
Abstract
Extracranial carotid artery aneurysms are extremely rare aneurysms. Treatment options are conventional open surgery, endovascular surgery, and conservative treatment. Surgical treatment of such aneurysms is challenging and it is important to determine the treatment strategies wisely. There is still no definite association for treatment modalities. In this case report, we present open surgical treatment of a 58-year-old female patient with internal carotid artery aneurysm. The patient was admitted to our clinic with spontaneous pulsatile mass in the right jugular region. Computed tomography angiography shown right internal carotid artery aneurysm. Aneurysm cranial distance was enough to perform end to end anastomosis. Aneurysm was excised by preserving cranial nerves. No complications developed during the postoperative period.
Introduction
Extracranial carotid artery aneurysms (ECAA) are encountered as rare and life threatening cervical or parapharyngeal pulsatile masses, which are primarily recognized by otolaryngologists or cardiovascular surgeons. 1 The incidence of these aneurysms is between 0.4% and 4% out of all peripheral arterial aneurysms. Carotid artery aneurysms should be treated due to high risk of cerebral embolism and compression-induced nerve damage, rupture and bleeding.2,3 These aneurysms and pseudo aneurysms are usually asymptomatic. 4 Generally; atherosclerosis is the most common cause of such aneurysms. 5 Furthermore neurological deficits in patients after neck injuries should arise suspicion of the presence of a carotid artery aneurysm. 6
Available options in ECAA management are conventional open surgery, endovascular surgery and conservative treatment. 3 Conventional surgical operations include end-to-end anastomosis and vein graft interposition. The most problematic part of conventional surgery is nerve damage that develops in aneurysms close to the base of the head. Endovascular surgery using closed stents are becoming more popular. The advancement in endovascular technologies and its relatively easier use is one of the contributing factors in this popularity. Although certain classifications such as Attigah classification have been defined in the field of conventional surgery, endovascular and surgical indications are still needed to be clarified due to low number of cases and long-term follow-up in previous reports.7,8
The purpose of this case report is to demonstrate that conventional surgical repair is still effective in selected patients in ECAA despite the use of endovascular repair methods which is reported to be successful with an increasing frequency.
Case Report
A 58-year-old female patient with no known history of hyperlipidemia, hypertension, coronary artery disease, trauma or previous neck surgery was admitted to our clinic with a spontaneous pulsatile mass that caused swelling in the right jugular region. Computed tomography (CT) angiography was performed previously at another medical center and an 3.31 × 2.84 cm arterial aneurysm which was located distally to the bifurcation was revealed in right internal carotid artery (ICA) (Figure 1). The neck of the ICA aneurysm was clearly demonstrated and cranial distance was enough to perform end to end anastomosis (4.64 cm) (Figure 2). Treatment options were revised by our team and conventional surgery was selected for the patient. The first reason for this choice is the absence of additional surgical comorbidity. The second is that the head base distance of the aneurysm fits end to end anastomosis. The third is the risk of distal embolism, which may occur with the development of spontaneous aneurysm on the atherosclerotic ground, even if it is not observed in CT angiography results. Also there was no sign of pseudoaneurysm, the aneurysm size was sufficient and the patient’s will to get rid of the mass supported our decision.
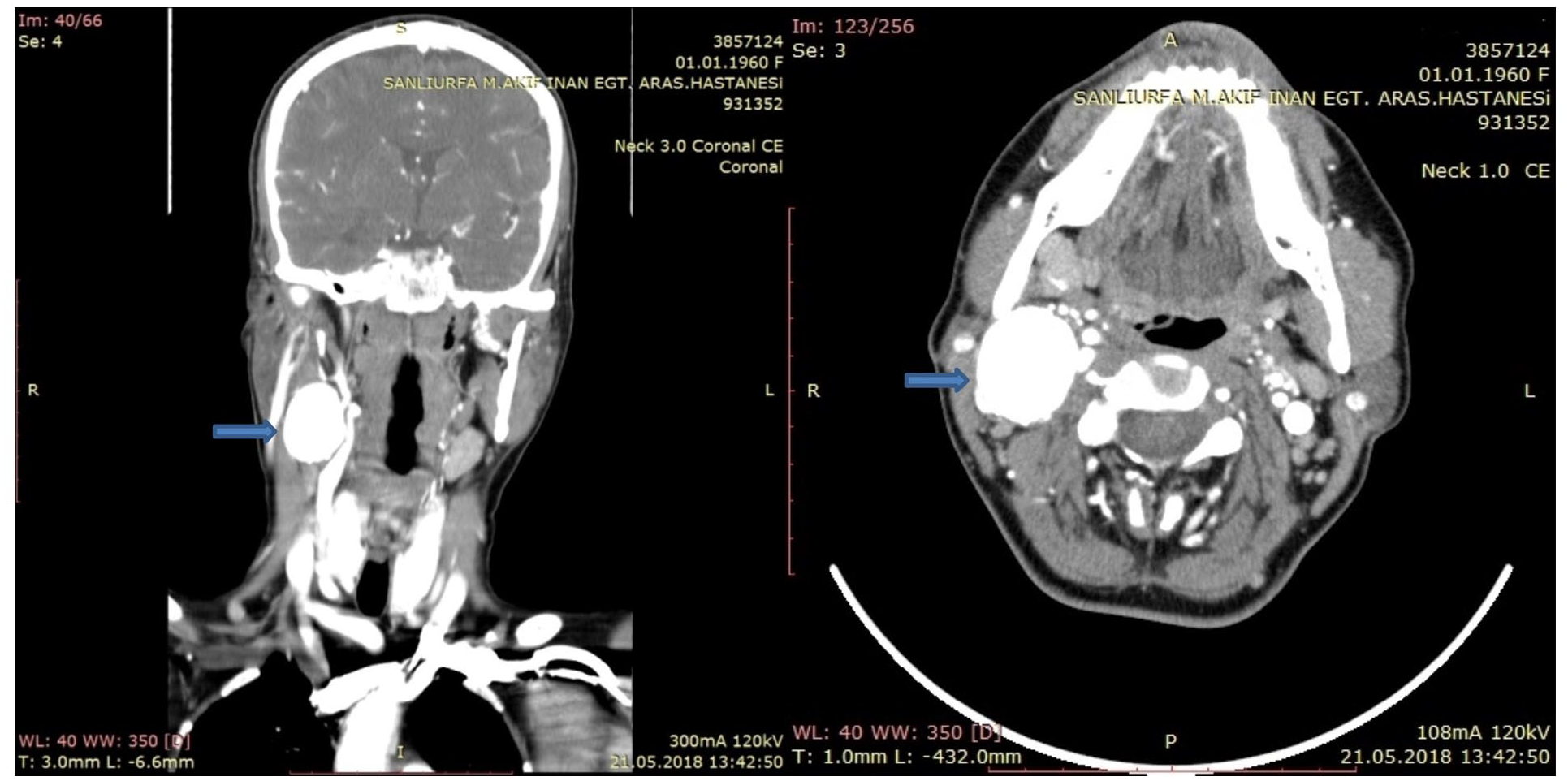
CT angiography image before operation. Blue arrow shows right internal carotid artery aneurysm.

CT angiography image before operation—the distance of internal carotid artery aneurysm to the cranium is 4.64 cm.
In our case, it was thought that cranial perfusion would be sufficient because of good left carotid artery circulation. There is no consensus on the routine use of EEG and shunt applications previous studies.9,10 Therefore, EEG monitoring and shunt application were not used during the operation. Under general anesthesia the patient was prepped and draped, an incision was made through the medial border of the sternocleidomastoid muscle. Common carotid artery (CCA), ICA, external carotid artery (ECA) and aneurysm were exposed by protecting cranial nerves (Figure 3). Carotid artery was clamped; the aneurysm was excised with blunt and sharp dissections. After removal of the aneurysm, proximal and distal ends of the ICA were seen to be in sufficient length. Proximal and distal ends of the ICA were repaired by end-to-end anastomosis without vein graft. A specimen of aneurysm wall was sent to pathology department and the results were well-matched with a true aneurysm. An antiplatelet treatment consisting of 1 drug was initiated (acetylsalicylic acid 100mg) and was continued after the discharge. There were no complications in postoperative period and she was discharged uneventfully on the fifth postoperative day. A CT angiography examination was carried out 12 weeks after the surgery (Figure 4). Flow was sufficient in control angiography and no stenosis or re-developing aneurysm was observed in the right carotid artery.

Operation images of: (A) ICA aneurysm, (B) N.Vagus during the operation, (C) ICA aneurysm + carotid arteries, and (D) ICA aneurysm after surgical excision.

CT angiography (3D) images, 12 weeks after surgery. Blue arrow shows repaired right internal carotid artery aneurysm.
There is no consensus on the routine use of EEG and shunt applications in the studies conducted. In our case, it was thought that cranial perfusion would be sufficient because of good left carotid artery circulation. Therefore, EEG monitoring and shunt application were not used during the operation
Discussion
There are a limited number of case reports in the literature regarding to the actual true extracranial carotid aneurysms. The treatment and surgical approaches of these patients vary with certain limitations. The optimal treatment is controversial and guidelines are not precise. 11 Treatment options depend on the etiology of the aneurysm, its size, neighboring structures, safe distance to the skull base, additional diseases that increase mortality, various treatments performed beforehand (radiotherapy, previous surgery, etc.) and the patient’s desire. Although conventional surgery is considered as a long-term primary treatment, preference in this modality changes with intravascular interventions due to developing technology. The success rates of both treatments are similar observed in medium and long-term studies. Regarding both forms of treatment, the decisive factors are risk of cranial nerve damage, re-intervention necessity, mortality, length of hospital stay, and frequency of cerebrovascular events.3,12,13
Various studies have shown that surgical treatment is one of the effective treatment methods in carotid aneurysms.1,8,13 The localization, etiology, clinical development and operative approaches of the lesions were investigated. The indication for surgical treatment was defined as the increase in the internal carotid artery (ICA) diameter and an increase of more than 50% of the common carotid artery. Anatomical properties and relations to the surrounding structures were the main factors on determining surgical strategies. 14
Although there is no discussion about its effectiveness, 8 conventional surgery has several limitations. These limitations started to be overcome with the advancement of endovascular treatment techniques. The most important limitation in our humble opinion is that conventional open surgery is dangerous to be performed in aneurysms which are close to the skull base where proximal and distal ends of the carotid artery cannot be controlled. The most common complication described after conventional intervention therapy was cranial nerve damage, which occurred in 11.8% of patients after surgery. 15 Cranial nerve injuries and length of hospital stay are reported to be high compared to endovascular treatment. Despite these disadvantages, it is still regarded as an effective method in eliminating the mass effect due to aneurysm. 12
Endovascular treatment will be especially useful in cases which are located close to the base of the skull where proximal and distal carotid artery is difficult to control. It will also minimize risks in patients receiving re-do neck surgery and in patients receiving radiotherapy to the neck area. Another effective endovascular treatment is pseudoaneurysms and traumatic dissections. Degeneration due to atherosclerosis in real aneurysms is not evident in these lesions and cerebrovascular events that may develop during the open procedure are less common. The most important problem in endovascular procedures is that the rate of reprocessing such as re-stenosis is higher than surgical operations.12,13
Endovascular therapies should be recommended to patients when there is no healthy ICA other than the extracranial aneurysm or there is not enough ICA length to be taken under control. Treatment modality of carotid artery aneurysm has largely evolved from operative to endovascular intervention at many institutions. Treatment benefits of endovascular modality include shorter convalescent and less procedure-related complications. This evolution reflects the improvement of endovascular devices and increased utility of endovascular applications. 16
Conclusion
Information on extracranial carotid artery aneurysms is limited. The etiology and course of this disease is not fully understood and criteria for treatment selection between open surgery versus endovascular intervention have not been thoroughly determined. Surgical excision of extracranial carotid aneurysm is one of the most effective treatment method but we still need qualitative studies reporting on the parameters mentioning size, volume and configuration of the aneurysm which can be used to determine the indications. Further studies on ECAA will complement these shortcomings.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed equally in the write-up and editing of the article.
Informed Consent
Consent was obtained from the patient for publication of the images and the case report
Disclaimer
Summary of this case report is presented at the 15th Congress of Turkish Cardiovascular Surgery Association, [PS-321], 26-29 October 2018, Belek, Antalya. The full article has not been submitted/published elsewhere.