
Abstract
Background:
The development of medicine, especially in oncology, has been helping prolong the cancer patients’ survival, but also leads to increasing the possibility of getting multiple cancers. However, the possibility of getting 4 primary cancers in 4 different sites is extremely rare.
Case presentation:
A 63-year-old female patient was diagnosed with thyroid cancer in 2018, and then with right colon cancer in 2019. In 2020, this patient was diagnosed with left renal pelvis cancer, and most recently, in April 2022, she was hospitalized with bladder cancer diagnosis. Thanks to being closely and regularly followed-up, her malignancies had been detected early and treated suitably. Her health remains stable now and she is under following-up.
Conclusion:
Even though developing another primary cancer in a cancer survivor is not uncommon now and has the tendency to increase, a patient having 4 primary cancers in 4 different sites is still extremely rare and should be noticed, further followed up and investigated. Cancer patients and survivors need to be followed-up regularly, to early detect not only the progression or recurrence but also the second cancer (if it exists), to get timely and suitable treatment.
Introduction
Cancer patients have a 20% higher risk of developing another primary cancer than the general population, and the second primary cancer has become the leading cause of death among patients with prolonged cancer survival. 1 Multiple primary cancers are defined as 2 or more malignancies that arise independently of each other in the same or different organs, while excluding metastatic sites of primary malignancies. 2 The incidence of multiple primary cancers ranges from 3% to 5%; most of them are double cancers, whereas quadruple primary neoplasms are extremely rare with only about 0.3% of all malignant tumors. 3 Here we reported a rare case that a patient has 4 consecutive malignancies in 4 different sites. Based on our literature review, there were only 9 such cases had been reported so far, as presented in the following Table 1.
List of published articles of cases with 4 primary cancers in 4 different sites.

According to this table, the youngest patient diagnosed with 4 cancers was 45 years old, and the oldest was 70. The most common cancer site is breast with five cases. Other common sites are stomach, bladder, colon, and lung. Six of 9 cases were from East Asia (China, Korea, Japan). We have not had information on survival of those patients since all case reports were published when patients were still alive.
Case Presentation
The patient is a 63-year-old female who had no significant medical or family history. She was admitted to our hospital in Marth 2018 with the diagnosis of right thyroid carcinoma on multinodular goiter after ultrasonography suggested a malignant lesion in the right lobe of the thyroid gland, and cytology of a fine-needle aspiration specimen revealed a follicular neoplasm. Thyroidectomy was then performed. The post-operative pathological resulted as pT3N0M0 stage I papillary carcinoma. One month after surgery, a regimen of 50mCI dose of I131 was administered. After completing this regimen, she was discharged and then followed-up by our Outpatient Department.
In October 2019, during a regular check-up, even though she had no symptoms of recurrence or abdominal pain or changing in bowel habit, the abdominal ultrasound showed uneven thickening in her ascending colon wall. Colonoscopy showed an ulcer-like neoplasm in the ascending colon, covering half of the lumen. The biopsy specimen of the neoplasm and abdominal CT-scanner confirmed that she had a second cancer which was cT4aN0M0 colon cancer. Therefore, right hemicolectomy was performed, and postoperative pathology revealed the high-grade adenocarcinoma with serosa, vascular and perineural invasion, with 17/17 inflamed lymph nodes, and high microsatellite instability (MSI-H). Postoperative diagnosis was pT4aN0M0, stage II colon cancer. Consequently, the patient started chemotherapy with XELOX regimen for 4 cycles. Each cycle lasted 3 weeks and consisted of oral capecitabine 1000 mg/m2 twice a day during the first 14 days, combined with IV oxaliplatin 130 mg/m2 on the first day.
In May 2020, right after completing the last cycle, she had macroscopic hematuria. Abdominal contrast-enhanced MRI and further tests detected the third primary cancer in the left renal pelvis (Figure 1). Nephro-ureterectomy was then performed. Her postoperative pathology result was papillary non-invasive carcinoma at pTaN0M0. After surgery, she was discharged and continued to be followed-up.
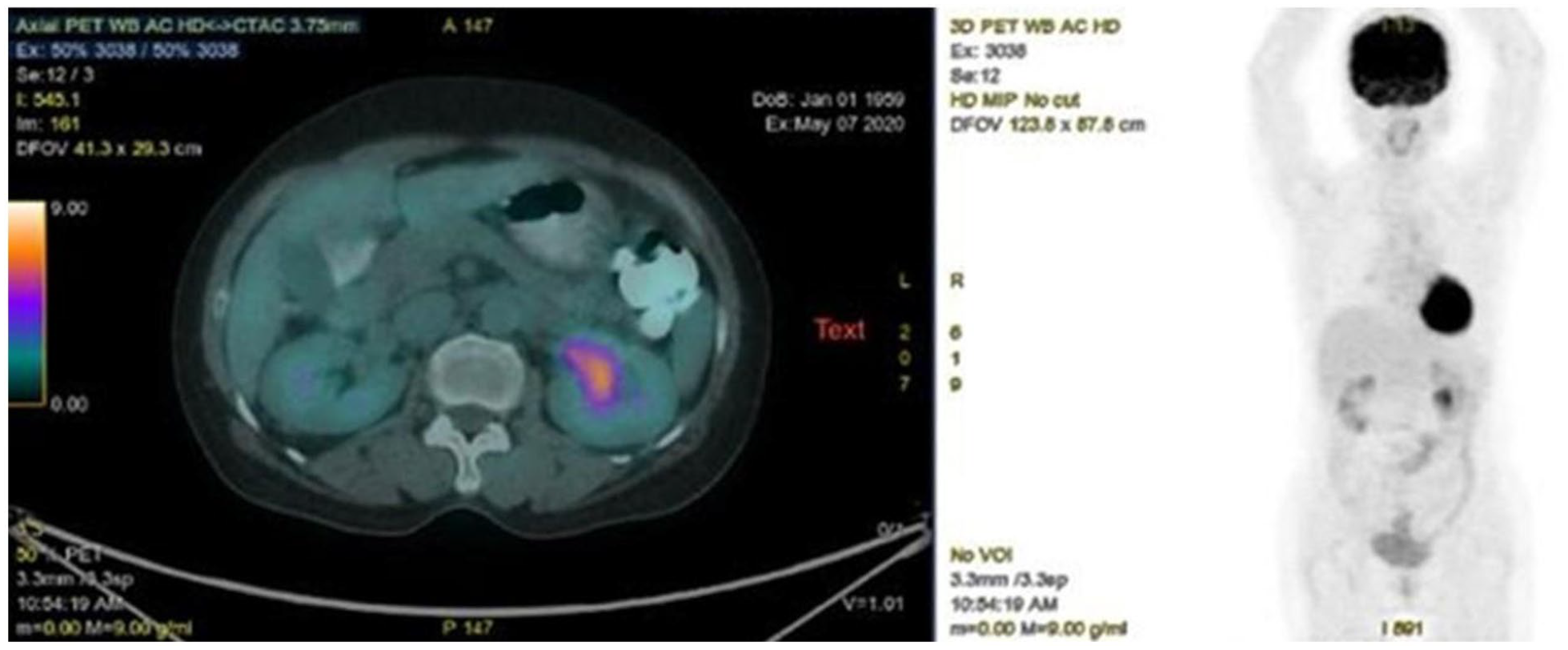
Renal pelvis cancer (FDG 6.5) on PET-CT.
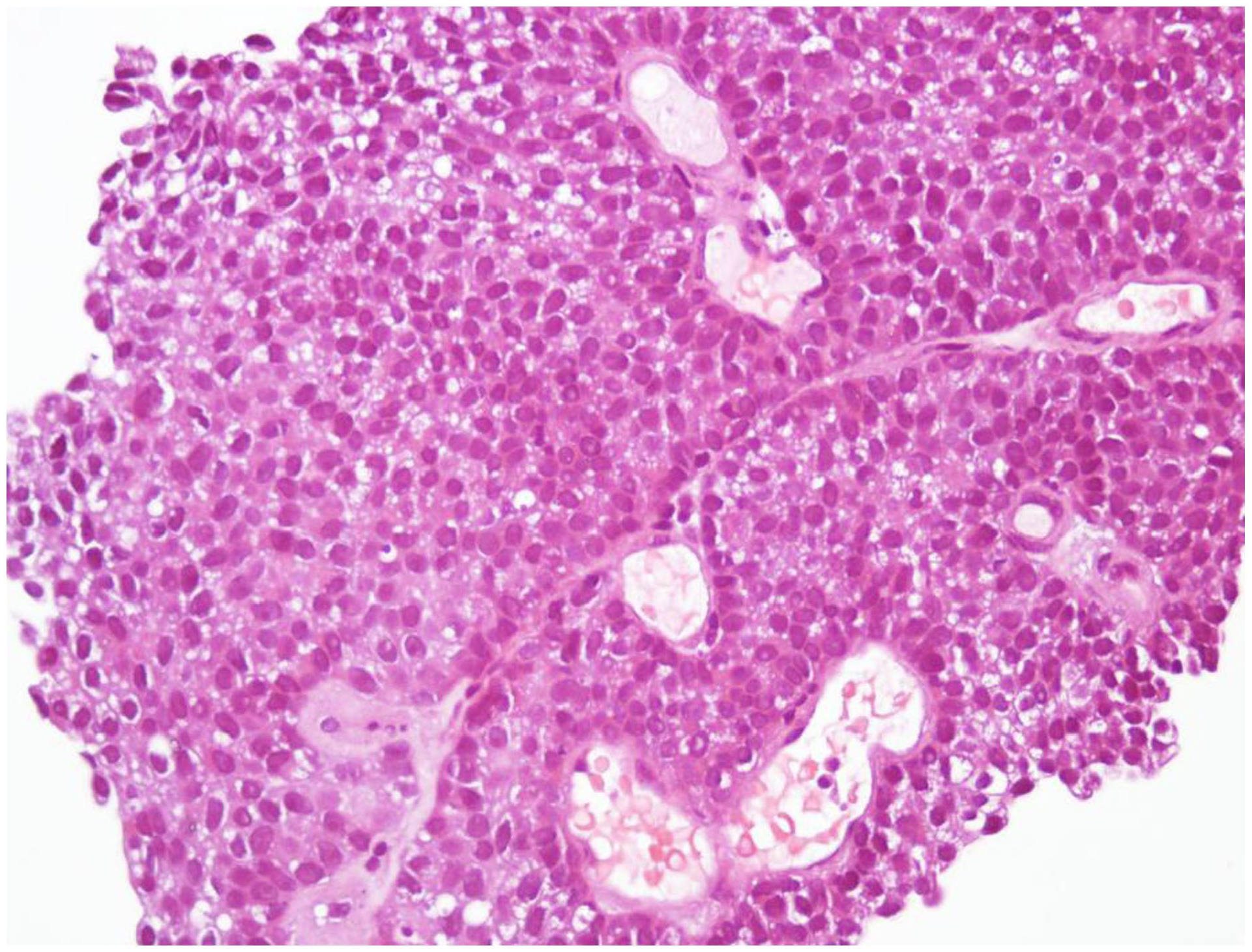
In April 2022, during a scheduled visit, her abdominal ultrasound revealed a lesion in her bladder wall without any reported symptoms. An initial diagnostic flexible cystoscopy showed a 2.5 cm lesion on the right wall of the bladder, without bleeding. Abdominal CT-scanner showed a 14 × 17 mm solitary tumor on the right wall of the bladder with no evidence of surrounding infiltration, neither lymph nodes nor metastases were detected. Histology confirmed that it was the grade 1 urothelial carcinoma of bladder. Transurethral resection of the bladder tumor was performed soon after. The postoperative diagnosis was pG1TaN0M0 bladder cancer. Five days after surgery, she was discharged and has been being followed-up since then. At the time being (December 2022), her overall status is stable; clinical examination and imaging tests showed no signs or symptoms of recurrence or metastases. Figure 2 below is the timeline of her disease progression illustrating when her 4 primary cancers were detected. The histopathological images of 4 sites were presented in the Figures 3 to 6.

Diagram of disease progression.

Histopathological image of thyroid cancer.

Histopathological image of colon cancer.

Histopathological image of left renal pelvic cancer.
Histopathological image of bladder cancer.
Discussion
The risk of getting multiple primary cancers is increasing along with increasing number of cancer survivors. About one-third of cancer survivors over the age of 60 have been diagnosed with another primary cancer. As the number of cancer survivors and the elderly increases, the occurrence of multiple primary cancers is also likely to increase.1,13 In an analysis by Bittorf et al 14 on 50 000 cancer patients over 40 years old, those with more than 2 malignancies accounted for 0.1%.
According to Tanjak et al’s study on 109 054 cancer patients over the 25-year period (1991-2015), multiple primary cancers were found in 1785 patients (1.63%) and more than a half of them were female (55.6%). 15 In a study conducted by Watanabe et al on 5456 autopsy cancer cases in Japan, there were 285 cases (5.2%) with 2 cancers and 58 cases (1%) with 3 or more cancers. Patients with oropharyngeal cancer, bowel cancer, laryngeal cancer, uterine cancer, bladder cancer, and thyroid cancer, had a higher probability of suffering from the second cancer. 16
According to Boice et al’s study, compared to the general population, cancer patients had a 31% (RR = 1.31) increased risk of developing a second cancer and a 23% (RR = 1.23) elevated risk of second cancer at a different site from the first; Common environmental exposures seemed responsible for the intensive appearance of the second cancer, especially those related to smoking, drinking, or both. 17
Genetic studies conducted over the last decades have led to the identification of a number of cancer susceptibility genes. Mutations of tumor suppressors and protooncogenes were proved to be the cause of syndromic presentation of secondary primary cancers.18,19 Bychkovsky et al’s analysis on 9714 multiple primary cancer patients showed the prevalence of germline pathogenic variants increased with the number of primary cancers (PCs): 13.1% with 2 PCs, 15.9% with 3 PCs, and 18.0% with ⩾4 PCs (P = .00056). 20 In Win et al’s study over an average follow-up duration of 5 years, people with mismatch repair had an increased risk of colorectal cancer, bladder cancer, and urinary tract cancer. 21 Lynch syndrome (LS) is also a high-risk factor for multiple primary cancers. Patients with LS may have an increased risk of colorectal cancer and other malignancies compared to the general population. 22 LS is caused by germline mutations in the DNA mismatch repair (MMR) genes MLH1, MSH2, MSH6, and EPCAM, and these MMR proteins can be detected by immunohistochemistry, but the final diagnosis of LS should be confirmed by genetic testing. Our patient has been confirmed with MSI-H status, thus we have recommended her to take genetic tests to detect certain mutations and LS, but due to unaffordability, the patient refused to do those tests.
In our patient, we could see some risk factors of multiple cancers such as her old age and her first primary cancer which is thyroid cancer. However, we have not found any relationship of her disease with smoking or drinking or family history. We also see some similar factors between our patient and published cases in the Table 1 such as being female, elderly, from East Asia, and having bladder and colon cancer. We speculate that this patient’s multiple primary malignancies might be attributed to individual sensitivity, or her MSI-H status or chemotherapy factors that she has absorbed.
Even though developing another primary cancer in a cancer survivor is not uncommon now and has the tendency to increase, a patient having 4 primary cancers in 4 different sites is still extremely rare and should be noticed, further followed up and investigated. Cancer patients and survivors need to be followed-up regularly with a scheduled medical examination program, to early detect not only the disease’s progression or recurrence, but also the second cancer (if it exists), in order to get timely and suitable treatment. By reporting this rare case of 4 primary cancers, we hope to share our clinical information and experience, thus contribute to improve the quality of diagnosis and treatment for cancer patients.
Footnotes
Acknowledgements
The authors would like to thank Dr. Nguyen Thanh Hang, Department of International Cooperation and Scientific Research, Hanoi Oncology Hospital, for editing English and providing consultation on academic writing.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Conceptualization, D.T.N; Writing—Original Draft, D.T.N, L.M.N; Writing—Review & Editing, D.T.N, T.L.P; Visualization, L.M.N; Supervision, Q.V.B.
Ethical Statement
Informed consent was obtained directly from the patient for publication of this case and all photos included therein. Given that this manuscript includes the description of 1 single case, it does not meet criteria for “human subjects research” and as such is exempted from IRB review.