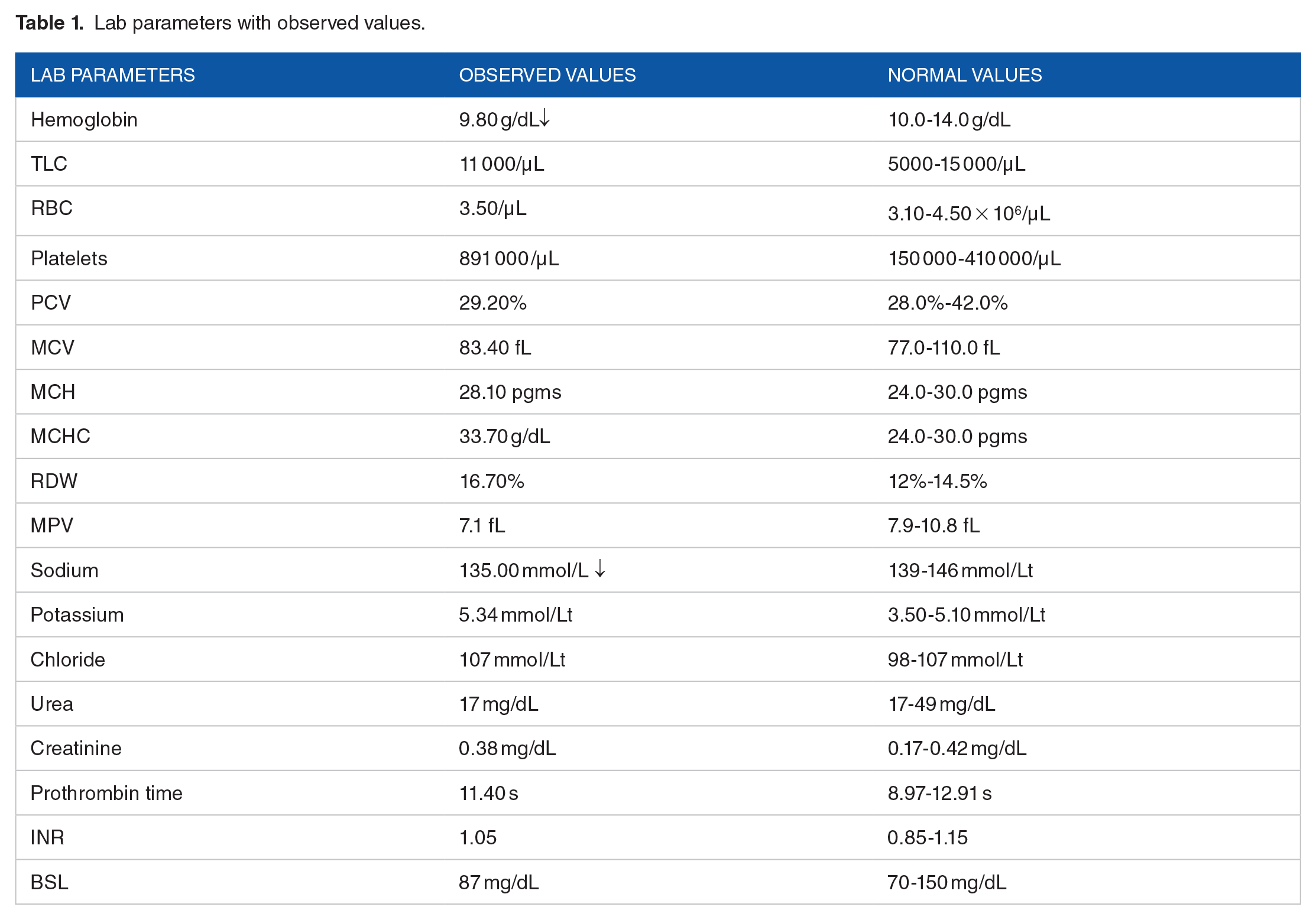
Clinical examination revealed the following laboratory parameters (refer to Table 1):
Lab parameters with observed values.
The histopathologic report indicated the absence of ganglionic cells. On February 18, 2023, the patient reported experiencing 9 to 10 episodes of greenish-yellowish-colored diarrhea, which was successfully treated with Enterogermina and ORS sachet.
On February 21, 2023, the patient underwent a successful pull-through surgery, spending 2 days in the PICU. Before the surgery, the patient received the necessary supplements, including TAB. MVBC and TAB. CALPOL. Post-surgery, a 10-day course of antibiotics, vitamins, and symptomatic care was administered (as shown in Table 1). Additionally, the patient reported 9 to 10 episodes of greenish-yellowish diarrhea on February 18, 2023, which was successfully treated with Enterogermina and an ORS sachet.
Following the successful surgical treatment, the infant demonstrated ease in passing stool, exhibited a happy expression, and enjoyed restful sleep (Figure 3).

Baby after the pull through surgery.
Throughout the treatment, the patient received various medications listed in Table 2:
Drugs with dose prescribed throughout the treatment.

Discussion
Hirschsprung disease, initially documented by Harald Hirschsprung in 1886, is characterized by the absence of submucosal and myenteric ganglionic cells in the colon. 11 A crucial indicator for urgent specialist referral is the delayed passage of meconium beyond 48 hours in term infants, particularly as the condition often presents with a failure to pass meconium within the first 24 hours after birth. Common signs in infants include abdominal distention, bilious vomiting, poor feeding, and persistent constipation. 12
While a barium enema serves as a diagnostic tool for detecting symptoms of Hirschsprung’s disease, its reliability as a sole diagnostic method varies. Further research is necessary to assess its accuracy, particularly in resource-limited settings, and compare it with alternative approaches. 13 Intra-operative biopsy and frozen section are recommended for precise identification of aganglionosis, with rectal biopsy remaining essential for disease confirmation. 14 Acetylcholinesterase (AChE) expression plays a critical role in diagnosing Hirschsprung disease by confirming the presence of hypertrophied nerve fibers through histochemical reaction detection of acetylcholinesterase activity. 15
Surgical treatment options, including Swenson, Duhamel, and Soave endorectal pull-through procedures, as well as trans-anal and laparoscopic techniques, demonstrate comparable short-term outcomes with benefits such as minimal analgesia and reduced hospital stays. 16 Postoperative care, following the ERAS protocol, prioritizes pain management, infection control, and nutritional supplements to expedite patient recovery. 17
Early diagnosis of Hirschsprung disease is imperative as late-diagnosed patients face increased susceptibility to complications such as hemorrhage, incontinence, and enterocolitis-related mortality. Late diagnosis may complicate colostomy surgeries, leading to issues like prolapse and hernia, along with developmental delays and a higher prevalence of comorbidities. 18 Therefore, risk indicators, like failure to pass meconium within 48 hours of delivery, should be carefully considered. 19
In our case, Hirschsprung’s disease was identified 15 days after birth through abdominal X-ray, colon X-ray (barium enema), USG, and rectal biopsy for confirmation. The histopathologic report confirmed the absence of ganglionic cells. A pull-through operation was conducted, revealing post-surgery anemia, an increased platelet count, and hypokalemia—a common complication of major abdominal surgery. 20
Conclusion
Hirschsprung’s Disease is a rare illness that, if not diagnosed correctly in neonatal life, has the potential to be harmful and fatal. Hirschsprung’s illness occurs uncommonly and infrequently in newborns, making an early diagnosis difficult and even fatal. Physicians must be able to recognize the disease’s characteristic symptoms, which include an enlarged abdomen and the absence of meconium during the first 48 hours after birth. Surgeons can now make definitive repairs at younger ages than in the past due to advancements in the diagnosis of Hirschsprung’s Disease and newborn critical care. With reports of positive results, neonatal primary pull-through operations have grown in popularity. Despite the majority of children having successful outcomes, a close and prolonged follow-up is advised for the early discovery and management of problems.
To avoid any delays in the diagnosis and treatment, we, therefore, expect that this article will enable pediatricians to consider Hirschsprung’s Disease as a potential diagnosis in cases of intestinal blockage.
Footnotes
Acknowledgements
The authors acknowledge all the medical and nursing team that provided an excellent care
Author Contributions
PP and AV was responsible for the conception of this article, patient care, case analysis, and manuscript writing. KR, PP and AV were responsible for patient care and manuscript revision.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Not applicable.
Informed Consent/Patient Consent
I hereby declare that parental consent was obtained before publishing this case report.
Trial Registration Number/Date
Not applicable.
Other Journal Specific Statements as Applicable
Not applicable.
Data Availability Statement
Not applicable.