
Abstract
Introduction:
Insulin is synthesized in the β-cells from preproinsulin. Preproinsulin becomes proinsulin after leaving the signal peptide. Proinsulin is separated into C-peptide and insulin by 2 enzymes. Hyperproinsulinemia is suspected to be a pancreatic β-cell defect that is augmented by the increased demand placed on the β-cell by hyperglycemia.
Case presentation:
A 39-year-old Japanese man visited to Shin-suma hospital in May 2013. Liver dysfunction, dyslipidemia, and hyperuricemia had been found in medical checkups in his workplace. Therefore, he visited Shin-suma hospital in order to receive intensive examination. Diet and exercise therapy were initiated. In November 2013, intact proinsulin and proinsulin per insulin (PI/I) ratio were evaluated as part of an ongoing study. His intact proinsulin level and PI/I ratio were markedly elevated. A 75 g oral OGTT revealed that his glucose tolerance was impaired. His glycosylated hemoglobin was 6.9%. He was diagnosed as having type 2 diabetes mellitus. Although, diet and exercise therapy continued, his hyperproinslinemia and diabetes mellitus remained. Therefore, aloguliptin was started in order to recover insulin secretion in November 2014. Thereafter, pioglitazone was added to improve insulin resistance. Finally, luseogliflozin was commenced to expect glucose-lowering effects. His HbA1c was stabilized. To the best of our knowledge, there have been few reports of patients with hyperproinsulinemia.
Conclusion:
When the physicians face treatment resistance in diabetes mellitus, we emphasize that evaluation of proinsulin should be considered as one of the methods.
Introduction
Type 2 diabetes mellitus is characterized by both β-cell dysfunction and insulin resistance. It is also demonstrated that the proinsulin processing system might deteriorate not only in diabetics, but also in non-diabetic Japanese individuals with age. We evaluated plasma proinsulin per insulin (PI/I) ratio by measuring plasma intact proinsulin. 1 Intact proinsulin significantly correlated with insulin resistance as determined by HOMA-IR in type 2 diabetes mellitus. 2 On the other hand, PI/I ratio negatively correlated with maximum β-cell secretory capacity induced by arginine injection in type 2 diabetes mellitus subjects. 3 According to Saisho et al, 4 PI/I ratio did not correlate with HOMA-IR. It is very important to know that the measuring PI/I ratio can be the only method to evaluate the impaired insulin processing within pancreatic β-cells in clinical practice. On immunoradiometric assay and chemiluminesence (MLT Research, Cardiff, UK) assay, the intact proinsulin was measured. The incubation condition for the antigen-antibody reaction was changed to overnight at 4°C, instead of 2 hours at 37°C recently. 5 Koyama et al 5 modified the intact proinsulin assay system to minimize the breakdown of proinsulin during the assay. Instead of 2 hours at 37°C, the incubation for the antigen-antibody reaction was changed to overnight at 4°C. In the present report, one prominent case of hyperproinsulinemia in a middle-aged patient is presented.
Case Presentation
A 39-year-old Japanese man visited to Shin-suma hospital in May 2013. Liver dysfunction, dyslipidemia and hyperuricemia had been were found at out in medical checkups in his workplace. Three months later he visited Shin-suma Hospital in order to receive intensive examination. He had no other medical history. His mother had type 2 diabetes mellitus and was treated with insulin injection therapy. On examination, his height, weight, and body mass index (BMI) were 164.5 cm, 67 kg, and 24.6 kg/m2, respectively. On arrival, laboratory tests showed that his fasting plasma glucose level was 114 mg/dL (normal < 126), glycosylated hemoglobin 6.1% (normal NGSP < 6.5), LDL-cholesterol 141 mg/dL (normal < 140), HDL-cholesterol 39 mg/dL (>normal 40), Triglyceride 98 mg/dL (normal < 150), AST 29 IU/L (normal < 34), ALT 73 IU/L (normal < 43), and uric acid 6.3 mg/dL (normal < 7.0), respectively (Table 1). Abdominal ultrasonography revealed that he had a fatty liver. Therefore, metabolic syndrome was diagnosed. Thereafter, diet (cholesterol <200 mg/day) and exercise (walking 30 minutes/day) therapy was initiated.
Body and Laboratory Parameters.

In November 2013, he agreed to measure intact proinsulin and PI/I ratio in our study. 1 In the present case, prominent hyperproinslinemia was detected by chance. His intact proinsulin level, PI/I ratio, and fasting blood glucose were 44.5 pmol/L (1.9-7.0), 1.4 (0.04-0.31), and 108 mg/dL respectively (Table 2). Five months later, his intact proinsulin level, PI/I ratio, and fasting blood glucose were 167 pmol/L, 0.6, and 147 mg/dL, respectively. In September 2014, a 75 g oral glucose tolerance test (OGTT) showed that his glucose tolerance was impaired accompanied by a marked elevation of total insulin and C-peptide (Table 3). His homeostasis model assessment (HOMA) −R (2.5°C) was 2.68. On the other hand, his HOMA-β was 50.5 (50%-120%). Therefore, insulin resistance was found. His glycosylated hemoglobin was also 6.9%. Thus, he was diagnosed as having type 2 diabetes mellitus. No diabetic complications were found. Therefore, diet (1800 kcal/day) and exercise therapy were continued. However, his hyperproinslinemia and diabetes mellitus remained. Therefore, aloguliptin was started to recover insulin secretion in November 2014. Thereafter, pioglitazone was added to improve insulin resistance. Finally, luseogliflozin was started to for its glucose-lowering effects. Thereafter, his HbA1c was stabilized (Figure 1).
75g oral glucose tolerance test.
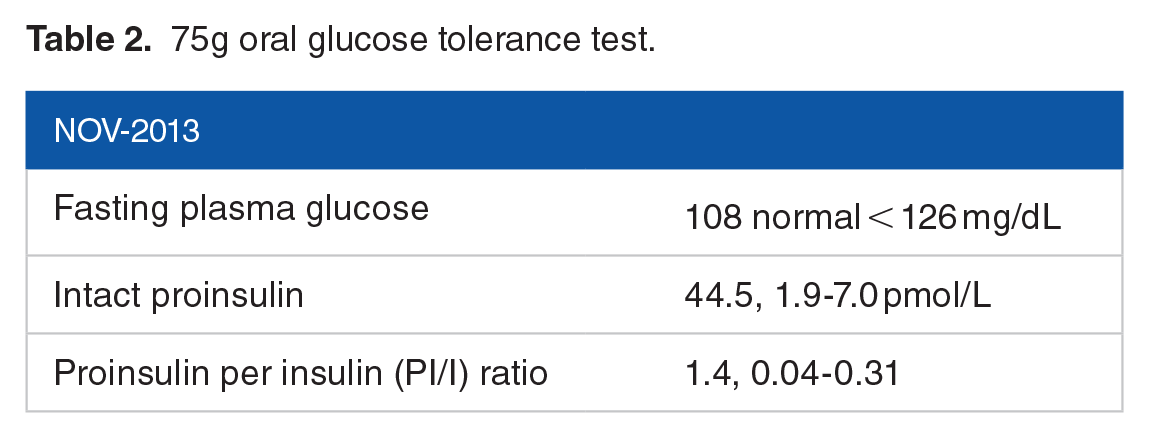
Intact proinsulin and PI/I ratio in Nov/2013.


Intact proinsulin, proinsulin per insulin (PI/I) ratio, and glycosylated hemoglobin, by year of outpatient clinic. After initiation of medication, intact proinsulin was dropped, whereas PI/I ratio remains relatively constant.
Discussion
In our ongoing study, we detected a case of prominent hyperinsulinemia in a middle-aged patient. To the best of our knowledge, there have been few reports of patients with hyperproinsulinemia. Ohashi et al 6 reported that familial hyperproinsulinemia was associated with diabetes mellitus. In the present case, only the patient’s mother was diagnosed with diabetes mellitus.
Insulin is synthesized in the beta-cells from preproinsulin. Preproinsulin becomes proinsulin after leaving the signal peptide. Proinsulin is separated into C-peptide and insulin by 2 enzymes, prohormone convertase 1/3 and 2. 7 Hyperproinsulinemia is suspected to be a pancreatic β-cell defect that is augmented by the increased demand placed on the beta-cell by hyperglycemia. 7
A disproportionate elevation of proinsulin relative to insulin in non-diabetic patients has been shown to predict the development of type 2 diabetes mellitus in patients at risk for the development of the disease. 8 In both middle-aged (50.8 ± 10.4 years) diabetic subjects (BMI 28.6 ± 7.2, HbA1c 7.8 ± 1.5%) and middle-aged (46.6 ± 13.0 years) non-diabetic subjects (BMI 29.7 ± 7.9), intact proinsulin and PI/I ratio of diabetic subjects were higher than non-diabetic subjects (intact proinsulin 13.5 ± 13.0 vs 6.4 ± 9.1 pmol/L, P = .003; PI/I 0.16 ± 0.15 vs 0.09 ± 0.09, P = .003). 1 In comparison, this patient’s intact proinsulin and PI/I ratio were as high as 44.5 pmol/L and 1.4. Thus, he had prominent hyperproinsulinemia. We hypothesize the patient’s proinsulin processing system was deteriorated. Therefore, insulin resistance was revealed in the present case. According to Then et al, 9 PI/I ratio was positively associated with prevalent and incident type 2 diabetes mellitus. PI/I ratio might serve as a biomarker for type 2 diabetes mellitus risk independently of the metabolic syndrome. Proinsulin alone was strongly and directly associated with all components of the metabolic syndrome. The metabolic syndrome including insulin resistance might have exacerbated the insulin processing defect and thus increased the PI/I in the present case. Hence, the hyperinsulinemia is also associated with metabolic condition in the present case. Therefore, we prescribed pioglitazone to improve insulin resistance. Thereafter luseogliflozin was started expecting its glucose-lowering effects without stimulating insulin secretion. His HbA1c was not deteriorated. A prospective follow-up of the present case is now underway.
Conclusion
We describe a case of prominent hyperproinsulinemia in a middle age patient. Insulin resistance was present and was suspected to aggravate the hyperproinsulinemia. Therefore, we started medication to reduce insulin resistance, but without effect on the HbA1c.
When physicians face treatment resistance in diabetes mellitus, we emphasize that evaluation of proinsulin should be considered as one of the methods.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Contributions
HY was responsible for database search and writing of the article. KK, KY and GY were responsible for correction of the article and supervision. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Informed Consent
Informed consent of the case report was obtained from the patient for publication of this case report.