
Abstract
Background:
Primary spinal osteosarcoma is a rare and intractable disease. Although en bloc resection is favorable for longer survival, it is not always achievable. Separation surgery, a partial resection with circumferential separation to safely deliver high-dose irradiation including intensity-modulated radiation therapy (IMRT), has been recently indicated for patients with spinal cord compression secondary to solid tumor metastases. However, little evidence regarding this combination approach to spinal osteosarcoma exists.
Case presentation:
We report a 55-year-old male patient with a T1 tumor who underwent urgent decompression surgery for epidural spinal cord compression. Pathological findings revealed primary osteosarcoma. Separation surgery, IMRT, and adjuvant chemotherapy were applied to reduce the symptoms of epidural spinal cord compression. The patient was alive without local recurrence at the 5-year follow-up.
Conclusions:
Separation surgery with IMRT can be a relatively safe and effective treatment option in patients with osteosarcoma adjacent to spinal cord when en-bloc resection is challenging.
Keywords
Introduction
Osteosarcoma is an osseous neoplasm, arising frequently in the extremities during adolescence and rarely in the spine. 1 Spinal osteosarcoma accounts for 1% to 3% of osteosarcoma. 1 Recent studies suggested that primary malignant spinal tumors including osteosarcoma should undergo en bloc resection to reduce local recurrence and achieve a complete cure with longer survival.1 -5 Although total en bloc spondylectomy (TES)6,7 can achieve marginal resection of tumors, this procedure requires sacrifice of nerve root and carries major risks, including massive bleeding, spinal cord injury, pleural effusion, and postoperative cerebrospinal fluid leakage.3,8 However, complete marginal resection is not always achievable due to adjacent neurovascular components and impending neurological dysfunction sometimes makes it impossible to perform neoadjuvant therapies aiming for maximizing the chance of marginal resection. 1 Bhatia et al 4 demonstrated that half of the patients with spinal osteosarcomas initially presented with limb weakness. Another traditional treatment option is palliative debulking surgery with adjuvant conventional radiotherapy, which is less invasive. Although adjuvant radiotherapy following biopsy or intralesional resection had a trend toward improved overall survival, this combination approach demonstrated shorter overall survival compared to TES. 1 More recent progresses in radiotherapy including intensity-modulated radiation therapy (IMRT) enabled increased exposure dose to the target with minimizing the damage to healthy tissue near the tumor. 9 However, even though IMRT has high spatial resolution, it is difficult to safely treat patients with spinal tumors adjacent to the spinal cord. Separation surgery, an emerging concept, involves resecting tumor lesions to create a 2 to 3 mm of tumor-free interval between the spinal cord and the vertebra, capable of applying high-dose irradiation for the target adjacent to the spinal cord.10,11 Recently, the combination of separation surgery and IMRT for patients with spinal cord compression secondary to solid tumor metastases demonstrated excellent clinical outcomes.10,11 However, little evidence regarding this combination approach to primary spinal osteosarcoma exists. The aim of this report is to report the outcome of a primary osteosarcoma successfully treated by separation surgery and IMRT.
Report of the Case
A 55-year-old male patient reported a 6-month history of gradually worsening neck pain and a 1-month history of rapidly worsening gait disturbance. He attended a nearby hospital and was initially diagnosed with a T1 solid tumor. He had no family history and no past medical history of malignant tumor. Preoperative computed tomography (CT) scans showed massive bone destruction from the T1 vertebra to the right pedicle. Magnetic resonance imaging (MRI) showed epidural spinal cord compression with complete obliteration of the cerebrospinal fluid space at the affected level caused by a progressive tumor (Figure 1A and B). He underwent urgent decompression surgery with T1 laminectomy and partial removal of the tumor to a feasible extent from the posterolateral aspect and posterior instrumentation with lateral mass screws (C5, C6) and pedicle screws (C7, T2–T4) for epidural spinal cord compression. Hematoxylin and Eosin staining sections demonstrated spindle cells with polymorphic atypical nuclei and osteoid (Figure 2A and B). The tumor was diagnosed as a spinal osteosarcoma.

Preoperative computed tomography (CT) image and magnetic resonance imaging (MRI) showing mass lesion at T1. (A) An axial CT image showing a massive destructive bone lesion from the T1 vertebra to the right pedicle. (B and C) A sagittal T1-weighted MRI (B) and an axial T2-weighted MRI (C) showing epidural spinal cord compression by a progressive tumor (indicated by white arrows) with complete obliteration of the cerebrospinal fluid space at the affected level.
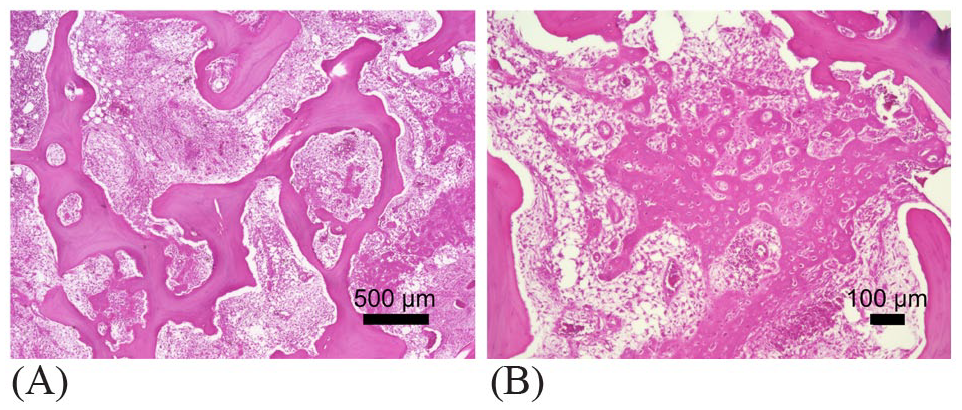
Hematoxylin and Eosin staining microphotographs showing spindle cells with polymorphic atypical nuclei and osteoid of an osteosarcoma with low magnification (×40) (A) and high magnification (×100) (B).
The patient was then referred to our hospital for further treatment. At that time, he was positive for Romberg test and walked with a cane. No metastasis was identified in positron emission tomography (PET)-CT and thus revision surgery for the residual tumor was planned. The Weinstein-Boriani-Biagini 12 classification of the lesion was involvement of sectors 1 through 4 and 9 through 12 with tissue layers B through D. The Tomita et al classification 13 of the lesion was type 4. Since the extraskeletal lesion was large, we determined that it would be difficult to apply TES. Therefore, we chose to treat the lesion with separation surgery and postoperative IMRT. Before separation surgery, transcatheter arterial embolization was performed against the segmental arteries. To confirm the epidural tumor extension, partial laminectomy of C7 and T2 was performed. We removed the region of the tumor that surrounded the epidural spinal cord with no attempt to aggressively remove the residual tumor and achieved circumferential decompression with more than 3 mm of tumor-free interval (Figure 3). The operating time was 6 hours 43 minutes and the blood loss was 490 g. Postoperative MRI showed that the epidural tumor was resected circumferentially from the epidural spinal cord, and epidural spinal cord decompression was accomplished (Figure 4A-C). No complication related with surgery was observed, for example, hematoma, surgical site infection, and neurological deterioration. Two weeks after separation surgery, IMRT at a total dose of 70 Gy was performed (Figure 5) without any irradiation-induced side effects and 4 cycles of doxorubicin and cisplatin were performed as adjuvant chemotherapy. The patient became able to walk without any assistance 3 months postoperatively and returned to work 8 months postoperatively. He exhibited a metastatic tumor to the right lung 3 years after surgery and then underwent resection surgery. At 5-year follow-up, the patient was alive without local recurrence (Figure 6).
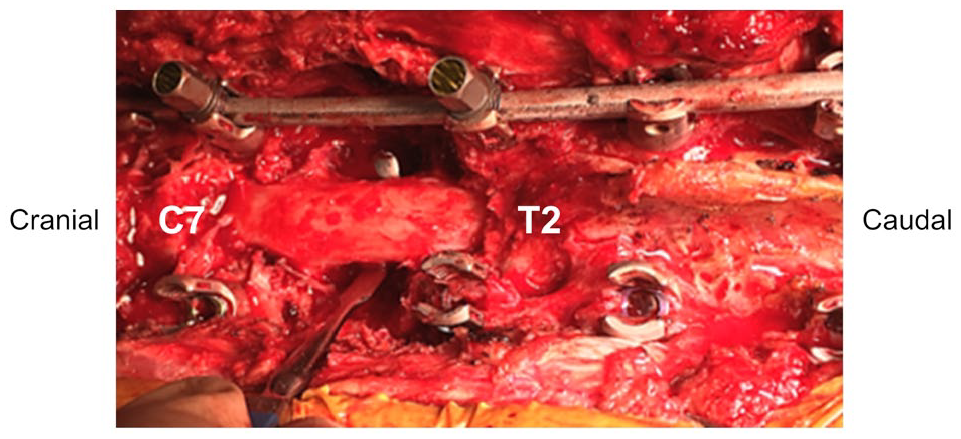
An intraoperative photograph after laminectomy at the level of the epidural tumor extension and at least partially above and below the levels of the tumor indicating circumferential decompression of the spinal cord.

Postoperative images of the cervicothoracic spine with posterior instrumentation between C5 and T4 and circumferential decompression at T1 level. (A and B) A posteroanterior radiograph (A) and a lateral radiograph showing posterior instrumentation from C5 to T4. (C and D) Axial images of computed tomography (C) and T2-weighted magnetic resonance image (MRI) showing sufficient circumferential decompression of the spinal cord.
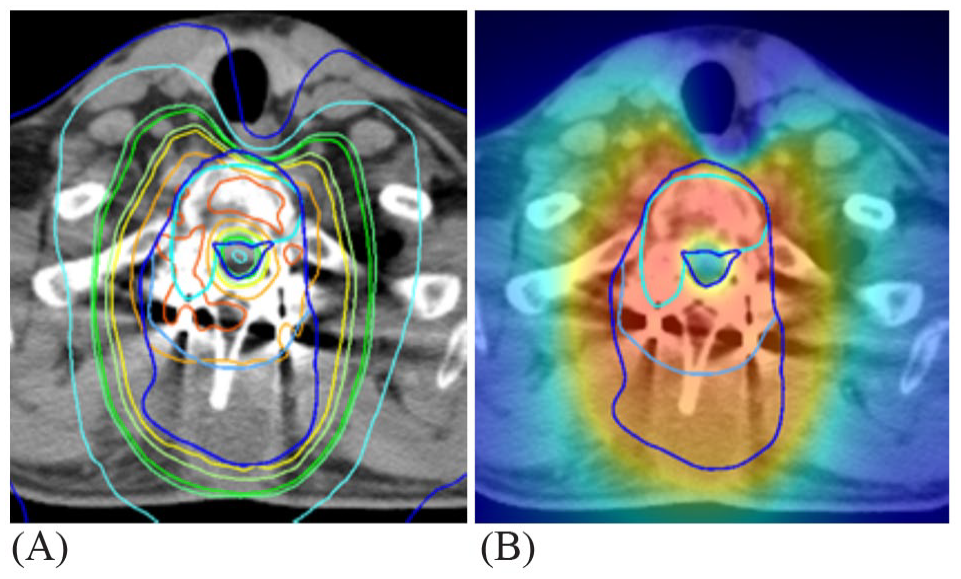
The intensity-modulated radiation plan showing satisfactory prescribed tumor target coverage and excellent sparing of the spinal cord.

A sagittal (A) and an axial (B) T2-weighted magnetic resonance image (MRI) at the 5-year follow-up showing no local recurrence.
Discussion
While the initial therapeutic goal in the management of spinal sarcoma is to achieve a marginal resection, this goal is not always achievable due to the anatomical characteristics. 1 Given its rarity, most studies regarding its local recurrence and survival are limited to small case reports and retrospective case series.
Survival rate for patients with osteosarcoma is much lower in the spinal involvement in comparison to limbs without any metastasis. 14 A multivariate analysis of 1702 patients with osteosarcoma identified an axial tumor site as a poor prognostic factor for response to chemotherapy, overall survival, and event-free survival. 15 The 5-year overall survival rate for patients with osteosarcoma of the extremities and trunk has increased to 55% to 70% owing to the advancements in recent years. 16 However, the Surveillance, Epidemiology, and End Results (SEER) registry from 1973 to 2012 demonstrated that the median overall survival of patients with osteosarcoma of the spine was only 1.3 years. 16 Moreover, partial resection and age are risk factors for short survival.1,15 Longhi et al reported that the 5-year survival rate for patients aged ⩾65 years with osteosarcoma were lower than 22%. 17 A systematic metanalysis from 1966 to 2015 demonstrated that median survival of patients with osteosarcoma of the spine following biopsy or subtotal decompression was 19 months when further surgery was not applicable. 1 This study also showed that patients with revision surgery after partial resection of spinal osteosarcomas had significantly longer survival compared to patients with no further surgery, 1 although it remains unclear whether marginal resection is superior to intralesional debulking for residual tumor. 1
Adjuvant therapy consists of chemotherapy and radiotherapy. A metanalysis demonstrated a substantial survival benefit of adjuvant chemotherapy and radiotherapy. 1 Adjuvant chemotherapy also suggested improved local control of disease. Recently, IMRT is increasingly being employed for the treatment of challenging sarcomas involving the spine. 18 The application of higher radiation doses to spinal tumors, even around the spinal cord, which do not exceed the radiation tolerance, is now possible with the combination of separation surgery and IMRT. In patients with isolated spinal metastasis, this combination approach demonstrated superiority in terms of blood loss and operation time, and non-inferiority in terms of overall survival compared to TES. 10 A retrospective study of 27 patients with paraspinal chordomas and sarcomas including one patient with osteosarcoma who underwent IMRT after surgery demonstrated favorable local control and survival. 18 However, little evidence regarding the combination of separation surgery and IMRT exists in the management of sarcomas, especially osteosarcomas.
Taken together, even though it is difficult to perform TES being the curative treatment, revision surgery and adjuvant chemotherapy would be advantageous for the survival. In the present case, considering difficulty in TES and recent favorable outcomes of adjuvant IMRT for spinal sarcomas, we selected a less invasive separation surgery with postoperative IMRT that may contribute to a relatively less bleeding, short operating time, and no complication. Although more recent studies suggested the effectiveness of proton beam therapy 19 and carbon ion therapy 20 on the survival and local control in patients with unresectable sarcoma of the trunk, these therapies was not chosen as the first choice, because posterior instrumentation had been performed before separation surgery and these therapies was not covered by insurance in our country at that time. Based on poor clinical outcomes in patients with primary osteosarcoma of the spine without marginal resection, our successful outcome of the survival without local recurrence at the 5-year follow-up should be valuable for clinicians when treating such a patient.
In conclusion, separation surgery with IMRT can be a relatively safe and effective treatment option in patients with osteosarcoma adjacent to spinal cord when en-bloc resection is challenging, although TES is ideal in the management for primary malignant spine tumors.
Footnotes
Acknowledgements
Funding:
The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration Of Conflicting Interests:
THE author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Author Contributions
All authors made a substantial contribution to the concept and design of the work; approved the version to be published. Kanda Y and Kakiuchi Y: acquisition, analysis, interpretation of data, and writing first draft of this case report.
Ethics Approval and Consent for Publication
This study was approved by the ethics committee and institutional review board of our hospital. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. The patients and their families were informed that data from the research would be submitted for publication, and gave their consent.