
Abstract
Paratubal cysts may mimic ovarian cysts, and most of them are diagnosed postoperatively. They originate from the mesosalpinx between the ovary and the fallopian tube. Only a few are large, and most paratubal cysts are less than 10 cm. We report a huge paratubal cyst in a 30-year-old woman, whose only preoperative complaint was abdominal distention over 4 months. Conservative surgery was performed with cyst removal while preserving the ovaries and tubes. A paratubal cyst should be included in the differential diagnosis of a large pelvic masses, especially in the reproductive age.
Introduction
Adnexal cysts may arise from ovarian and fallopian tube tissues. A paratubal cyst is a type of adnexal cyst that originates from the mesothelium in the large ligament between the fallopian tube and the ovary; it accounts for 10% of all adnexal masses. 1 Most cases of paratubal cysts are misdiagnosed as ovarian cysts and are suspected in just 1 of 15 patients before surgery. 1 Their mean size has been reported to be 7.51 cm; only 12.96% are larger than 10 cm. 2 Only a few cases of giant para tubal cysts (>20 cm) have been published, and all cases have had different approaches and histopathological types.3-8 We report a case of a giant para tubal cyst mimicking an ovarian cyst in a 30-year-old woman and provide some representative images along with a literature review. The cyst was managed with surgical removal while preserving the adnexa; the final postoperative diagnosis was that of a benign paratubal cyst.
Case Report
A 30-year-old woman visited the outpatient clinic seeking treatment for abdominal distention present since the last 4 months. She had no history of surgery. Bowel and bladder functions were normal. Menstruation was regular and without any pain. The patient was nulliparous. Computed tomography (CT) scan with contrast showed a thin walled unilocular cyst arising from the left adnexa with dimensions of 22.3 cm × 18.4 cm × 6.8 cm; no papillary projections or nodules were observed (Figure 1). The Ca 125 level was 13.64 U/mL.

A computed tomography scan showing a thin-walled, unilocular cyst without any papillary projections or nodules.
Because of the large size of the cyst and the patient’s preference, a laparotomy was performed. We performed a midline incision above the umbilicus, trying to exteriorize the cyst without any rupture. Intraoperative exploration showed a large, thin-walled, unilocular cyst arising from the left para-tubal tissue without any adhesions; the left tube and left ovary were normal (Figure 2). The para tubal cyst was dissected to separate it from the normal ovary and tube (Figure 3). The para tubal cyst was removed and sent for histopathological examination (Figure 4). The left tube and left ovary were preserved (Figure 5). The uterus and right adnexa were normal. Frozen section examination confirmed by final histopathological examination revealed a benign serous cyst of size 22 cm × 17 cm × 6 cm.
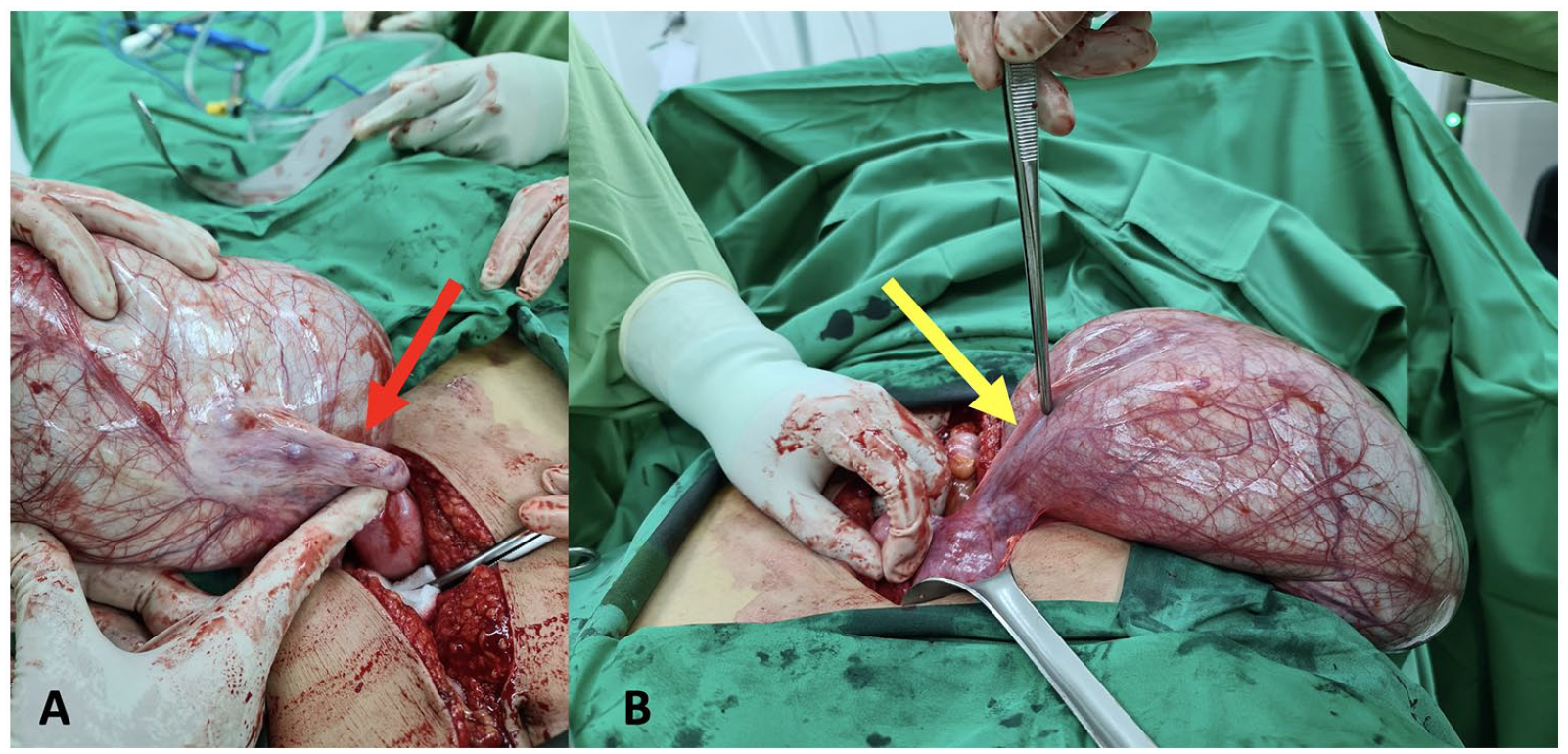
(A) A view from the above showing a large left paratubal cyst with a normal left ovary (red arrow) and (B) a view from below showing a left sided, smooth-surfaced, paratubal cyst with normal left tube (yellow arrow).

Dissection of the left paratubal cyst was performed to separate the cyst from the normal left ovary (red arrow) and left tube (yellow arrow).

A huge left paratubal cyst was removed.

The left tube and left ovary were preserved.
Written, informed consent was obtained from the patient for the publication of this report and its accompanying images (Table 1).
Large paratubal cases.

Discussion
A paratubal cyst is a cyst that originates from the mesosalpinx between the ovary and the fallopian tube and may arise from the mesothelium, mesonephric, or paramesonephric (Mullerian) tissues. 4 The duct shrinks as the fetus starts to develop female sex organs. Occasionally, remnants of the duct can be found and may grow into a paratubal cyst. The vestiges of the paramesonephric (Mullerian) duct may also form cysts. Para ovarian cysts and paratubal cysts are the same and are used to describe cysts that arise from the tissue between the ovary and fallopian tube.2,5,11 Para tubal cysts have been found in 7.3% of pediatric and adolescent populations. 12 The incidence in the general population is estimated to be around 3%, with the third and fourth decades being the peak age of recurrence. 5 The majority of paratubal cysts occur in the reproductive age, and only 6.25% of paratubal cysts occur in postmenopausal age. 13 Most paratubal cysts are asymptomatic unless they have already enlarged significantly. The patient in our case did not have symptoms until she experienced abdominal distension over 4 months. Paratubal cysts may cause complications if they undergo torsion and rupture.
Most paratubal cysts are diagnosed intraoperatively. Only 1 in 15 patients are diagnosed preoperatively. 1 One report showed that 307 patients did not have a paratubal cyst ultrasonographically, but finally, 298 had a paratubal cyst confirmed surgically. 14 Most paratubal cysts appear as thin-walled unilocular cysts with smooth borders. On CT, benign paratubal cysts appear as thin-walled unilocular cysts with a smooth capsule containing clear fluid.3,8,15 On magnetic resonance imaging, benign paratubal cysts appear as a thin-walled unilocular cyst with smooth borders. 5 Imaging of non-benign paratubal cysts may show intramural solid nodules, papillary projections, or a septum inside the cyst.5,16,17 A CT scan in our case showed a thin-walled unilocular cyst with smooth borders, without solid nodules, papillary projections or a septum, and histopathological examination confirmed the diagnosis of a benign paratubal cyst.
The majority of paratubal cysts are benign. 5 However, there have been several reports where paratubal cysts were borderline or malignant.10,18,19 As the incidence of malignancy in paratubal cases is very low, there is no reliable data regarding the efficacy of Ca 125 levels in predicting a malignancy in patients with paratubal cysts. Age, gross appearance, size, septation, and Ca 125 levels are all weak indicators of malignancy. 2 Hence, frozen sections should be checked intraoperatively to confirm the malignancy status of the paratubal cyst, especially when there is a papillary projection inside the cyst. Papillary projections growing from the cyst wall are ultrasound findings that are suspicious of malignancy of paratubal cysts. 20 In our case, no papillary projections were observed and the frozen section result was in concordance with the final histopathological examination, which showed a benign serous cyst.
The low incidence of paratubal cysts has led to a lack of standard consensus on their management. Some paratubal cysts are removed laparoscopically, while several others are removed via laparotomy.2-5 There are no standard criteria for laparoscopy or laparotomy. The size of the cyst, patient’s preference, and cyst rupture concern were the reasons for deciding on a laparotomy in our case. Intraoperative management are varies between cystectomy, cystectomy plus salpingectomy, and adnexectomy.2,3,21 The majority undergo a cystectomy for a paratubal cyst. 2 The patient in our case underwent paratubal cystectomy and preservation of the ovary and the fallopian tube. Paratubal cysts commonly occur in the reproductive age when fertility is still necessary; hence, conservative surgery preserving tubes and ovaries should be the first consideration. Intraoperatively, careful exploration should be performed to confirm the origin of the cyst, and misdiagnosis as a large ovarian cyst and subsequent adnexectomy should be avoided. Most para-tubal cysts are benign, and only a few are borderline.9,10,16,21 The most common occurrence of a paratubal borderline tumor is among the elderly.9,10
This case suggests that a paratubal cyst should be included in the differential diagnosis of pelvic masses, especially in the reproductive age. A huge paratubal cyst may mimic a large ovarian cyst preoperatively and intraoperatively. Careful inspection during surgery is necessary to confirm a paratubal cyst. Cystectomy should be the first consideration in the management of paratubal cysts.
Footnotes
Funding:
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Data collection, manuscript writing and editing.
Ethics
In our institution, a case report does not require approval from ethic committee.
Patient’s Consent
A written and informed consent was obtained from the patient informing them about the publication of case and pictures in the journal.