
Abstract
Background:
Bardet-Biedl syndrome (BBS) also known as Laurence-Moon-Bardet-Biedl syndrome one of the rarely reported genetic disorder characterized by an intellectual disability, limb, kidney abnormalities, obesity, and Rod-cone dystrophy. Other associated condition includes diabetes mellitus, hypertension, hypogonadism, facial dysmorphism, and congenital heart defects. This case highlights megaloblastic anemia associated with BBS.
Case presentation:
A 16-year-old female patient who had a moon face, truncal obesity, polydactyly, low IQ, and visual impairment presented with the complaint of shortness of breath and easy fatiguability. She had bilateral retinal pigmentosa in her eyes and her laboratory evaluation and bone marrow biopsy revealed megaloblastic anemia secondary to vitamin B12 deficiency. She received injectable vitamin B12, folate, and red cell contrate transfusion. Her symptoms improved and she was discharged with oral medication.
Conclusion:
Megaloblastic anemia in BBS is rarely reported, further research is needed to find the exact cause that is necessary for proper management and better outcome.
Introduction
Bardet-Biedl syndrome (BBS) also known as Laurence-Moon-Bardet-Biedl syndrome is an autosomal recessive inherited condition characterized by impaired cognition, limbs deformities, visual impairment due to rods and cones dystrophy, and urogenital abnormalities. The incidence rate varies from 1:140 000 to 1:160 000 live births in North America and Europe. 1 Conversely, in Kuwait and Newfoundland, the rate is much greater, with an estimated frequency of 1:13 500 and 1:17 500, respectively. 1 According to recent studies, 18 genes are involved in the pathogenesis of BBS. These are named as BBS genes that is, BBS1, BBS2, BBS3/BBS4, BBS5, BBS6, BBS7, BBS8, BBS9, BBS10, and BBS11. These genes produce proteins called BBS proteins, that are responsible for 80% of that mutation. 2 The BBS proteins are involved in ciliary dysfunction, disruption of the chemical signaling pathways that are active throughout the developmental process, and sensual perception.3,4 Other conditions associated with BBS include diabetes mellitus, hypertension, congenital heart disease, facial dimorphism, speech problems, dental deformities, and liver failure. 4
The clinical presentation consists of night blindness which is a symptom of visual impairment that is, retinal dystrophy featuring photoreceptors with unusual pigmentary dystrophy and early macular involvement. Limb involvement occurs in about 70% of cases and includes postaxial polydactyly, brachydactyly, partial syndactyly, clinodactyly, and sandal-gap. Hypogonadism or small external genitalias especially in male patients occurs in 90% of the cases and females present with ambiguous genitalia. Decreased IQ is a significant trait (86%), but mental retardation is a contentious aspect. In 5% of people with chronic renal failure, renal dysplasia can exist without clinical signs of renal illness. 5 Very little is known about megaloblastic anemia in BBS, thus this case report highlighted the co-existence of megaloblastic anemia in patients with BBS.
Case Report
A 16-year-old female patient presented to the outpatient department of a tertiary care hospital with 6 months history of dyspnea on exertion and easy fatiguability. The dyspnea was gradual in onset and was relieved with rest. On further inquiry, there was no cough, fever, chest pain, orthopnea, or paroxysmal nocturnal dyspnea (PND). She does not have any history of epigastric discomfort, Malena, or previous history of hepatitis B or C infection. She was taking a balanced diet and there was no history of body aches, numbness, or tingling sensation in the body. Her medical history was significant for recurrent otitis media, frequent falls at night, and the need for support for walking during the night. There was no history of gastrointestinal surgery or food allergy. The patient was born at term through normal vaginal delivery as a result of consanguineous marriage, and there was no family history of a similar condition. The patient did not attain menarche or pubarche.
On examination, she was active with a height of 150 cm and weight of 74 kg having a body mass index (BMI) of 32.8 kg/m2. She had a pale conjunctiva and vital signs of blood pressure of 110/80 mm of Hg, pulse rate of 88 beats per minute, respiratory rate of 17 breaths per minute and there was no postural drop. She had a moon face, high arched palate, truncal obesity flat feet, and polydactyly as shown in Figure 1.

showing the clinical features of Bardet-Biedl syndrome (A) moon face, (B) polydactyly of the right hand and left feet (C).
The rest of the clinical examination and assessment was normal except for mild cognitive impairment having a mini-mental state examination (MMSE) score of 19/30.
An ophthalmological and audiological evaluation was requested and the fundoscopy revealed bony spicules suggestive of retinitis pigmentosa in both eyes as shown in Figure 2. Ear examination revealed bilateral tympanic membrane perforation.
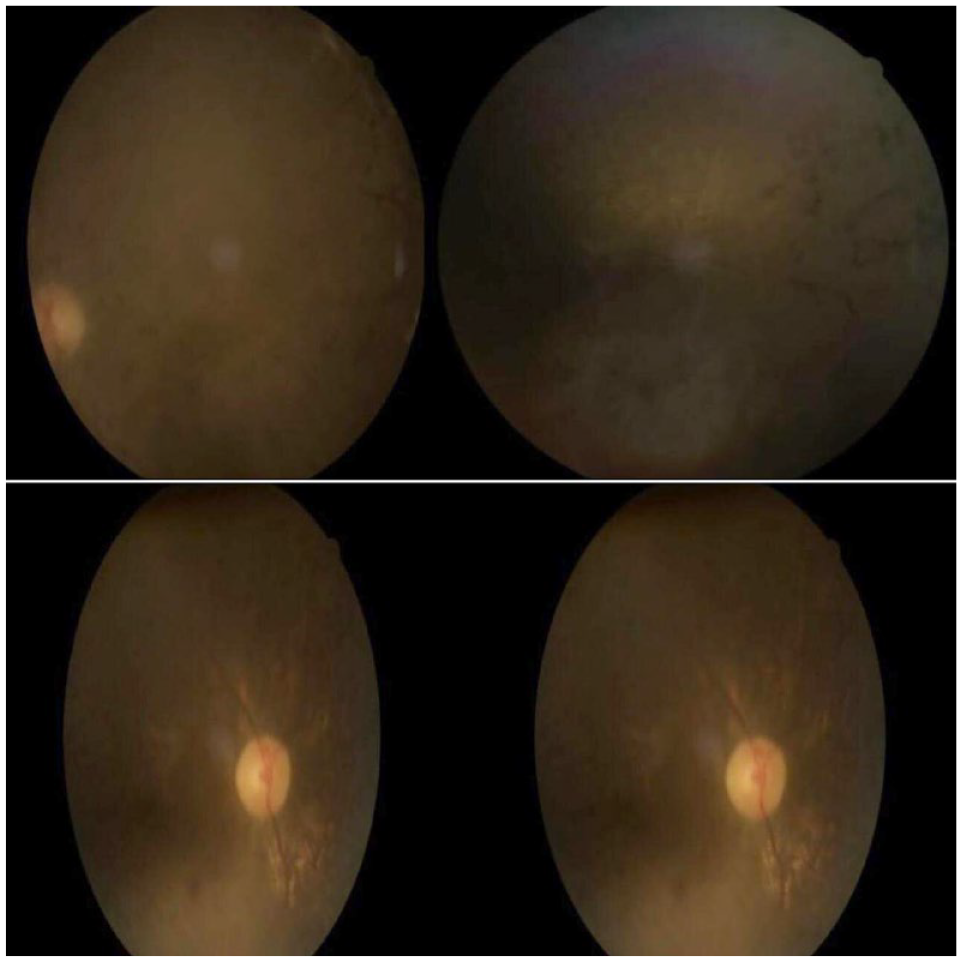
Fundoscopy of both eyes showing bony spicules suggestive of retinitis pigmentosa.
Laboratory investigations were unremarkable except for macrocytic anemia and raised erythrocyte sedimentation rate (ESR) as shown in Table 1.
Laboratory investigations.

Abbreviations: HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; ESR, erythrocyte sedimentation rate; fL, femtoliter; g/dL, gram per deciliter; IU/L, international unit per liter; LDH, lactate dehydrogenase; mg/dL, milligram per deciliter; mm, millimeter; ng/mL, nanogram per milliliter.
Peripheral blood smear showed macrocytosis, poikilocytosis, and anisocytosis while bone marrow showed megaloblastic changes with hyper-segmented neutrophils. She was further investigated and anti-intrinsic factor antibodies were positive which further supported the diagnosis of pernicious anemia that led to vitamin B12 deficiency. An ultrasound of the abdomen and pelvis was done on the fetal lobulated cortical margins, the volume of ovaries was small for age (1.5 mL volume against a normal value of 3). The patient was diagnosed as a case of Bardet- Biedl syndrome according to the clinical diagnostic criteria suggested by Forsythe & Beales [2013] in which our patient had 4 major and one minor features. 5 The patient has transfused 3 pints of red cell concentrates and 1 mg hydroxycobalamin IM 3 times per week for 2 weeks. On 6 weeks of follow up her symptoms improved and her hemoglobin raised to 10.3 g/dL she was further continued with the same treatment but her hydroxocobalamin was switched to once monthly for 3 months.
Discussion
Bardet-Biedl syndrome (BBS) is a rare autosomal recessive disorder with clinical and genetic heterogeneity that occurs when one gene influences 2 or more seemingly unrelated phenotypic traits. It is characterized by structural and functional abnormalities of organs and tissues with diverse embryonic derivation. It requires at least 3 mutations that seem to be required for the phenotype to be clinically expressed as loss of protein-coding for the BBS gene. It is formally known as Laurence Moon Bardet Biedl Syndrome. However, Laurence–Moon–Biedl–Bardet syndrome (LMBBS) is not considered as a right term now. Laurence and Moon had paraplegia but no polydactyly and obesity. However, polydactyly and obesity are primary features of BBS. Thus, Laurence–Moon syndrome is considered to be a separate entity. 6 Pakistan has got a genetically heterogenous population and the ratio of consanguineous marriages is higher than other countries. About 60% of the marriages in the country are consanguineous resulting in an increased incidence of autosomal recessive diseases. About 80% of them are among first cousins, thereby increasing the possibility of homozygous mutations. Despite this disturbing fact, the frequency of LMBBS is still unknown in Pakistan, and the majority of cases go undiagnosed. To date, only 9 cases with these mutations have been reported that do not correlate the existence of megaloblastic anemia with BBS.1,7
BBS patients begin to exhibit symptoms within the first 10 years of their lives. The first complaint is frequently having trouble seeing at night, and nystagmus is frequently discovered. 8 The age at which patients are diagnosed varies greatly depending on when their symptoms of rod-cone dystrophy first appear. Although it can start in infancy, this is more frequently diagnosed between the ages of 5 and 10 and usually begins with night blindness. Nine years old is the typical diagnostic age, when the first signs of vision issues appear. Obesity that appears from early childhood or isolated polydactyly may not often require referral. Without a family history, antenatal diagnosis of BBS is exceedingly rare, however, it might be suspected if echogenic kidneys and polydactyly are seen during an ultrasound examination. 9 According to diagnostic criteria, a patient who had 4 primary features or 3 primaries along with 2 secondary features is considered a BBS patient. Primary features include rod-cone dystrophy, polydactyly, obesity, hypogonadism in males, learning disabilities, and renal anomalies. The Secondary features include speech disorder or delay, brachydactyly/syndactyly, strabismus/cataracts/astigmatism, polyuria/polydipsia (nephrogenic diabetes insipidus), developmental delay, mild spasticity (especially lower limbs), diabetes mellitus, ataxia/poor coordination/imbalance, hypertrophy of left ventricle, other congenital heart diseases, dental crowding/high arched palate, and hepatic fibrosis. 10
Our patient had 4 primary features that is, Rod-cone dystrophy, Polydactyly, Obesity, and Learning disabilities that fulfill the diagnostic criteria of Bardet-Biedl syndrome. Moreover, the bone marrow shows megaloblastic anemia and hypersegmented neutrophils. Although it is unknown if the occurrence of pernicious anemia in this patient has some association with BBS or is just a solitary occurrence. Finding the exact cause will need some genetic studies that will further guide us about the long-term treatment of pernicious anemia in such patients.
There is currently no known treatment for this ailment because of a lack of understanding. Only symptomatic therapy, which necessitates a multidisciplinary strategy focused on each distinct presenting characteristic, can provide relief. The need to routinely monitor the endocrine, lipid, and glucose systems cannot be overstated. Maintaining a healthy weight and blood pressure as well as scheduling routine eye exams are essential for keeping the condition under control. Regular eye exams are crucial for detecting any degenerative changes in the eyes since an early diagnosis can stop further degeneration. Similarly, the patient has to be checked for diabetes and hypertension problems The sickness and how to manage its symptoms should be explained to the patient and those who are caring for them. For individuals in need of assistance, there are visual aids, speech, and behavior treatment, and schools for underprivileged children accessible. Hormone replacement treatment and cosmetic surgery to remove extra digits are other possible options. 11
Conclusion
The clinical presentation of BBS varies and can involve any organ or system of the body. Megaloblastic anemia in BBS is a rarely reported associated condition, further research is needed to find the exact cause of megaloblastic anemia in BBS. The condition might be either due to low intake of vitamins in BBS patients or it might be due to the genetic predisposition. Early diagnosis and vitamin replacement are necessary for better outcomes.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
S.H., Q.A.K., conceived the idea, Q.A.K., P.S collected the data, S.I., N.F.B. did the literature search. H.P., S.R., F.A.H., M. A wrote the original manuscript. Q.A.K., S.H. did the final editing and revised the manuscript critically. All the authors reviewed and approved the manuscript.
Consent
Written informed consent has been taken from the patient’s father to publish this case and its accompanying images. The consent can be available upon Editor in Chief request.
Guarantor
Dr. Qaisar Ali Khan