
Abstract
Background:
Directional coronary atherectomy (DCA) revived in Japan since 2014. DCA is a special device to remove the atherosclerotic plaque of coronary artery in percutaneous coronary intervention (PCI). However, DCA procedure is recommended to perform by 8Fr system, which is one of the limitations of DCA.
Case Series:
Since transradial approach is the main access route for PCI, we considered how to perform DCA by TRA. The external diameter of 8Fr guiding catheter (GC) and 6Fr sheath are 2.70 and 2.67 mm. Then, if 6Fr sheath can be inserted without any resistance, 8Fr GC is considered to be insertable. We performed 5 cases of DCA by the transradial 8Fr sheathless GC approach, all cases were successful without discomfort associated with insertion and removal of the 8Fr GC.
Conclusion:
DCA by the transradial 8Fr sheathless GC approach might be one of options to avoid bleeding complication and serve more comfortable treatment for the patients.
Introduction
Directional coronary atherectomy (DCA) (Atherocut™, NIPRO, Japan) revived in Japan since 2014 and it has been reported the effectiveness of DCA from Japan.1,2 Revived DCA can be insertable into 7Fr guiding catheter (GC). However, confirming by angiography during DCA procedure is very difficult in 7Fr GC system because DCA is so tight for 7Fr GC. Therefore, DCA procedure is recommended 8Fr GC because it is important to confirm the debulking position correctly. Since 8Fr system is basically performed by femoral approach, complications at the puncture site are concern. The transradial 8Fr sheathless GC approach is one way to solve this problem, and we succeeded DCA by transradial approach (TRA).
We describe a first case report of DCA by the transradial 8Fr sheathless GC approach. Because there are many high bleeding risk (HBR) patients, the approach reported here may be a potential of useful technique for HBR patients even in DCA.
Case Series
Procedure of the transradial 8Fr sheathless GC system is shown here. The approach site can be done by right or left radial artery. As shown in Figure 1A, the 8Fr sheathless GC system is made by inserting the 125-cm 6.5Fr inner catheter (STA, MEDKIT Co. Ltd., Tokyo, Japan) into a 100-cm 8Fr CL3.5SH (RoadMaster, GOODMAN Co. Ltd., Aichi, Japan). After insertion of 6Fr sheath, we exchange using a 260 cm 0.035′ guidewire from 6Fr sheath to the 8Fr sheathless GC system. Because the inner catheter tapers down to the 0.035′ guidewire and easily inserted on the wire into the radial artery, the tip of the 8Fr GC can follow easily during open the skin entry site with a surgical blade (Figure 1B). The full system is advanced through the radial to the ascending aorta. After removal of the inner catheter, the 8Fr GC is engaged into the coronary ostium as usual. The inner and outer diameter of 8Fr GC and 6Fr sheath are shown in Figure 1C. The external diameter of 8Fr GC is equivalent to the external diameter of 6Fr sheath. Then, if 6Fr sheath can be inserted without any resistance, 8Fr GC is considered to be insertable.
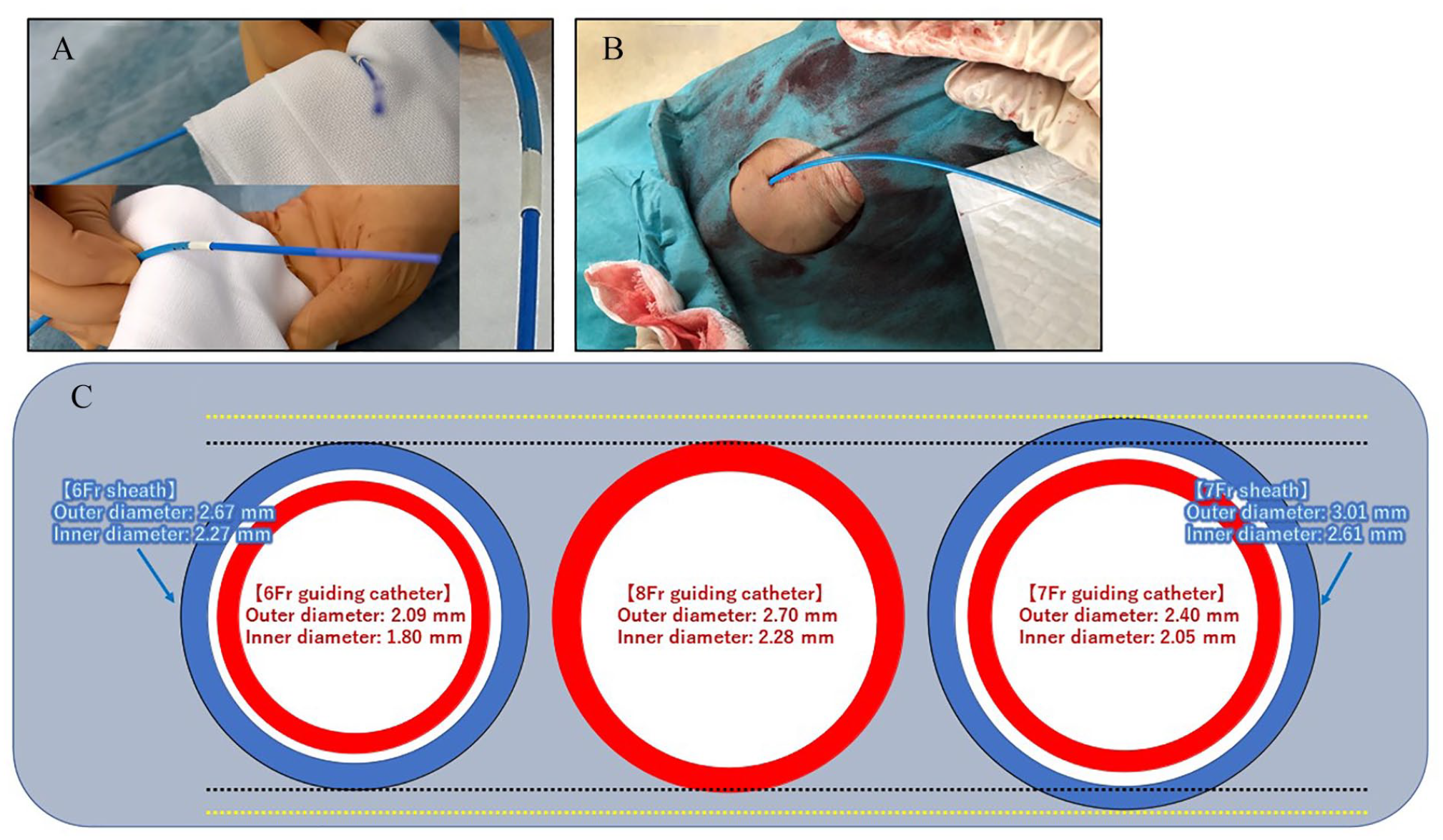
(A) The sheathless system is made by inserting the 125-cm 6.5Fr inner catheter into a 100-cm 8Fr GC. (B) Example of inserted the transradial 8Fr sheathless GC system. (C) Comparison of inner and outer diameter of 6Fr sheath, 6Fr GC, 8Fr GC, 7Fr sheath, and 7Fr GC.
Since April 2020, we treated 5 patients with DCA by the transradial 8Fr sheathless GC system successfully. In all cases, the postoperative course was good and there was no occlusion of the radial artery after procedure. We performed DCA-Drug-coated Balloon (DCB) treatment with the goal of debulking up to the percent plaque area (%PA) <58.5% according to previous report. 3
Case-1: A 72-year-old woman was hospitalized with a complaint of exertional angina. Her coronary risk factors were hypertension and dyslipidemia. Culprit lesion was a stenosis of the proximal left anterior descending artery (LAD) (Figures 2AI). DCA (L-size) performed (15 cuts) by the transradial 8Fr sheathless GC approach (Figure 2AII) and final angiogram showed excellent result successfully with 3.0 mm DCB (SeQuent® Please NEO, NIPRO, Osaka, Japan) (Figure 2AIII). The %PA before and after DCA were 82% and 55%, respectively.
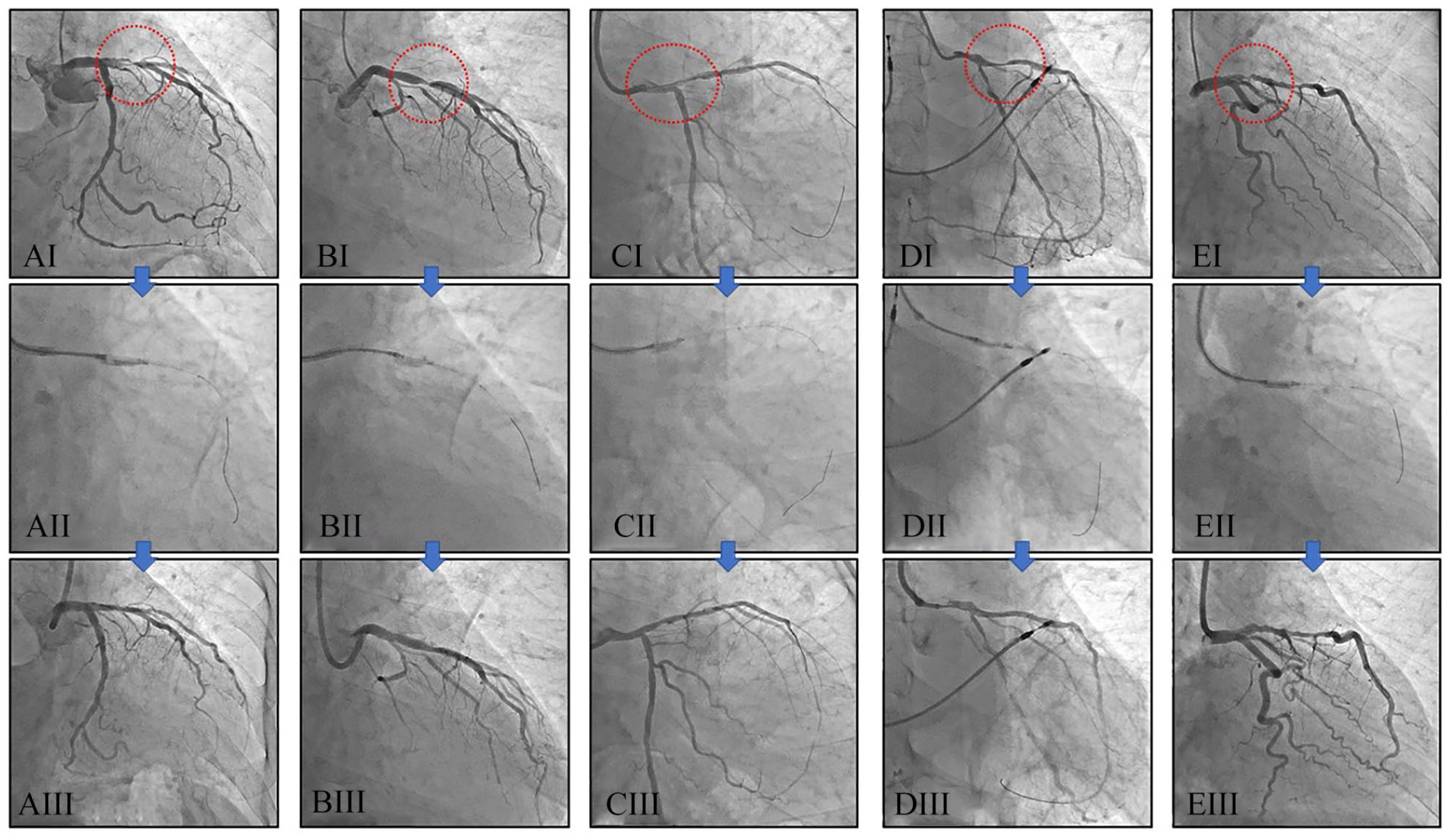
DCA cases using by the transradial 8Fr sheathless GC system. (AI-AIII) A 72-year-old woman. (BI-BIII) A 72-year-old man. (CI-CIII) A 66-year-old man. (DI-DIII) A 76-year-old man. (EI-EIII) A 61-year-old woman.
Case-2: A 72-year-old man was hospitalized with a complaint of exertional angina. His coronary risk factors were dyslipidemia and current smoker. Culprit lesion was a stenosis of the proximal LAD (Figures 2BI). DCA (L-size) performed (16 cuts) by the transradial 8Fr sheathless GC approach (Figure 2BII) and final angiogram showed excellent result successfully with 3.5 mm DCB (Figure 2BIII). The %PA before and after DCA were 83% and 53%, respectively.
Case-3: A 66-year-old man was hospitalized with a complaint of exertional angina. His coronary risk factors were hypertension, dyslipidemia, diabetes, and current smoker. Culprit lesion was a stenosis of the just proximal LAD (Figures 2CI). DCA (L-size) performed (18 cuts) by the transradial 8Fr sheathless GC approach (Figure 2CII) and final angiogram showed excellent result successfully with 3.0 mm DCB (Figure 2CIII). The %PA before and after DCA were 82% and 55%, respectively.
Case-4: A 76-year-old man was hospitalized with a complaint of exertional angina. His coronary risk factor was hypertension. Culprit lesion was a stenosis of the proximal LAD (Figures 2DI). DCA (L-size) performed (13 cuts) by the transradial 8Fr sheathless GC approach (Figure 2DII) and final angiogram showed excellent result successfully with 3.0 mm DCB (Figure 2DIII). The %PA before and after DCA were 85% and 56%, respectively.
Case-5: A 61-year-old woman was hospitalized with a complaint of exertional angina. Her coronary risk factors were hypertension, dyslipidemia, and diabetes and she had metal allergies. Culprit lesion was a stenosis of the proximal LAD (Figures 2EI). DCA (L-size) performed (15 cuts) by the transradial 8Fr sheathless GC approach (Figure 2EII) and final angiogram showed excellent result successfully with 3.5 mm DCB (Figure 2EIII). The %PA before and after DCA were 83% and 55%, respectively.
The 8Fr sheathless GC system was removed after procedure and hemostasis was achieved by the use of a TR Band (Terumo, Tokyo, Japan) without any problems. No complications have occurred such as pseudo-aneurysm, arterial-venous fistula, thrombosis, compartment syndrome, and occlusion of radial artery.
Discussion
We first described that the DCA using by the transradial sheathless approach with the 8Fr GC. The principal findings were that the insertion of 8Fr GC is easy and the procedure of DCA can be also performed as usual. All cases were not needed to convert a conventional system using sheath. TRA is a common approach instead of the transfemoral approach recently because complication rate in TRA is significantly lower than transfemoral approach 4 and TRA improve patient comfort and reduce mortality. 5 Recently, the effectiveness and safety of TRA have been reported even in chronic total occlusion (CTO) lesions. 6 However, since the size of radial artery is smaller than femoral artery, one limitation is that the 8Fr sheath cannot be used for insertion. Therefore, the 8Fr sheathless GC system may be useful for procedures that require 8Fr GC such as DCA and intravascular ultrasound guide technique in CTO. If it is possible to insert 6Fr sheath, inserting the 8Fr sheathless GC system may be possible without any troubles, because the outer diameter of 8Fr GC is smaller than that of 7 Fr sheath and equivalent to the outer diameter of 6Fr sheath as shown Figure 1C. Use of the sheathless system allows the use of larger lumen GC without increasing the maximal external diameter of the system via the radial artery. We need to be committed to providing the less-invasive and comfortable treatment for the patient.
Although DCA catheter is available in 7Fr GC system, 8Fr GC system is better to maintain adequate pressure waveform and contrast injections during DCA. The concept that DCA can only be done from a femoral approach is one obstacle to the spread of DCA treatment. We hope that our report helps to lower the threshold of DCA. We think the stability of the 8Fr sheathless GC system is sufficient, because we did not encounter the slipping back or forward of the 8Fr sheathless GC system during procedure. In fact, sufficient debulking was achieved in all cases and the patients were able to finish with stent-less treatment using DCB. Since, the efficacy and safety of stent-less treatment by using DCB has been reported,3,7 we will investigate the clinical outcomes of DCA/DCB treatment in the future. During the period of these cases, only 1 case was DCA by transfemoral approach, because her bilateral radial arteries were poorly palpated. Then, the percentage of DCA by TRA is 83% (5/6 cases) in our institution, which is getting higher. However, femoral approach may be preferred when delicate manipulation of GC is required, such as left main trunk lesion, or short left main trunk case. Elaborate control of GC in the sheathless GC system is difficult compared with the usual system using sheath. Therefore, we have to adjust our procedure flexibly according to the anatomy or lesion morphology in each patient.
It has been reported that 8Fr sheathless GC system did not increase procedure time, contrast volume, or radiation dose and showed the effectiveness and safety in percutaneous coronary intervention (PCI) to CTO 8 and left main trunk. 9 We considered that DCA treatment by transradial sheathless approach using 8Fr GC is not only feasible but also provides high efficacy with acceptable safety margin like previous reports.8,9 We will investigate this point including the incidence of occlusion of radial artery collaborating with other facilities in a future.
Conclusions
The transradial 8Fr sheathless GC approach may be useful method in DCA to reduce complication when the size of radial artery is appropriate. In addition, we considered that it is advantageous to have another way of approach in the PCI procedure.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
T.N. designed and executed the procedure and drafted the manuscript.
T.I. and Y.K. were contributed to the concept and helped to write the manuscript.
S.T. is a co-supervisor and edited the manuscript.
E.T. is a supervisor and edited the manuscript.
All authors reviewed and approved the final manuscript.